Background and Objectives: Electronic health records (EHRs) have had mixed effects on the workflow of ambulatory primary care. In this study, we update previous research on the time required to care for patients in primary care clinics with EHRs.
Methods: We directly observed family physician (FP) attendings, residents, and their ambulatory patients in 982 visits in clinics affiliated with 10 residencies of the Residency Research Network of Texas. The FPs were purposely chosen to reflect a diversity of patient care styles. We measured total visit time, previsit chart time, face-to-face time, non-face time, out-of-hours EHR work time, and total EHR work time.
Results: The mean (SD) visit length was 35.8 (16.6) minutes, not counting resident precepting time. The mean time components included 2.9 (3.8) minutes working in the EHR prior to entering the room, 16.5 (9.2) minutes of face-to-face time not working in the EHR, 2.0 (2.1) minutes working in the EHR in the room (which occurred in 73.4% of the visits), 7.5 (7.5) minutes of non-face time (mostly EHR time), and 6.9 (7.6) minutes of EHR work outside of normal clinic operational hours (which occurred in 64.6% of the visits). The total time and total EHR time varied only slightly between faculty physicians, third-year and second-year residents. Multivariable linear regression analysis revealed many factors associated with total visit time including patient, physician, and clinic infrastructure factors.
Conclusions: Primary care physicians spent more time working in the EHR than they spent in face-to-face time with patients in clinic visits.
A survey by the Office of the National Coordinator for Health Information Technology in 2014 reported that 87% of primary care physicians used electronic health records (EHRs).1 Reviews of the effect of EHRs on patient and physician outcomes have been mixed, including neutral to small positive effects on common quality metrics and disease-specific guidelines,2-5 mixed on office workflow,2,6,7 and mostly decreased on primary care physician productivity.8-10 There is little to no evidence that patient outcomes are improved or overall health care costs are reduced.4,11
Major studies of the work US family physicians perform in their clinic have been published, but all before the national growth of EHRs.12-24 Although several studies of the impact of EHRs on physician work report an effect on time as a percentage of their work day, almost no previous studies measured the actual time spent. A recent study of four types of physicians found that 27% of their time was spent in clinical face-to-face time with the patient and 49% of their time was spent using the EHR and other deskwork.25 Heavy EHR use in primary care is associated with increased time pressure, increased physician stress, and decreased job satisfaction.26
Previous studies have shown that for a mostly middle-aged, insured population, family physicians address 2.5 to 3.1 issues in the average clinic visit.12,15,16 The average number of issues per visit grows to 3.9 to 6 for elderly patients and 4.6 for patients with diabetes.16,24 Multiple issues are not likely to get equal attention. Other research observed that primary care physicians in clinic only spend 1 minute on other patient concerns after the chief complaint is addressed.24 This time crunch is associated with reduced provision of common chronic disease services when multiple patient concerns are addressed.27
The purpose of our study was to update measures of the time primary care physicians require to care for ambulatory patients in clinics, to measure how much time was spent working in the EHR, and to determine the other patient, physician, and visit characteristics associated with these time measures.
Study Population
This was a cross-sectional, observational study in clinics of 10 family medicine residency programs that are members of the Residency Research Network of Texas (RRNeT).
Observer Training and Measurements
Visit observers/data collectors (“observers”) were medical students and one premed undergraduate student. Each volunteered to participate in a 4-week research elective during a normal break in their primary class schedule. Investigators scheduled a 1-day orientation and training session at the medical school in San Antonio to teach enrollment and consent procedures, and review all sections of the instrument. Prior to the training, one investigator filmed physician-patient interactions (both complex and simple visits) and used these during training so the observers could practice recording pertinent data. The investigator-trainers provided feedback to insure consistent data collection approaches among all observers.
This study used a visit survey to describe each patient’s visit in multiple domains. The primary instrument was based on the National Ambulatory Medical Care Survey (NAMCS), which includes the reason for visit, new or continuing/follow-up patient, patient demographics, diagnoses, screening services, exams, medicines, procedures, nonmedical treatments, and referral patterns.28 Unlike NAMCS, there were no numerical limits on any of the categories in our study.
Observers were instructed to record all concerns brought up in the visit by either the patient or physician. These could include symptoms, diagnoses, socioeconomic concerns, health care system issues, or even concerns about people other than the patient (for example, a question about a child’s health during an adult’s scheduled visit). These concerns were recorded in a section entitled Reasons for Visit (RFV), which mirrored the NAMCS instrument. Observers were also asked to record all of the concerns that were actually addressed by the physician during the visit (issues addressed), which also mirrors the NAMCS instrument. The investigator-trainers provided training on how to make this distinction during the session. For example, a patient may have mentioned a recent headache, but the physician spent no observed time taking a history of the headache or prescribing a medication for the headache. In this scenario, the headache would be recorded in the RFV section, but not the Issues Addressed (IA) section.
Observations
Patient-physician visits were purposely sampled at the level of the observed physician. A true randomization of physicians was impractical given the nature of their clinic schedules. However, observers were instructed to shadow as wide a variety of physicians as possible, and to preferentially observe FP faculty whenever possible, followed by third- or second-year residents. Data collection occurred in May and June 2015, toward the end of the academic year, which meant that observed residents had 2 and 3 full years of clinical experience.
Observers recorded data from alternate patient visits to allow time to complete the lengthy study instruments and to decrease the burden of their presence on the observed physician. Observers were instructed to be a “fly on the wall” and to impact the encounter as little as possible. They were instructed to move to the corner of the examination room that was the least visible to the patient. A crucial component of data collection was the time required for the physician to complete the encounter, both face-to-face time and non-face time. Observers were instructed to not make any statements or ask the physician any questions until he or she was finished with that visit, and was ready to see the next patient. While the physician was seeing the nonobserved patient, the observer would complete recording relevant data on paper copies of the instruments and await the next eligible patient. The observer would explain the nature of the study and seek verbal consent from the patient and furnish a 1-page informational letter (signed consent was not required). If the patient declined to be observed, the next eligible patient was approached. At the end of each half-day clinic session, the observer transferred the written data onto a web-based version of the instrument through Survey Monkey.
Time Measurement
Observers used personal watches or cell phones to record time data. If documentation and other administrative work was incomplete at the end of the clinic session, the observers asked the physician to estimate how much time he or she would spend documenting in the EHR for each patient outside of clinic hours. A study investigator followed up with each student to inquire about their judgment of whether the estimated times seemed reasonable and consistent given their observation of each physician’s documentation style and computer skills. Every observer reported that estimated times were consistent with observed behaviors and were unlikely to exaggerate the actual time spent.
Data Analysis
Results were analyzed using descriptive statistics. Group comparisons of continuous variables were assessed using independent samples t-tests or analysis of variance (ANOVA) as appropriate, and comparisons of all categorical data were analyzed using chi square. Bivariate correlation coefficients were calculated to identify variables that potentially predicted the time outcomes. Those that had a P value of < .20 were included in the multivariable linear regression models to identify independent predictors of time outcomes. SPSS (Statistical Package for the Social Scientist) version 20 was used for analysis (SPSS Inc., Chicago, IL). All tests were 2-tailed, and alpha levels were set at 0.05 to determine statistical significance.
The project was approved by the Institutional Review Board (IRB) at the University of Texas Health Science Center at San Antonio and each of the participating residencies.
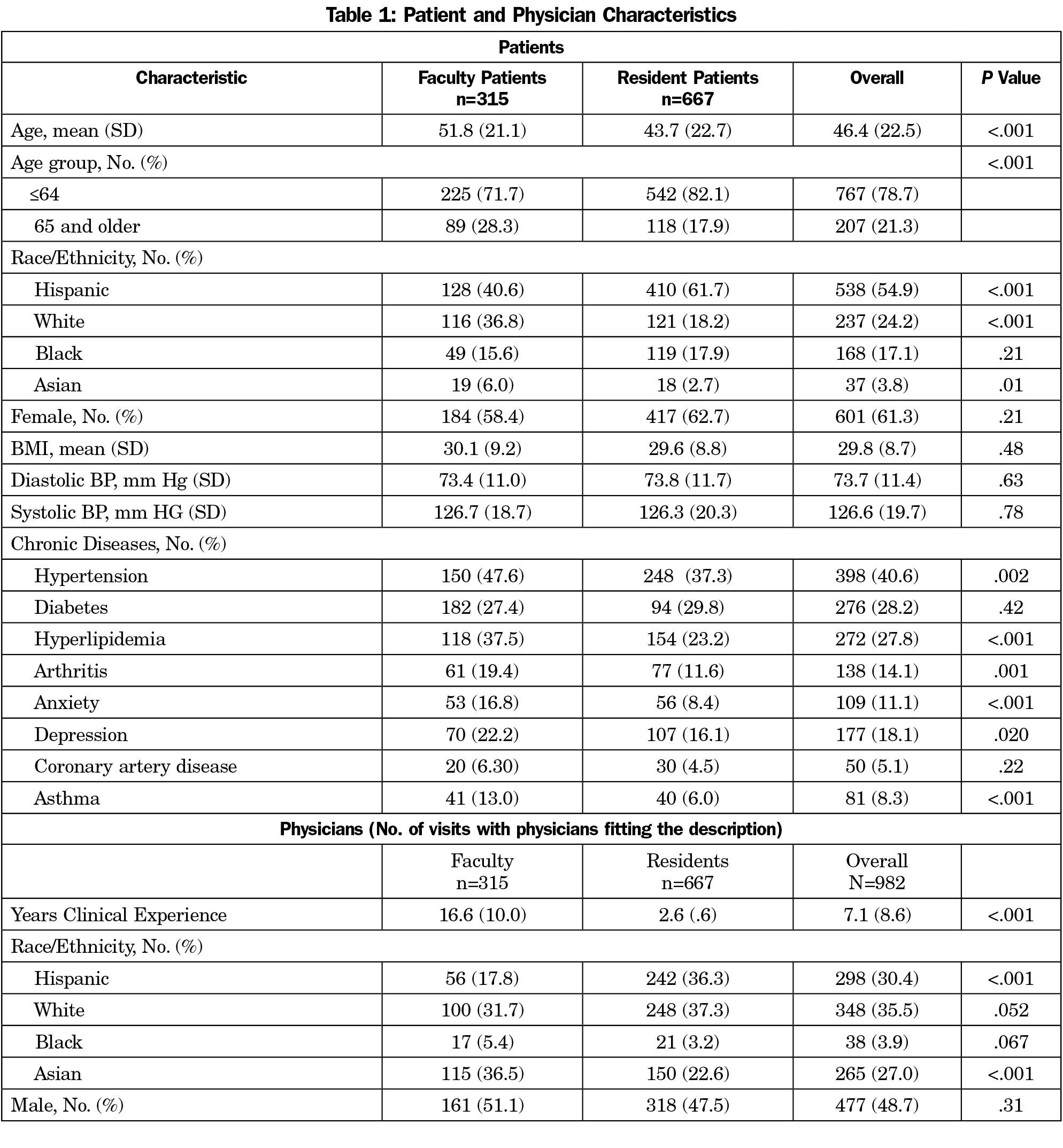
We observed 982 clinic visits. Characteristics of the patients and physicians are shown in Table 1.
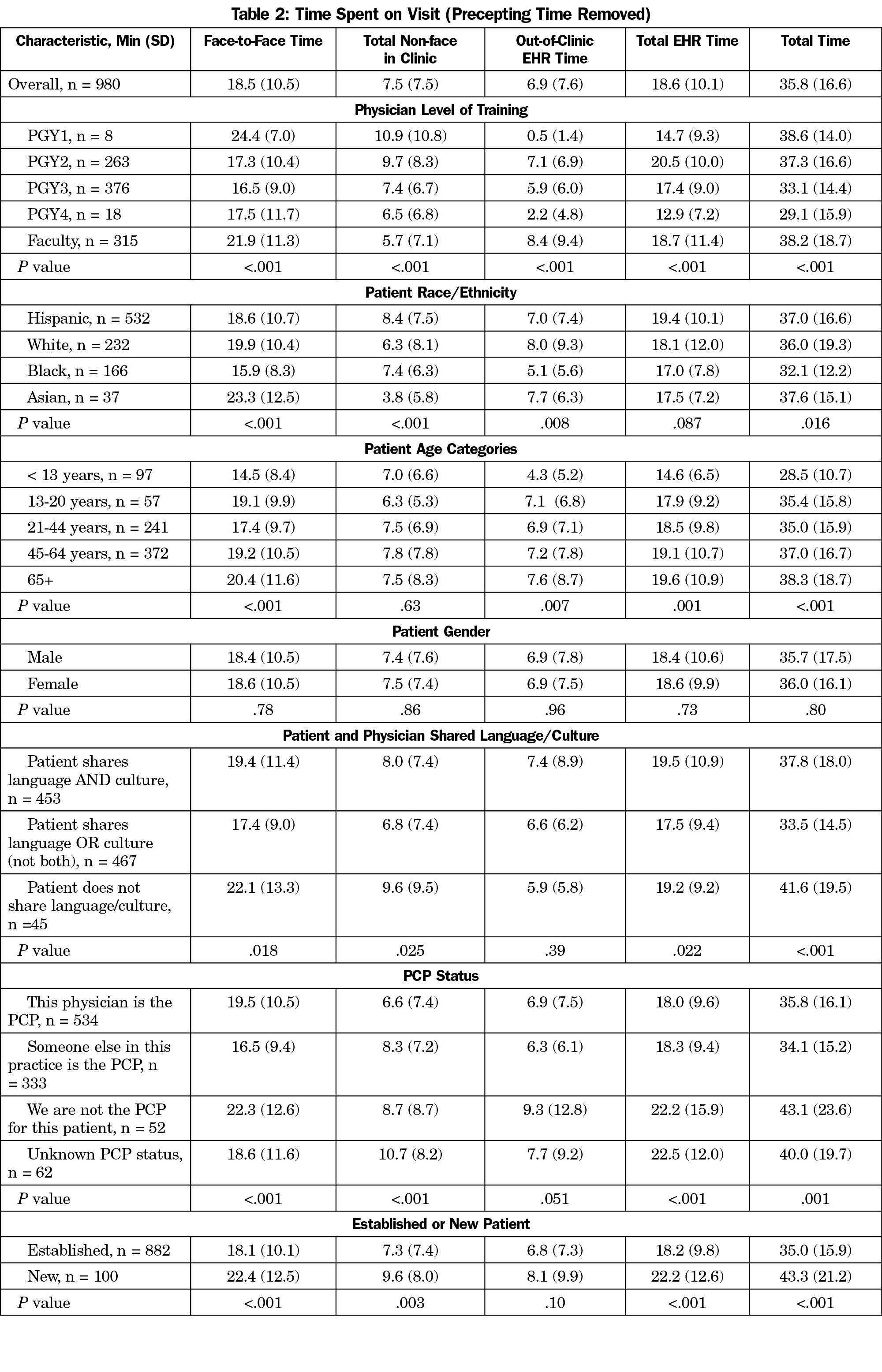
In 982 physician-patient visits, the mean (SD) visit length was 35.8 (16.6) minutes, not counting resident precepting time. The mean time components included 2.9 (3.8) minutes working in the chart prior to entering the room, 16.5 (9.2) minutes of face-to-face time not working in the EHR, 2.0 (2.1) minutes working in the EHR in the room, 7.5 (7.5) minutes of non-face time (mostly EHR time), and 6.9 minutes (7.6) of EHR work outside of normal clinic operational hours. The total estimated EHR time per visit was 18.6 minutes (corrected for estimated non-face/non-EHR time performing other tasks such as filling out forms).
The total time and total EHR time varied only slightly between faculty physicians, third- and second-year residents (38.2 [18.7], 33.1 [14.4], and 37.3 [16.6] minutes; 18.7 [11.4], 17.4 [9.0], and 20.5 [10.0] minutes, respectively, P<.001 for both comparisons, Table 2). Patients seeing faculty were older and raised more reasons for the visit than patients seeing residents. One faculty-only clinic had notably longer mean visit times even when corrected for factors such as patient demographics and the number of issues addressed per clinic visit. When it was removed from the analysis, the average faculty time was reduced by 3 minutes (35.3 [18.7] min, P=.01 for the different physician types). There was no consistent pattern of mean total EHR time by clinical experience, other than the longest time was spent by second year residents (20.4 minutes per visit, Table 3). In general, physicians who had completed residency training spent less previsit time and less EHR time, but more face-to-face time.
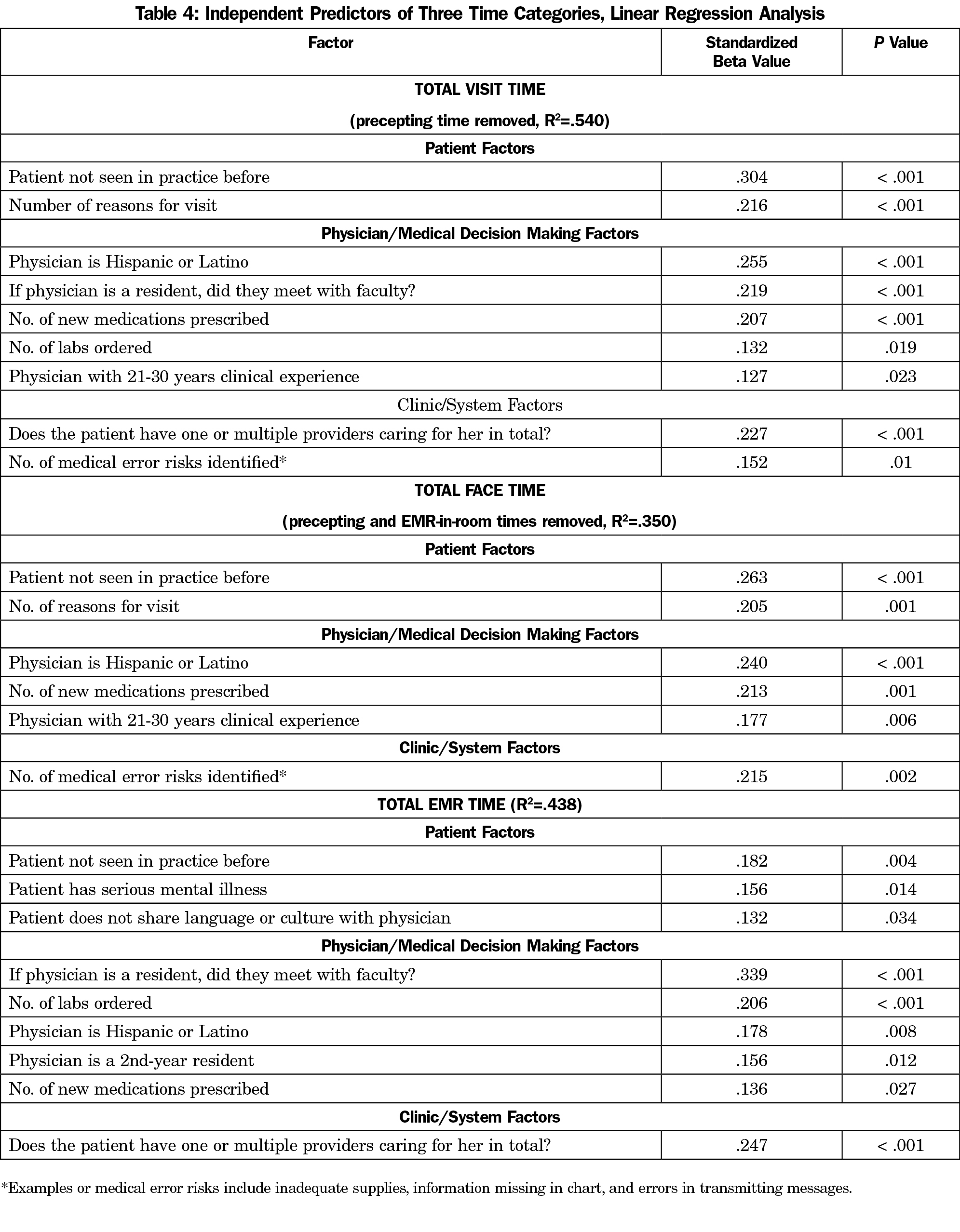
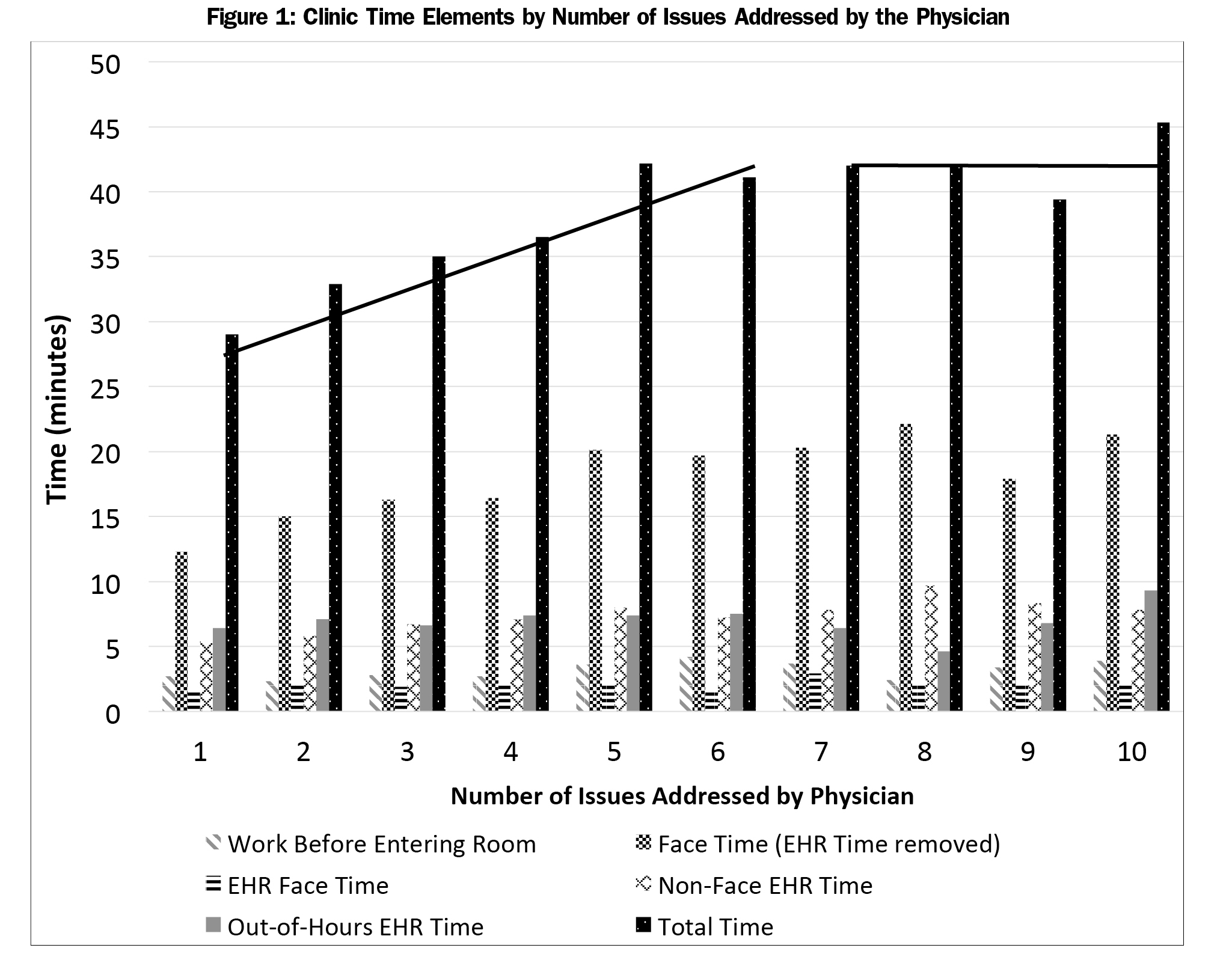
Multivariable linear regression analysis revealed many factors associated with visit times, including patient, physician, and clinic or system factors (Table 4). These times were adjusted to remove precepting time for patients seen by residents. The single largest contributor to total time and non-face time was still whether or not the resident checked out the patient with a preceptor. This factor did not impact face-to-face time with the patient. Other important contributors included if the patient was new to the practice and the number of reasons for the visit the patient stated. Time use as a function of the number of issues the physician addressed is shown in Figure 1. Two important notes apply to the figure First, the number of reasons for the visit and the number of issues the physician addressed were almost exactly colinear. Issues addressed is reported here for brevity. Secondly, in the linear regression, there was a significant interaction with a dummy variable at six to seven visits, which is why two separate linear regressions are shown. Other patient and physician factors were mostly noncontributory. Years of physician experience had little impact on any of the time measures.
We found that family physicians spent more time in direct ambulatory patient care working in the EHR than they spent in face-to-face time with their patients. The majority of family physicians worked through lunch, stayed late at clinic, or took their work home to complete the day’s EHR work. Significant predictors of visit length included the number of reasons for the visit, new patients to the practice, the number of medications prescribed, whether the physician was Hispanic, whether a resident physician presented the patient to an attending physician, whether the patient had one or multiple physicians caring for him or her, and a few other factors.
Our results of the time spent by the physicians working in the EHR are similar to a recent study that used EHR time stamp data from 471 primary care physicians.29 They found physicians logged an average of 3.08 hours on office visits and 3.17 hours on “desktop medicine” each day, which is similar to the ratio we measured. They also noted a trend from 2011 to 2014 of declining time allocated to face-to-face visits, accompanied by increasing time allocated to desktop medicine.
Our measurements of the face-to-face time are similar to previous studies from the pre-EHR era. Since the Center for Medicare and Medicaid Services Evaluation and Management rules were introduced, direct observational studies measured between 13.4 and 19.3 minutes of mean face-to-face time,15,17,18,23,24,30,31 which is similar to our result of 18.5 minutes. Our result is at the high end of this range, which may be explained by including resident physicians, additional EHR time in the exam room (2.0 minutes per visit), and more issues addressed per visit than most of the previous studies. All US results stand in contrast to a recent study in the UK, where the average general practitioner consultation included 9.5 minutes of face-to-face time and 3.3 minutes of EHR time.32 The UK results are consistent with observed consultation times across six countries in Europe in 2002 of 7.6 to 15.6 minutes total (overall mean, 10.7 minutes).33 Our results imply that US FPs spend more time working in the EHR than their European counterparts spend in the entire visit.
Strengths of our study included the direct observation of physician work and the comprehensive nature of our data collection. Potential weaknesses of our study include the fact that observers had 1 day of training, visits were not recorded to check for intraobserver agreement, time allocation was only kept to the minute (other studies broke down time into 15 second increments), observations included many residents and did not include physicians in private practice, and the ever-present Hawthorne effect. Further analysis (not fully reported here) found that most time or other related differences (eg, number of issues addressed) were explained by differences in patient demographics across the sites. Another weakness is that the times reported for working in the EHR outside of normal clinic hours were estimated, not observed directly. All observers believed the times estimated by the participating physicians were consistent with time elements they did observe, and that none of the physicians estimated times unrealistically. The mean out-of-hours time comprised only 19% of the total visit time.
Our study successfully captured the work performed by the physician for each observed patient. We did not attempt to capture physician work devoted to other patients not seen that day. A recent estimate was that 13% of a family physician’s time is spent coordinating care among different physicians and other health care providers, such as physical therapists and home health agencies.34 Other studies found that 39 to 45% of a family physician’s time is spent out of the exam room,21,30 and total work time not directly involved with a patient clinic visit consumed between 20 and 50% of a primary care physician’s time that is not compensated.21,35 This time includes activities such as fielding telephone calls, emails, prescription refills, and reviewing lab reports, imaging reports, and consultant reports.36
Previous researchers observed that for each additional problem addressed in clinic, the visit length increased by 1 to 2.5 minutes.15 These studies followed physicians in private practice who managed fewer problems per visit than in our study. Previous research has also found that inner-city patients, such as those seen in almost all our clinic sites, had more chronic medical problems and more problems evaluated per visit.37 Our results yielded a 2-slope relationship, where the total time increased by 2.6 minutes per additional issue the physician addressed up to six issues, then plateaued.
An unexpected finding was that an important independent predictor of total visit time and non-face time was whether a resident checked out the patient with an attending, even though precepting time was removed from the reported times. This could reflect that we should have attributed more time to precepting, that patient visits that were checked out to attendings were more complex than average and required more thought and time, or that the attending changed some of the residents’ assessments and plans.
Our findings have important economic implications for family physicians. The original studies led by Hsiao that led to the Resource-Based Relative Value Scale (RBRVS) used by the Center for Medicare and Medicaid Services to value physician work, were conducted at a time when there was less work performed between visits and before the current evaluation and management (E&M) rules were enacted.38 In Hsiao’s original studies, non-face time was estimated to be 29% of the total visit time for primary care E&M visits,39 and were based on telephone surveys of physicians.40 Our study found this figure to be 54% of the total visit time. Furthermore, in the Hsiao’s studies, hypothetical cases based on current procedural terminology (CPT) codes were used. However, there are no CPT codes that describe when a physician addresses more than three issues in a visit, nor are physicians allowed to submit more than one E&M CPT code per day for payment.38 This implies that the relative value weightings of the CPT codes should be recalculated to increase payment for the significant EHR work time required in today’s primary care.
Acknowledgments
RRNeT Investigators include Nina Torkelson, Jerry Kizerian, Ronya Green, David Edwards, Sunand Kallumadanda, and Tamara Armstrong.
The authors thank the medical student research volunteers: Tanner Campbell, Jade Law, Brenda Chavez, Clayton Bishop, Caroline Stephens, Nicholas Inman, Katie Molina, Tiffany Brown, Shannon Brougher, and Thomas Heydon.
Financial Support: This project was funded with the help of the Texas Academy of Family Physicians Foundation. The project described was also supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR001120. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflicts of Interest: Dr Young discloses that he is the sole owner of Sentire, LLC, which is developing a novel documentation, coding, and billing system for primary care. All other authors report no conflicts.
Prior presentations: This study was presented at NAPCRG 2017 Annual Meeting, Nov 17-21, 2016, Montreal, Quebec, Canada.
References
- Heisey-Grove D, Patel V. Any, Certified, and Basic: Quantifying Physician EHR Adoption through 2014. ONC Data Brief. September 2015. https://www.healthit.gov/sites/default/files/briefs/oncdatabrief28_certified_vs_basic.pdf. Accessed Nov 2, 2016.
- Lau F, Price M, Boyd J, Partridge C, Bell H, Raworth R. Impact of electronic medical record on physician practice in office settings: a systematic review. BMC Med Inform Decis Mak. 2012;12(1):10.
https://doi.org/10.1186/1472-6947-12-10.
- Jones SS, Rudin RS, Perry T, Shekelle PG. Health information technology: an updated systematic review with a focus on meaningful use. Ann Intern Med. 2014;160(1):48-54.
https://doi.org/10.7326/M13-1531.
- Jamal A, McKenzie K, Clark M. The impact of health information technology on the quality of medical and health care: a systematic review. Health Inf Manag. 2009;38(3):26-37.
https://doi.org/10.1177/183335830903800305.
- Crosson JC, Ohman-Strickland PA, Cohen DJ, Clark EC, Crabtree BF. Typical electronic health record use in primary care practices and the quality of diabetes care. Ann Fam Med. 2012;10(3):221-227.
https://doi.org/10.1370/afm.1370.
- McDonald CJ, Callaghan FM, Weissman A, Goodwin RM, Mundkur M, Kuhn T. Use of internist’s free time by ambulatory care Electronic Medical Record systems. JAMA Intern Med. 2014;174(11):1860-1863.
https://doi.org/10.1001/jamainternmed.2014.4506.
- Howard J, Clark EC, Friedman A, et al. Electronic health record impact on work burden in small, unaffiliated, community-based primary care practices. J Gen Intern Med. 2013;28(1):107-113.
https://doi.org/10.1007/s11606-012-2192-4.
- Fleming NS, Becker ER, Culler SD, et al. The impact of electronic health records on workflow and financial measures in primary care practices. Health Serv Res. 2014;49(1 Pt 2):405-420.
https://doi.org/10.1111/1475-6773.12133.
- Adler-Milstein J, Huckman RS. The impact of electronic health record use on physician productivity. Am J Manag Care. 2013;19(10 Spec No):SP345-352.
- Rudin RS, Motala A, Goldzweig CL, Shekelle PG. Usage and effect of health information exchange: a systematic review. Ann Intern Med. 2014;161(11):803-811.
https://doi.org/10.7326/M14-0877.
- O’Reilly D, Tarride JE, Goeree R, Lokker C, McKibbon KA. The economics of health information technology in medication management: a systematic review of economic evaluations. J Am Med Inform Assoc. 2012;19(3):423-438.
https://doi.org/10.1136/amiajnl-2011-000310.
- Stange KC, Zyzanski SJ, Jaén CR, et al. Illuminating the ‘black box’. A description of 4454 patient visits to 138 family physicians. J Fam Pract. 1998;46(5):377-389.
- Horner RD, Paris JA, Purvis JR, Lawler FH. Accuracy of patient encounter and billing information in ambulatory care. J Fam Pract. 1991;33(6):593-598.
- Kikano GE, Goodwin MA, Stange KC. Evaluation and management services. A comparison of medical record documentation with actual billing in community family practice. Arch Fam Med. 2000;9(1):68-71.
https://doi.org/10.1001/archfami.9.1.68.
- Flocke SA, Frank SH, Wenger DA. Addressing multiple problems in the family practice office visit. J Fam Pract. 2001;50(3):211-216.
- Beasley JW, Hankey TH, Erickson R, et al. How many problems do family physicians manage at each encounter? A WReN study. Ann Fam Med. 2004;2(5):405-410.
https://doi.org/10.1370/afm.94.
- Bindman AB, Forrest CB, Britt H, Crampton P, Majeed A. Diagnostic scope of and exposure to primary care physicians in Australia, New Zealand, and the United States: cross sectional analysis of results from three national surveys. BMJ. 2007;334(7606):1261.
https://doi.org/10.1136/bmj.39203.658970.55.
- Mechanic D, McAlpine DD, Rosenthal M. Are patients’ office visits with physicians getting shorter? N Engl J Med. 2001;344(3):198-204.
https://doi.org/10.1056/NEJM200101183440307.
- Binns HJ, Lanier D, Pace WD, et al; Primary Care Network Survey (PRINS) Participants. Describing primary care encounters: the Primary Care Network Survey and the National Ambulatory Medical Care Survey. Ann Fam Med. 2007;5(1):39-47.
https://doi.org/10.1370/afm.620.
- Gilchrist VJ, Stange KC, Flocke SA, McCord G, Bourguet CC. A comparison of the National Ambulatory Medical Care Survey (NAMCS) measurement approach with direct observation of outpatient visits. Med Care. 2004;42(3):276-280.
https://doi.org/10.1097/01.mlr.0000114916.95639.af.
- Gottschalk A, Flocke SA. Time spent in face-to-face patient care and work outside the examination room. Ann Fam Med. 2005;3(6):488-493.
https://doi.org/10.1370/afm.404.
- Parchman ML, Romero RL, Pugh JA. Encounters by patients with type 2 diabetes--complex and demanding: an observational study. Ann Fam Med. 2006;4(1):40-45.
https://doi.org/10.1370/afm.422.
- Parchman ML, Pugh JA, Romero RL, Bowers KW. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5(3):196-201.
https://doi.org/10.1370/afm.679.
- Tai-Seale M, McGuire TG, Zhang W. Time allocation in primary care office visits. Health Serv Res. 2007;42(5):1871-1894.
https://doi.org/10.1111/j.1475-6773.2006.00689.x.
- Sinsky C, Colligan L, Li L, et al. Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties. Ann Intern Med. 2016;165(11):753-760.
https://doi.org/10.7326/M16-0961.
- Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc. 2014;21(e1):e100-e106.
https://doi.org/10.1136/amiajnl-2013-001875.
- Fenton JJ, Von Korff M, Lin EH, Ciechanowski P, Young BA. Quality of preventive care for diabetes: effects of visit frequency and competing demands. Ann Fam Med. 2006;4(1):32-39.
https://doi.org/10.1370/afm.421. PMID:16449394.
- Centers for Disease Control and Prevention. Questionnaires, Datasets, and Related Documentation. http://www.cdc.gov/nchs/ahcd/ahcd_questionnaires.htm. Accessed Feb 25, 2016.
- Tai-Seale M, Olson CW, Li J, et al. Electronic health record logs indicate that physicians split time evenly between seeing patients and desktop medicine. Health Aff (Millwood). 2017;36(4):655-662.
https://doi.org/10.1377/hlthaff.2016.0811.
- Gilchrist V, McCord G, Schrop SL, et al. Physician activities during time out of the examination room. Ann Fam Med. 2005;3(6):494-499.
https://doi.org/10.1370/afm.391.
- Pizziferri L, Kittler AF, Volk LA, et al. Primary care physician time utilization before and after implementation of an electronic health record: a time-motion study. J Biomed Inform. 2005;38(3):176-188.
https://doi.org/10.1016/j.jbi.2004.11.009.
- Hayward J, Buckingham S, Thomson F, et al. “How long does it take?” A mixed methods evaluation of computer-related work in GP consultations. J Innov Health Inform. 2015;22(4):409-425.
https://doi.org/10.14236/jhi.v22i4.95.
- Deveugele M, Derese A, van den Brink-Muinen A, Bensing J, De Maeseneer J. Consultation length in general practice: cross sectional study in six European countries. BMJ. 2002;325(7362):472.
https://doi.org/10.1136/bmj.325.7362.472.
- Bodenheimer T. Coordinating care--a perilous journey through the health care system. N Engl J Med. 2008;358(10):1064-1071.
https://doi.org/10.1056/NEJMhpr0706165.
- Chen MA, Hollenberg JP, Michelen W, Peterson JC, Casalino LP. Patient care outside of office visits: a primary care physician time study. J Gen Intern Med. 2011;26(1):58-63.
https://doi.org/10.1007/s11606-010-1494-7.
- Baron RJ. What’s keeping us so busy in primary care? A snapshot from one practice. N Engl J Med. 2010;362(17):1632-1636.
https://doi.org/10.1056/NEJMon0910793.
- Blankfield RP, Goodwin M, Jaén CR, Stange KC. Addressing the unique challenges of inner-city practice: a direct observation study of inner-city, rural, and suburban family practices. J Urban Health. 2002;79(2):173-185.
https://doi.org/10.1093/jurban/79.2.173.
- Johnson SE, Newton WP. Resource-based relative value units: a primer for academic family physicians. Fam Med. 2002;34(3):172-176.
- Hsiao W, Braun P, Dunn D, et al. A National Study of Resource-Based Relative Value Scales for Physician Services: Phase II Final Report to the Health Care Financing Administration. Boston, MA: Harvard School of Public Health; 1990. HCFA contract, 18-C-98795/1-03.
- Dunn D, Hsiao WC, Ketcham TR, Braun P. A method for estimating the preservice and postservice work of physicians’ services. JAMA. 1988;260(16):2371-2378.
https://doi.org/10.1001/jama.1988.03410160045006.



There are no comments for this article.