Background and Objectives: The University of Utah (UU) serves an increasingly diverse state and houses the only public medical school, dental school, and college of pharmacy in the state. Utah’s diversity in the health professions lags behind the diversity of its general population, and the nation.
Methods: The Health Sciences Learning, Engagement, Achievement, and Progress (HS-LEAP) Program is a 4-year undergraduate pipeline program intended to increase racial and ethnic diversity in the health professions, specifically focused on students underrepresented in medicine (URM). Each student self-identified and submitted demographics at the time of enrollment. We followed students to successful engagement in their profession of choice; we compared graduation and postgraduation outcomes to non-HS-LEAP students at UU from 2005-2016.
Results: Almost 80% of HS-LEAP students are from communities underrepresented in medicine: 41% Latinx, 28% Asian, 7% Black, 2% American Indian/Alaskan Native, and 1% Pacific Islander. HS-LEAP students had lower ACT scores upon undergraduate enrollment, higher grade point averages in their first semester of college, higher fall-to-fall first-year retention rates, and higher 6-year graduation rates when compared to non-HS-LEAP UU students. Students who completed HS-LEAP attended graduate school at twice the rate of students who participated in HS-LEAP, the majority in the health professions.
Conclusions: The HS-LEAP program is associated with increased URM success in undergraduate programs and elevated participation in graduate programs in medicine, dentistry, pharmacy, physician assistant, nursing, and public health. Similar programs, with continuous assessment and evaluation, could be adopted in other locations to improve the representation of these groups in health professions.
Black, Latinx, American Indian/Alaska Native, and Pacific Islander populations remain underrepresented in medicine (URM) and the health professions at levels far below their representation in the general population.1,2 The growing diversity of the US population necessitates increased diversity in the health professions as patients from URM communities often prefer health professionals who share their cultural background, and URM health professionals are more likely to serve URM communities.3 URM health professionals are also twice as likely to practice in the inner city and rural areas.4
Utah is home to a growing Latinx population (approximating 450,000, 14.2%)5, to part of the Navajo Nation, and the highest percentage of Pacific Islanders in any state outside of Hawaii. There are over 60,000 refugees in Utah, from Somalia, the Democratic Republic of Congo, Syria, Iraq, Vietnam, Myanmar, and other countries, with over 120 languages represented.6 In comparison, the most linguistically diverse community in the United States—Queens, New York—has 160 languages represented.7 The Utah physician workforce is 1.6% Latinx, 0.5% Black, 0.4% American Indian/Alaska Native, and 0.5% Pacific Islander.8 Overall, the other health professions face similar diversity challenges, especially pharmacy, dentistry, and physical therapy.9-11
University-based, diversity-focused pipeline programs can support racial/ethnic diversity in the medical workforce.12 The majority of these programs13-20 are research-focused summer programs that target specific skills and are designed to prepare for one specific branch of health care, usually medicine. We report on a unique pipeline program at the University of Utah that aims at increasing URM student entry into the health professions through an integrated curriculum designed to be a part of each of the undergraduate years.
Description
In 2001, the School of Medicine at the University of Utah launched a 4-year experiential learning program called Health Sciences Learning, Engagement, Achievement and Progress (HS-LEAP), to prepare URM students to be competitive for admission to health sciences graduate/professional programs. This program was based on an existing pipeline program at the University of Utah, founded in 1994, that has been described in detail in the literature.21 Ultimately, HS-LEAP sought to increase the number of URM health care professionals. URM was defined as students from American Indian/Alaska Native, Black, Latinx, Pacific Islander, Southeast or Refugee Asians, lower socioeconomic, and rural backgrounds.
Once accepted to the University of Utah, matriculating students may apply to HS-LEAP in the spring of their senior year in high school. Students are recruited from local and regional high schools, and the application is available online. Approximately 65 to 80 students apply each year. Applications are randomly assigned to be reviewed by one of four review teams. Each review team is comprised of one health sciences or HS-LEAP faculty, one senior staff member, and one HS-LEAP student graduate. Each team includes at least two members who identify as URM. From the most recent round of applicants, 40 positions were offered. Successful applicants included Black (15%), Asian (20%), Latinx (43%), American Indian/Alaska Native (5%), Pacific Islander (3%), and rural/lower SES (14%). Over 60% were first-generation college students, and 73% were women. Twenty-nine students enrolled in HS-LEAP in that year.
Students gather for a welcome day in the week before fall classes begin. There they meet the faculty member who teaches most of their HS-LEAP classes and their peer advisor, who will be with them throughout that first year. One peer advisor is competitively selected from the previous year’s HS-LEAP first-year students. Each peer advisor is hired for up to 20 hours per week and is registered for the second year HS-LEAP classes. The peer advisor also attends all of the first-year classes with the new students, as part of their employment. Peer advisors are an important link between new students and faculty, as students tend to be comfortable with near peers.22 The peer advisor serves as a mentor for HS-LEAP students throughout their 4-year HS-LEAP experience but is employed as such only during the second year of HS-LEAP.
The 4-year, 14 credit hour integrated curriculum is intended to provide building blocks and experiences that allow the student to engage in didactic, clinical, research, and community aspects of the health professions. In their first year, the students take two foundational classes that are both three credit hours per semester. In the fall, the course focuses on the care of underrepresented communities, research skill development, and documentation formats. In the spring semester, the course is an introduction to bioethics in which students can apply what they learned in the fall to the identification, study, and resolution or mitigation of conflicts among competing values or goals. These foundational courses also fulfill curricular requirements necessary for graduation. The second-year curriculum is devoted to experiential learning, with each student required to shadow a health professional in their area of interest for 20 hours. Accompanying this experience are classroom seminars given by various faculty experts regarding current social and political issues facing the health care system today. These topics include cultural literacy, integrative medicine, medical ethics, professionalism, and medical-legal considerations. The classroom seminars are taught over two semesters, each one for two credit hours. The third year is dedicated to a research experience in a UU lab. HS-LEAP students are hired by researchers for 10 hours per week, for two semesters. This activity is accompanied by a class (one credit) on conventions of scientific reporting each semester. HS-LEAP students spend their fourth year in a community engagement project and in a skill development (personal statements, applications, and interviewing) course (one credit each).
All HS-LEAP activities and coursework after the first year are in addition to the individual students’ major coursework, but some do fulfill general education requirements. Students who successfully complete all the above courses and activities are considered HS-LEAP graduates and receive a cord that can be worn with their graduation regalia.
Impact
Using enrollment data, we identified all students who participated in at least one semester of HS-LEAP and associated their college entry ACT score, which was obtained from admissions. Each ACT cohort was analyzed for the following outcomes: first-semester GPA, first-year fall-to-fall retention rates, 6-year graduation rates, completion of HS-LEAP program, entry and completion of graduate education. Each student is assigned a University ID number, that was used to search our databases for those HS-LEAP participants who did not continue in HS-LEAP until completion of the program. All other HS-LEAP participants were enrolled in our programs until graduation. We also used those data to calculate the percentage of HS-LEAP students who participated in all four years of HS-LEAP.
In addition to the above outcomes, we calculated HS-LEAP entry into the health professions with a graduate degree. All rates and calculations were stored in Microsoft Excel. The data and statistical analysis for all comparisons were provided by one of the authors (M.M.) at the Office of Budget and Institutional Analysis (OBIA) of the University of Utah, using the IBM SPSS Statistics program (Poughkeepsie, NY). The University of Utah Institutional Review Board determined this study to be exempt from oversight..
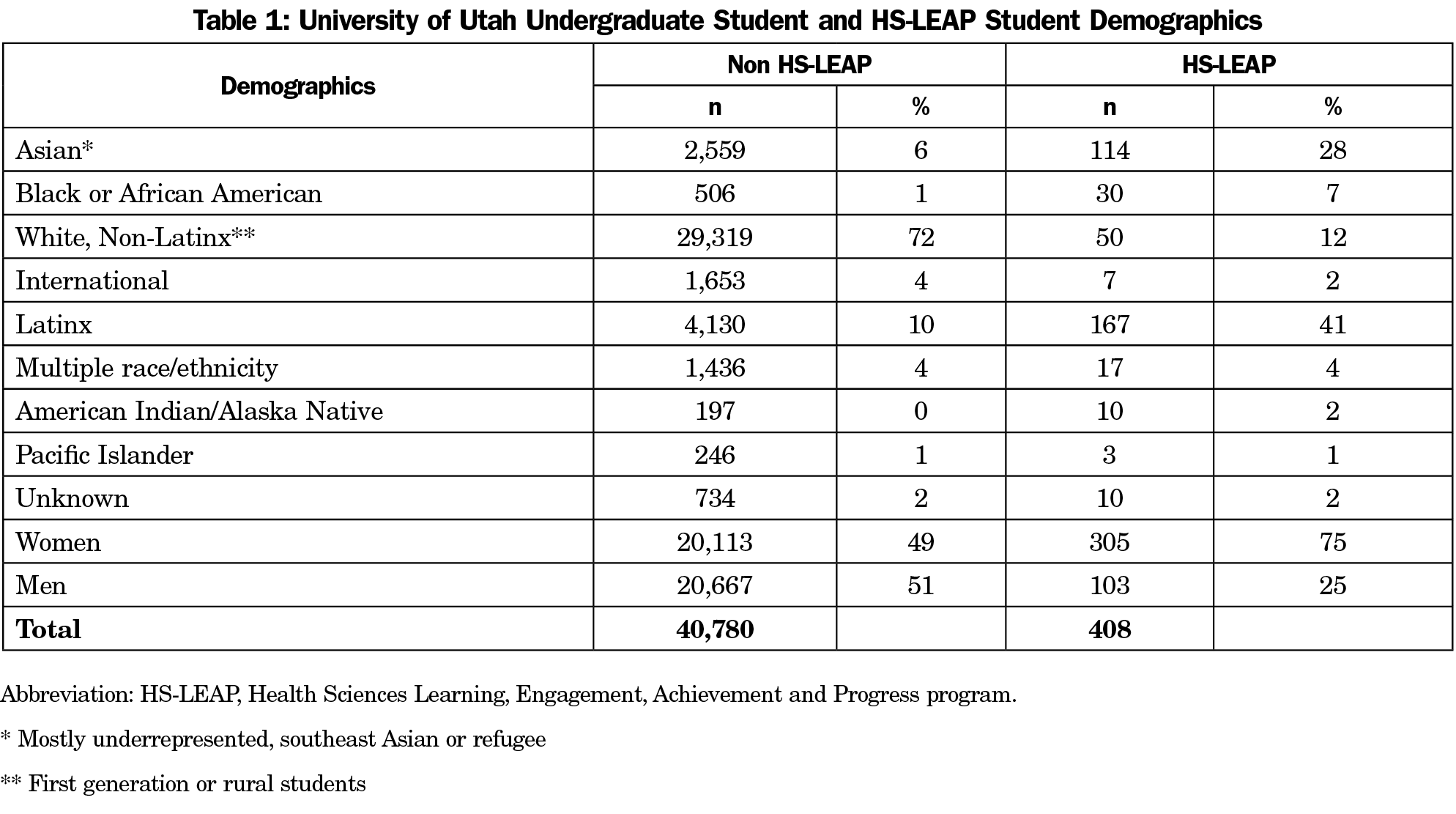
Four hundred eight students participated in HS-LEAP since 2005. Table 1 shows demographic data of the participants. Of note, almost 80% of the students in HS-LEAP are URM, and 75% are women. By individual groups, HS-LEAP has seven times the representation of Black students, four times the representation of Asian, Latinx, and American Indian/Alaska Native students when compared to the overall UU student population. The White, non-Latinx student representation in HS-LEAP is one-sixth of that demographic representation in the overall UU population. In terms of URM status, 79% of HS-LEAP students are from URM backgrounds, compared to 18% of overall UU students.
HS-LEAP students have typically entered the program with ACT scores lower than those of other first-year students (Figure 1).
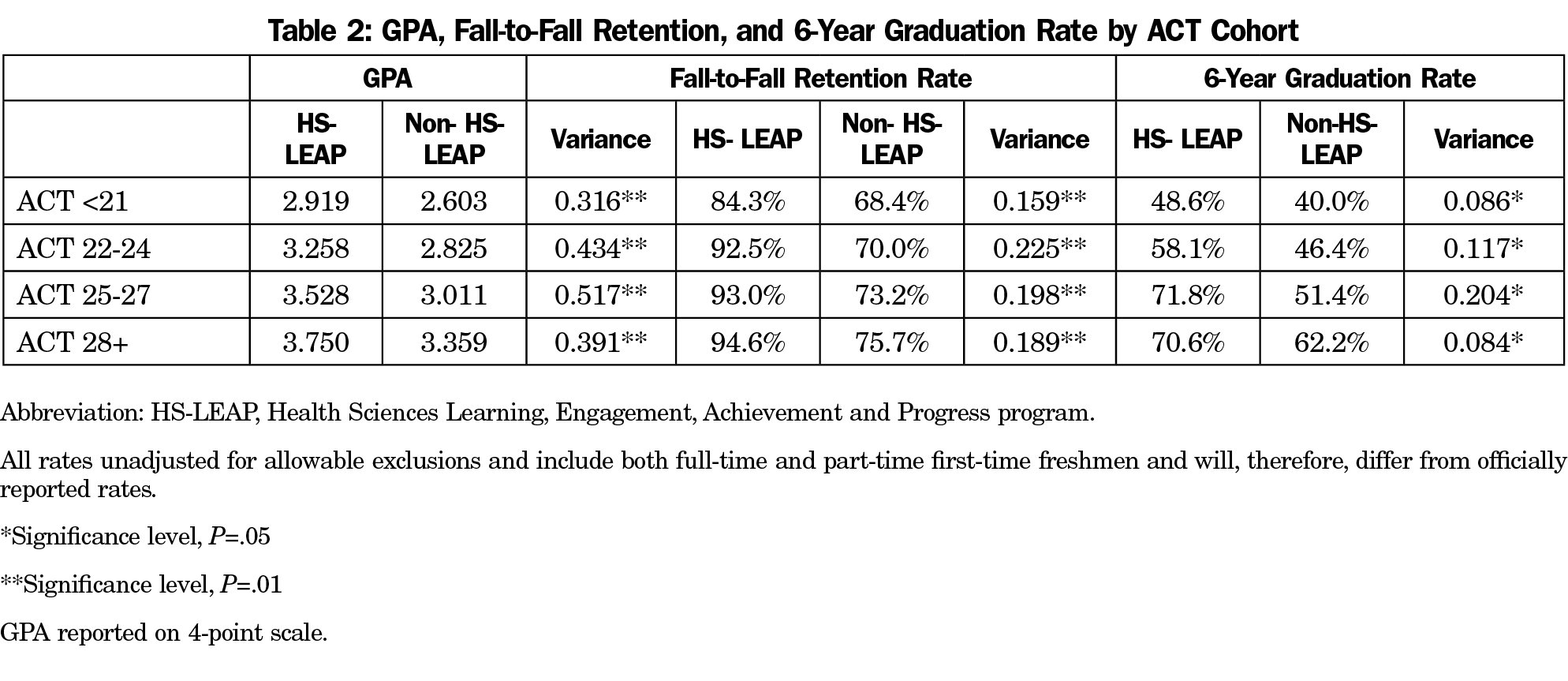
Although controversial, standardized test scores (including the ACT) have been used as both predictors of academic success as well as a measure of student expectations.23 The University of Utah uses the ACT score as a part of their admissions process. We found that at every ACT level, HS-LEAP students achieve higher GPAs in the first semester, higher fall-to-fall retention rates, as well as higher 6-year graduation rates when compared to their non-HS-LEAP peers. Thirty-eight percent of students who start HS-LEAP continue on to earn their HS-LEAP graduation cord.
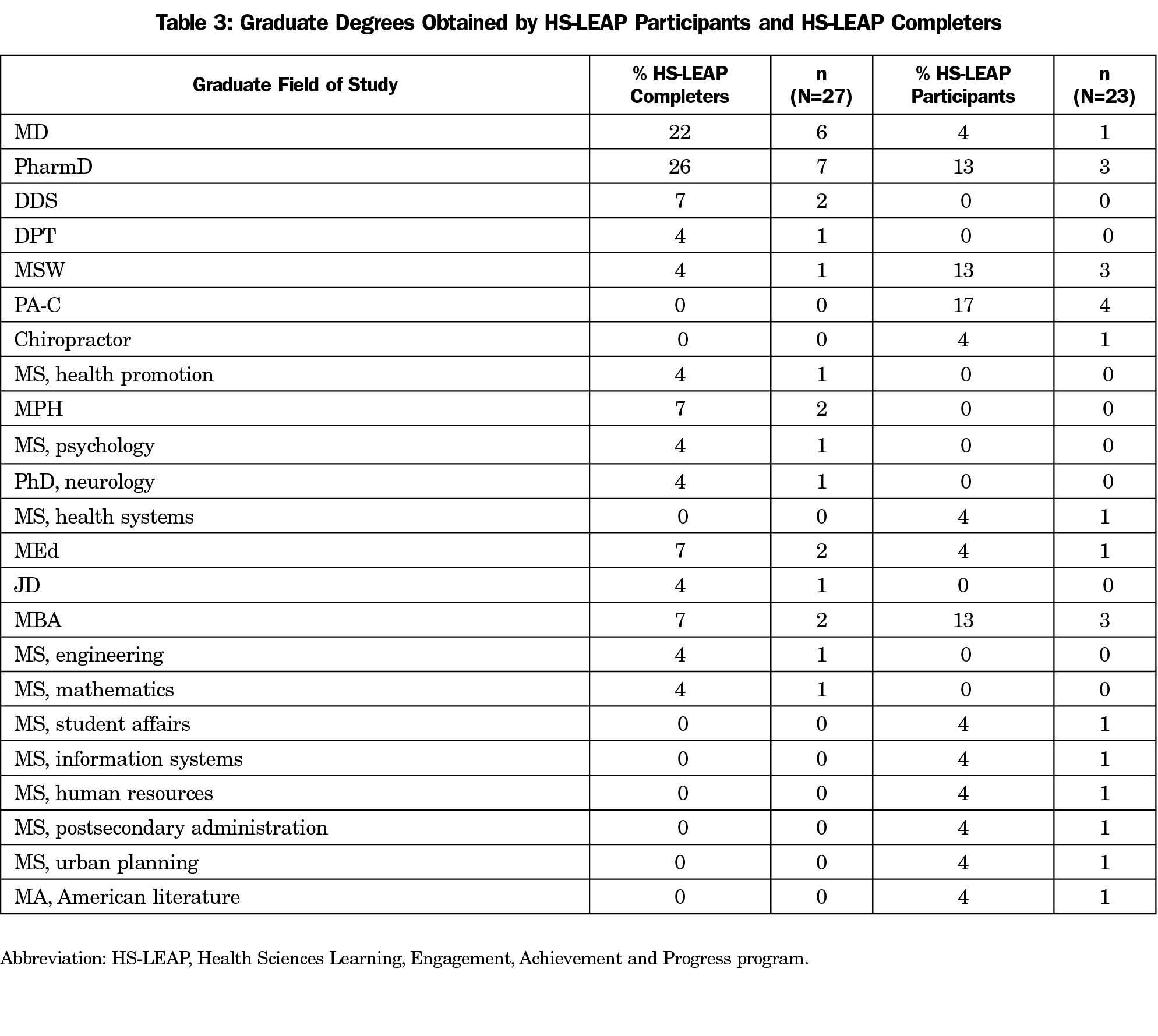
HS-LEAP participants enroll in graduate school at the same rate as their non-HS-LEAP peers. However, those who complete HS-LEAP attend graduate school at twice the rate of those who are participants in HS-LEAP (18.4% vs 9.2%, P<.01). At the time of this writing, 66% of those who obtained graduate degrees became health professionals, as illustrated in Table 3.
Funding
HS LEAP is fully funded through a partnership between the LEAP program in Undergraduate Studies on main campus and University of Utah Health. Support includes faculty compensation, student research stipends, and administrative salary support. HS-LEAP expenses include yearly faculty support of $2,500 per credit hour, guest lecture honorariums at $500 each, student research stipends cumulatively accounted for up to $40,000 per year, salary and benefit support of a half-time program manager at $42,000/yearly, and other miscellaneous incidentals. Per student participant, HS-LEAP operates at a rate of $3,445 over the 4 years (or $430/semester).
Participation in HS-LEAP is associated with higher mean first semester GPA, higher first-year fall-to-fall retention, and higher 6-year graduation rates when compared to those students who did not participate in any HS-LEAP activities. Completion of the HS-LEAP curriculum is associated with higher participation in graduate programs overall and in health sciences when compared to HS-LEAP participants who did not finish the program. Essentially, participation in at least one semester of HS-LEAP is beneficial for GPA, retention, and graduation, but completion of HS-LEAP is beneficial for graduate school participation. In the language of dose-response, 4 years of HS-LEAP is associated with more benefits than any lesser amount of participation. HS-LEAP has been well received and has been a focus of the diversity efforts of University of Utah Health.
HS-LEAP has a significant attrition rate (62%), and this is a threat to the validity of our study. We attempted to correct for this factor by including all participants in HS-LEAP in these data, not just graduates from HS-LEAP. HS-LEAP requires students to register when they are seniors in high school, at a time when most students are not sure what they are going to study in college. Conversations with graduates and former leaders reveal that most of those students who left did so because they are no longer interested in medicine or health care. The high attrition rate is being addressed, both in the curriculum, as well as in the selection of students. Future work will illustrate what effect the changes listed later in the discussion can have on HS-LEAP students.
Because of the observational nature of our study, we are not able to assert that HS-LEAP was a cause of the successes of our students. We celebrate the fact that our students’ success is completely theirs. They have overcome extreme obstacles to go as far as they have, and we want to both honor their journey and recognize their triumphs. Most importantly, our students develop and demonstrate grit, which is a major predictor of success in the health professions, and in medicine in particular.24 In the future, different methods of collecting data as well as different experimental designs are being considered to test HS-LEAP’s causation of our student success.
HS-LEAP students enter with a cohort in their first semester, which they remain a part of for all years that they participate in HS-LEAP. Students find a unique identity that connects them to a network of friendships and supportive colleagues as they continue their education. Students also connect to program faculty and advisors who can mentor them throughout college and prepare them to go beyond. Inclusion and belonging are associated with academic success, and HS-LEAP participation enhances this aspect of the cultural capital students need to succeed.25
Unlike other pipeline programs, HS-LEAP is a 4-year program designed to produce health professionals, not only physicians. Nearly all first-year HS-LEAP students state that they are going to medical school, but as students mature and are exposed to other health professions, their perspective may change. Since admission is competitive, students selected for HS-LEAP have demonstrated that they can do the work required for demanding graduate programs, evidenced by their strong coursework and GPAs. Engagement in the program helps the individual student focus on a health care professional goal, even when medical school is no longer an area interest. This part of the program is being strengthened, encouraging students of color to remain in health care, even though they may have become disenchanted with their original goals.
Like most pipeline programs, HS-LEAP could benefit from a greater connection with the graduate programs. We are exploring ways to more effectively connect these students with the health sciences graduate programs. Currently, we are negotiating for guaranteed interviews for HS-LEAP graduates in our professional degree programs. We are also engaging key Health Sciences faculty and staff in the HS-LEAP curriculum so that when the students do apply, they are not completely unknown to the programs to which they are seeking admission.
Successful programs that maintain the interest of URM students in the health sciences can effectively move toward equity in health profession education and improve health care delivery and outcomes. Because HS-LEAP pays the students for their university lab experience, as well as many of the faculty members who lecture in the program, there are significant costs for the University of Utah. We are now in contact with foundations, donors, and community leaders to identify areas where we can collaborate and increase the external funding of this project.
The most heartening changes to HS-LEAP are happening outside of our program. Many of the graduate programs (MD, DDS, DNP) are developing and refining their holistic admissions process, essentially giving credit for the distance traveled26 by each student. Our physican assistant program (Master’s in Physician Assistant Studies) and Biological Sciences PhD programs no longer require or consider the Graduate Record Examination (GRE) in their admissions processes. The medical school is actively developing a conditional acceptance program for students from their institutional diversity categories, namely the students underrepresented in medicine, as defined in the first paragraph of this paper. This will assuredly help further diversify our student bodies in each professional school, and it will enhance the quality of our programs.
References
- Rodriguez JE, Campbell KM, Adelson WJ. Poor representation of Blacks, Latinos, and Native Americans in medicine. Fam Med. 2015;47(4):259-263.
- Richert A, Campbell K, Rodríguez J, Borowsky IW, Parikh R, Colwell A. ACU workforce column: expanding and supporting the health care workforce. J Health Care Poor Underserved. 2013;24(4):1423-1431. doi:10.1353/hpu.2013.0162
- Marrast LM, Zallman L, Woolhandler S, Bor DH, McCormick D. Minority physicians’ role in the care of underserved patients: diversifying the physician workforce may be key in addressing health disparities. JAMA Intern Med. 2013.
- Winkleby MA. The Stanford Medical Youth Science Program: 18 years of a biomedical program for low-income high school students. Acad Med. 2007;82(2):139-145. doi:10.1097/ACM.0b013e31802d8de6
- United States Census Bureau. Utah Dashboard. https://www.census.gov/quickfacts/UT. Published 2018. Accessed June 24, 2019.
- Whitehurst L. Census Finds About 120 Languages Spoken in Utah. KSL.com. https://www.ksl.com/article/37282340/census-finds-about-120-languages-spoken-in-utah.Published November 8, 2015. Accessed June 6, 2019.
- Lubin G. Welcome to the Language Capital of the World: Queens, New York. World Economic Forum/ Business Insider. https://www.weforum.org/agenda/2017/02/queens-in-new-york-has-more-languages-than-anywhere-in-the-world. Published 2017. Accessed August 1, 2019.
- UMEC. Utah Medical Education Council. Utah’s Physician Workforce, 2016: A Study of the Supply and Distribution of Physicians in Utah. Salt Lake City, UT.2016.
- Utah Medical Education Council. Utah’s Physical Therapist Workforce, 2016 Salt Lake City, UT: Utah Medical Education Council; 2016. https://umec.utah.gov/wp-content/uploads/Utahs-Physical-Therapist-Workforce-2016-FINAL.pdf. Accessed July 6, 2020.
- Utah Medical Education Council. Utah’s Dentist Workforce, 2017: A Study of the Supply and Distribution of Dentists in Utah. Salt Lake City, UT: Utah Medical Education Council; 2017. https://umec.utah.gov/wp-content/uploads/Utah-Dentist-Workforce-Report-2017-1.pdf. Accessed July 6, 2020.
- Utah Medical Education Council. Utah’s Pharmacist Workforce, 2018. Salt Lake City, UT.: Utah Medical Education Council; 2018. https://umec.utah.gov/wp-content/uploads/Pharmacist-Workforce-Report-2018-FINAL.pdf. Accessed July 6, 2020.
- Campbell KM, Brownstein NC, Livingston H, Rodríguez JE. Improving underrepresented minority in medicine representation in medical school. South Med J. 2018;111(4):203-208. doi:10.14423/SMJ.0000000000000792
- Summers MF, Hrabowski FA III. Diversity. Preparing minority scientists and engineers. Science. 2006;311(5769):1870-1871. doi:10.1126/science.1125257
- Underwood SM, Fay T. The UWM Health Careers Bridge Program: an innovative approach for improving the recruitment, retention and graduation of minority students in nursing and health careers. J Nurs Educ. 1996;35(4):179-181.
- Keith L, Hollar D. A social and academic enrichment program promotes medical school matriculation and graduation for disadvantaged students. Educ Health (Abingdon). 2012;25(1):55-63. doi:10.4103/1357-6283.99208
- Sullivan WM, DeVolder J, Bhutiani M, Neal KW, Miller BM. The MD-MEd Joint-Degree Program at Vanderbilt University: Training Future Expert Medical Educators. Acad Med. 2017;92(8):1124-1127. doi:10.1097/ACM.0000000000001497
- Alfred L, Beerman PR, Tahir Z, LaHousse SF, Russell P, Sadler GR. Increasing underrepresented scientists in cancer research: the UCSD CURE program. Journal of cancer education : the official journal of the American Association for Cancer Education. 2011;26(2):223-227.
- Pizur-Barnekow K, Rhyner PM, Lund S. The pipeline training program in maternal and child health: interdisciplinary preparation of undergraduate students from underrepresented groups. Matern Child Health J. 2010;14(3):422-429. doi:10.1007/s10995-009-0478-x
- Guerrero AD, Holmes FJ, Inkelas M, Perez VH, Verdugo B, Kuo AA. Evaluation of the pathways for students into health professions: the training of under-represented minority students to pursue maternal and child health professions. Matern Child Health J. 2015;19(2):265-270. doi:10.1007/s10995-014-1620-y
- Bernstein J, Paine LL, Smith J, Galblum A. The MCH Certificate Program: a new path to graduate education in public health. Matern Child Health J. 2001;5(1):53-60. doi:10.1023/A:1011349902582
- Bliss C, Webb J, St.Andre M. The Impact of the University of Utah’s LEAP Program on Student Performance. J Gen Educ. 2012;61(1):19. doi:10.1353/jge.2012.0009
- Haggins A, Sandhu G, Ross PT. Value of Near-Peer Mentorship from Protégé and Mentor Perspectives: A Strategy to Increase Physician Workforce Diversity. J Natl Med Assoc. 2018;110(4):399-406. doi:10.1016/j.jnma.2017.09.001
- Hiss WC, Franks VW. Defining Promise: Optional Standardized Testing Policies in American College and University Admissions. National Association for College Admission Counseling. http://www.nacacnet.org/research/research-data/nacac-research/Documents/DefiningPromise.pdf2014. Accessed July 6, 2020.
- Duckworth A. Grit: The Power of Passion and Perseverance. New York: Scribner; 2016.
- Strayhorn TL. College students' sense of belonging : a key to educational success for all students. Second ed. doi:10.4324/9780203118924
- Ray R, Brown J. Reassessing student potential for medical school success: distance traveled, grit, and hardiness. Mil Med. 2015;180(4)(suppl):138-141. doi:10.7205/MILMED-D-14-00578
- Perlich P. Refugees in Utah. Salt Lake City, UT: Kem C. Gardner Policy Institute; 2017.




There are no comments for this article.