Background and Objectives: The feasibility of funding an additional year of residency training is unknown, as are perspectives of residents regarding related financial considerations. We examined these issues in the Family Medicine Length of Training Pilot.
Methods: Between 2013 and 2019, we collected data on matched 3-year and 4-year programs using annual surveys, focus groups, and in-person and telephone interviews. We analyzed survey quantitative data using descriptive statistics, independent samples t test, Fisher’s Exact Test and χ2. Qualitative analyses involved identifying emergent themes, defining them and presenting exemplars.
Results: Postgraduate year (PGY)-4 residents in 4-year programs were more likely to moonlight to supplement their resident salaries compared to PGY-3 residents in three-year programs (41.6% vs 23.0%; P=.002), though their student debt load was similar. We found no differences in enrollment in loan repayment programs or pretax income. Programs’ descriptions of financing a fourth year as reported by the program director were limited and budget numbers could not be obtained. However, programs that required a fourth year typically reported extensive planning to determine how to fund the additional year. Programs with an optional fourth year were budget neutral because few residents chose to undertake an additional year of training. Resources needed for a required fourth year included resident salaries for the fourth year, one additional faculty, and one staff member to assist with more complex scheduling. Residents’ concerns about financial issues varied widely.
Conclusions: Adding a fourth year of training was financially feasible but details are local and programs could not be compared directly. For programs that had a required rather than optional fourth year much more financial planning was needed.
The optimal length of training in family medicine has been hotly debated in the United States. for more than a decade.1-8 Proponents of longer training suggest an additional year should be added to address a broad scope of practice within the context of clinical and educational work hour requirements,9-11 lack of adequate preparation in medical school,12-14 and skills needed to perform in complex health care systems.15,16 Some have advocated for a 2-year training model similar to Canada. The decision is further complicated by challenges in how residency training is financed in the United States. Most US family medicine residency programs rely heavily on federal graduate medical education (GME) funding to support their residents and faculty salaries as well as program operations.17 However, that funding has been largely fixed since the introduction of caps on resident positions in 1997; thus, sponsoring institutions may be reluctant to allow residencies to add additional positions to their program without this traditional source of salary support. Federal funding formulas for direct medical education expenses (DME) currently provide only 50% funding for family medicine residents in a fourth year of training. However, if the discipline changed to 4 years of training, the Centers for Medicare and Medicaid Service would automatically pay for all 4 years.
Another consideration includes the decisions medical students make regarding an acceptable length of residency training given their debt load. In 2016, the Association of American Medical Colleges Graduation and Tuition and Student Fees survey indicated the average debt load for graduating medical students was $190,000.18 Research has shown that stress related to personal finances affects physical health and well-being among physician trainees.19 In fact, a recent study of the impact of debt load found high debt was correlated with callousness, stress, suicidal thoughts, failing medical licensing exams, and leaving or being dismissed from medical school.20 It is therefore important to understand whether residents view the opportunity cost of a fourth year of training as worth a year of lost practice income.
A well-established challenge in determining of how residency training is financed is the reported lack of transparency and accountability that exists in this regard.21,22 One survey study that had a 72% response rate from residency program directors reported that 59.3% of directors had attempted to discover this information and fewer than half were successful.21 Another challenge with attempting to ascertain this information in detail is that there is no way to validate that it is correct.
The Length of Training Pilot (LoTP) Study in family medicine was designed to address eight core research questions, one of which includes: “Is adding a fourth year of training financially feasible for residency programs?” As reported in other studies, we were unable to obtain specific budget data from all LoTP programs that would have allowed us to conduct a comparative quantitative financial analysis to address this research question. Thus, this paper reports on financial considerations of an additional year of training from the perspectives of residents and residency directors.
Length of Training Pilot
The LOTP, which runs from 2013 to 2022, is a mixed-methods prospective case-control pilot study designed to assess how the length of family medicine residency training affects both learner and program outcomes, such as scope of practice, preparedness for independent practice and clinical knowledge.23 Residency programs that had already transitioned to 4 years of training or that were planning to do so applied for the pilot in 2012 and, after approval, were matched to 3-year programs (3YR) based on region, size, and clinical training setting.
The LoTP includes a total of 17 residency programs that meet specific eligibility requirements, including being in good standing with the Accreditation Council for Graduate Medical Education (ACGME), and participating in all required evaluation activities. Seven 3YR civilian programs, six 4YR civilian programs, and four Navy programs applied for and were enrolled in the study. The Navy programs were excluded from these analyses because the costs associated with their programs are vastly different from civilian programs. Because of the large size of one 4YR program, two 3YR programs were matched to it to ensure equivalent numbers of residents in 3YR and 4YR groups. The 4YR programs included two university-based programs and four community-based, medical school-affiliated programs. They ranged in size from six to 22 residents per year. Four of the six 4YR programs required 4 years of training for all graduates, while two offered an optional fourth year of training where residents knew at the time of entry to the program that completing a fourth year was possible. Three-year programs included two that were university-based, four that were community-based, medical school-affiliated, and one community-based, nonaffiliated, and ranged in size from six to 11 residents per year.
Evaluation of the pilot is overseen by a team of educational researchers in the Department of Family Medicine at Oregon Health & Science University (OHSU). All LoTP programs obtained Institutional Review Board (IRB) approval. OHSU’s Institutional Review board granted the evaluation team an educational exemption to obtain data from the study sites (IRB# 9770).
Instrument Design and Data Collection
Residents and Graduates Data Collection. Quantitative resident financial data, collected from a resident survey administered annually between 2013-2018, included student loan debt, enrollment in loan repayment programs, moonlighting status and reasons to moonlight. We also asked 4YR programs to provide resident salaries according to program year and 66.7% did so. Graduate financial data, collected from a graduate survey administered annually 1 year after training was completed, included pretax income.
We derived resident perspectives on financial considerations from in-person focus groups during site visits and group telephone interviews. The financial question asked of 4YR program residents was: “How have you thought about financial considerations of a fourth year of training?” and of 3YR program residents: “How did financial considerations impact your decision to pursue a 3YR versus 4YR residency?” The questions posed to residents of 4YR and 3YR programs were slightly different to reflect the fact that residents in 4YR programs had already made their decision to pursue an additional year of training, so our interview prompts to elicit their perspective on financial considerations reflected this. In 4YR programs, a total of 47 residents participated in focus groups during site visits (2013-2014) and 22 residents participated in group telephone interviews in 2019. In 3YR programs, a total of 25 residents participated in group telephone interviews during virtual site visits (2014) and 28 residents participated in group telephone interviews in 2019.
Program Data Collection. We collected data on financial considerations of a fourth year of training from the program perspective during in-person meetings with 4YR program directors during site visits (n=6) and during annual telephone follow-up calls, during which three independent recorders collected field notes. Questions asked of the 4YR program directors included (1) “What was your approach to financing the fourth year of training?”; (2) “What approaches did you take to negotiate for additional resources?”; (3) “What resources did you need?”; and (4) “What financial advice would you give to other residency directors who are considering offering 4 years of training?”
Data Analyses
We used responses from PGY-3 residents in 3YR programs or PGY-4 residents in 4YR programs for demographics, student loan debt and loan repayment program enrollment. The graduate survey data were taken 1 year postgraduation for residents of both 3YR and 4YR programs. We excluded residents who trained in 4YR programs but who graduated after just 3 years of training because the study was designed to evaluate length of training. All of these were from optional 4YR programs. We analyzed quantitative data using descriptive statistics (χ2 or Fisher’s Exact test). All tests were two-sided with α levels set at 0.05.
Three independent observers collected field notes (notes recorded by trained observers to capture responses to questions asked by the facilitator) during in-person or telephone group interviews or focus groups. These were compiled into single composite documents to ensure the study record was complete for each event. Two study team members (P.A.C. and A.E.) conducted qualitative analyses of the composite documents. They used open coding of relevant passages and phrases in composite reports and then compared codes during consensus meetings held between July 2019 and August 2019. We applied the consensus open codes to the composite reports, a process that was repeated until coding was complete which included combining, eliminating and refining codes using constant comparative analyses.24 We achieved code saturation when no new codes were applied to the data, and saturated open codes were applied to the remaining composite reports. The analysis team then conducted axial coding25 and determined definitions for the selective codes24 in the form of themes and subthemes for each code category. We then selected exemplar statements from composite reports to illustrate these themes.
Participating Residents
No statistical differences were found for age, gender, race/ethnicity, marital or parental status, student loan debt load, or enrollment in loan repayment or scholarship programs between the two study groups (Table 1), though females predominated in both study groups.
Financial Considerations Among Residents
We found that PGY-4 residents in 4YR programs were more likely to moonlight compared to PGY-3 residents in 3YR programs (4YR=41.6% vs 3YR=23%; P=.002), even though their student debt load was not different. The main reasons they reported for moonlighting included to gain experience (3YR=89.2%, 4YR=88.9%) and to obtain extra income (3YR=83.8%, 4YR=66.7%), with about half reporting they moonlight to pay off debt (3YR=51.4%, 4YR=55.6%). None of these reasons were statistically significant between the two groups. Graduates also did not differ according to total pretax income or the percent who had certificates of added qualification (Table 1). Among residents in the 4YR programs, fourth-year salaries in 2013-2014 averaged $61,469 (SD=$1,935; range $51,078-$62,737) and increased to $67,324 in 2019-2020 (SD=$8,827; range $61,100-$73,584, data not shown).
Eight themes emerged based on the question, “How did financial aspects of 4 years of training affect your decision to choose a 4YR residency?” These included lost income (due to delaying entry into independent clinical practice), higher income (fourth year of training as a bargaining chip to get a higher salary), nonmonetary paybacks of additional training (benefits of gaining additional skills, including procedures, and confidence), delay in loan repayment (viewed by some as positive because of deferral, and viewed by others as negative because the start of repayment is delayed), philosophical issues related to income (if income mattered, they would not have chosen family medicine), higher salary in fourth year of training (salary structure significantly higher in fourth year), family considerations (needs of family are affected by additional training, that was perceived as more important than financial considerations), and avoidance (trying not to think about lost income, Table 2).
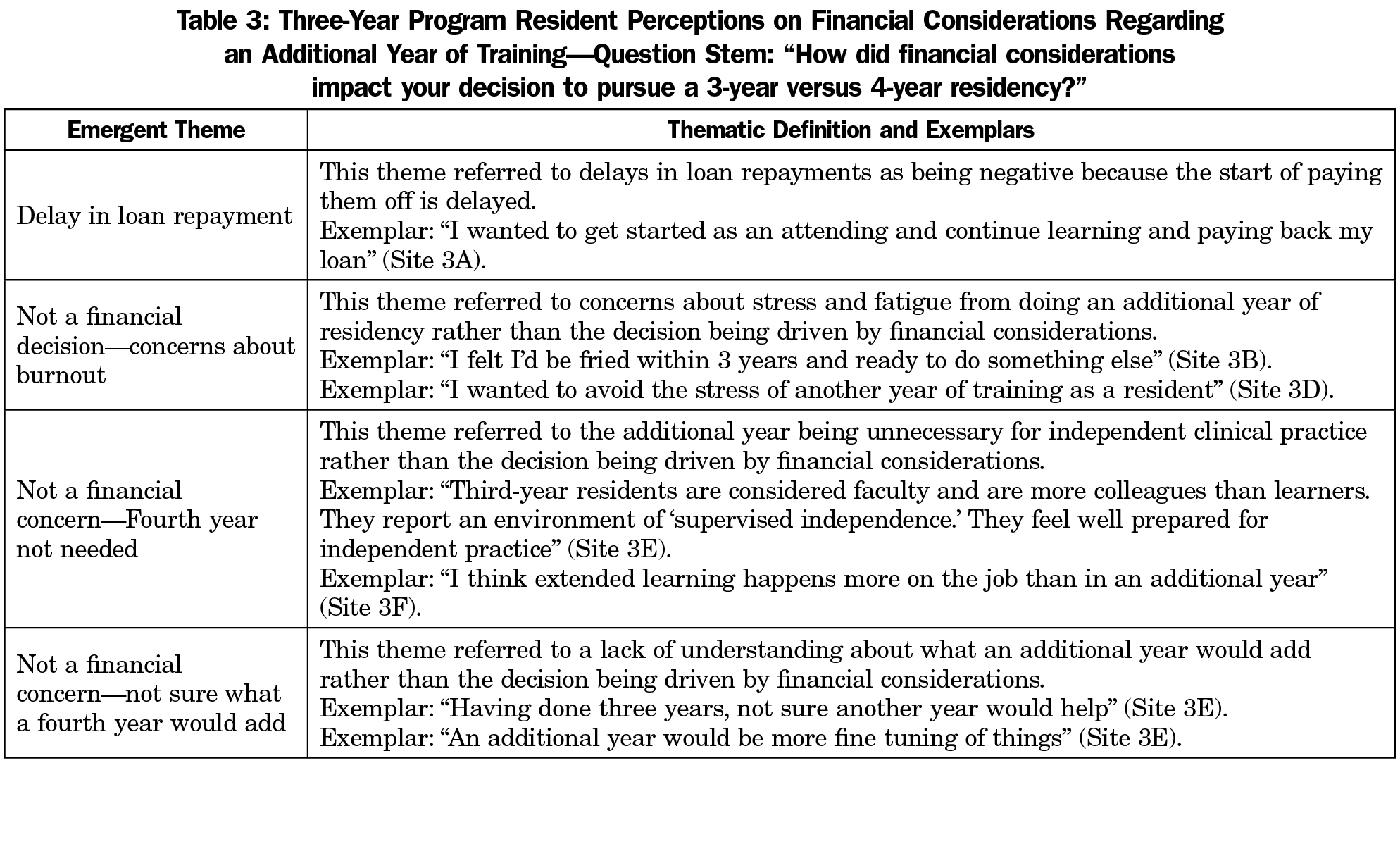
Four themes emerged from residents in 3YR programs who responded to the question, “How did financial considerations impact your decision to pursue a 3-year versus 4-year residency?” These included delay in loan repayment (viewed as negative because the start of repayment is delayed); concerns about burnout (financial considerations trumped by concerns about fatigue and stress related to an additional year of training); fourth year is not needed (financial considerations less important than the perspective that a fourth year is just not necessary for independent clinical practice); not sure what a fourth year would add (financial considerations trumped by uncertainty about what a fourth year of training would add, Table 3).
Financial Considerations of 4YR Programs
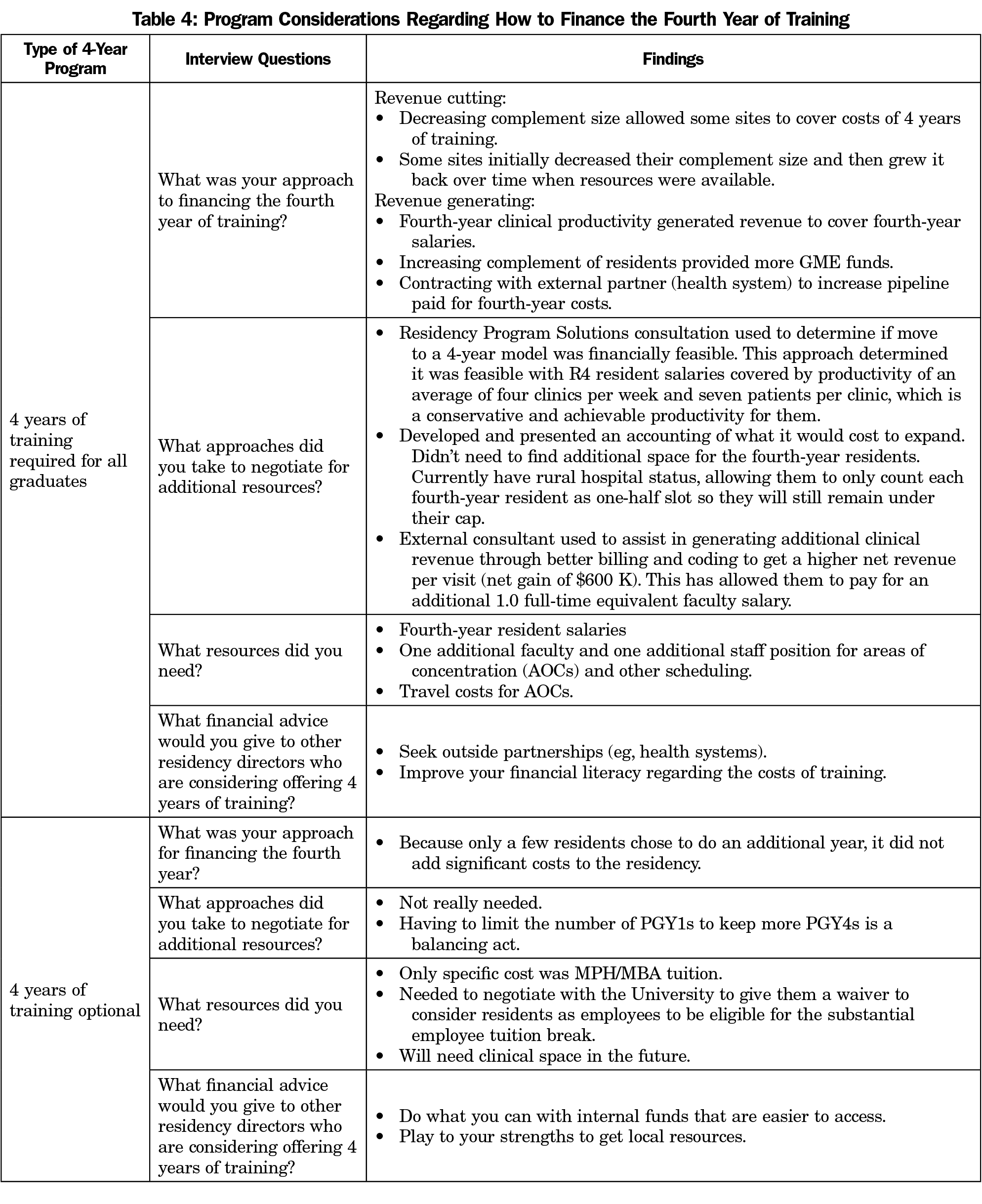
Programs’ descriptions of financing a fourth year of training varied according to whether the extra year was required of all residents or was optional (Table 4). Programs that required a fourth year typically undertook extensive planning to determine how to fund the additional year of training. Some reduced their complement of residents to cover fourth-year residents’ salaries. Some residencies initially reduced their complement and then increased it over time as the clinical productivity of fourth-year residents increased. One program contracted with another health system to establish a new continuity clinic site for residents to support the costs of the additional year of training. For programs with an optional fourth year of training, this change was essentially budget neutral because only a few residents chose to undertake the additional year of training.
The resources needed for programs with a required fourth year typically included resident salaries for the fourth year of training, one additional faculty full-time equivalent (FTE), and one additional staff member to assist with more complex scheduling. Resources needed by programs with an optional fourth year did not include adding faculty or staff because so few residents chose a fourth year. One program had costs associated with tuition for a master’s degree in public health or a master’s degree in business administration, but they negotiated with their sponsoring institution to allow residents to benefit from a substantial tuition reduction (Table 4).
Programs with a required fourth year typically used consultants (eg, Residency Program Solutions) to help determine whether a fourth year was financially feasible. One site received consultation on how to improve billing and coding to optimize net revenue per patient visit. These programs developed an accounting of what it would take to expand and then negotiated with their sponsoring institutions to execute the transition. The advice that residencies with a required fourth year would offer other program directors who are considering adding a fourth year of training included seeking outside partnerships, such as other health systems, and improving financial literacy regarding the costs of training. Advice from those who had an optional fourth year of training included maximizing internal funds that are easier to access and using program strengths to get local resources (Table 4).
This study examined financial considerations associated with extending residency training in family medicine by an additional year. It includes the perspectives of residents who trained in required and optional 4YR programs as well as those in 3YR programs. It also includes the viewpoints of program directors in both optional and required 4YR programs. We learned that offering an optional fourth year of training had much less financial impact on the programs than offering a required fourth year. A required fourth year necessitated one additional faculty and one staff member that was not needed if a fourth year of training was optional because the programs could absorb the costs of having between a few to about 33% of their residents undertaking an additional year of training. This finding is important because the RC-FM requires one core faculty member for every six residents.26 Thus, depending on the size of the program, 4YR programs may either need to hire more than one core faculty member or grant core faculty designation to another existing faculty member to be compliant.
Our findings also revealed that program directors explored various options, including potential additional institutional GME funding, and potential new financial income based on clinical productivity and more accurate billing strategies. Often, clinical productivity in the fourth year of training was an important source of income to support resident salaries in that training year, an important finding. However, our study did not discern whether the increase in residency visits represents a shift from faculty visits, which may affect the bottom-line revenues. Neither did we fully explore the extent to which highly capitated environments may have affected these costs. The most recent National Data Report from the Residency Review Committee for Family Medicine shows that the mean number of patient visits for fourth-year residents during 2017-2018 was 839 (SD=235.9, range 299-1,279; n=48 residents), and the average for PGY-3 residents was 924 (n=4,057).27 The importance of clinical productivity as a revenue source rests in the planning phase for the additional fourth year. Programs considering a move to an additional year of training should assess their practice population to ensure they can support the additional patient care volume provided by the fourth-year residents in their respective family medicine centers.
For many clinics, adding volume or increasing access should add significantly to the bottom line, unless seeing patients results in revenue loss because of payment models. In at least one case, this work had the unanticipated benefit of improving billing and coding practices to further stabilize their economic picture, while also providing a higher salary for fourth-year residents. We learned that fourth-year residents’ salaries varied greatly, especially toward the end of the measurement period and in all cases were higher than the average family medicine resident salary of $57,400 reported for 2019.28 Although productivity may be higher, some level of supervision is still likely to be needed in the fourth year. Notably, many programs lacked a sophisticated understanding of how their residencies are funded, due in part to the lack of transparency with sponsoring institutions that is well recognized in existing literature.29 Determining residency funding was essential in determining the feasibility of adding another year of training, which resulted in building a skill set that could benefit many residencies in the discipline.
We also learned that 4YR residents were statistically more likely to moonlight in their fourth year of training compared to their 3YR counterparts, though the reasons for moonlighting did not differ and were most commonly reported to gain experience. One possibility is that the intensity of training in the third and fourth year may be less, allowing for more time to moonlight. The debt load between the two groups also did not differ, suggesting this was not a reason for choosing 3 versus 4 years of training. Managing debt load is an important concern for most residents. We found that over one-third of residents in the LoTP were enrolled in loan repayment or scholarship programs with no differences between 3YR or 4YR programs. The most recent national survey of 2015 graduates of family medicine programs, as assessed 3 years after graduation, shows that 46% are enrolled in scholarship or loan repayment programs, an increase from 34% for 2013 graduates.30 Our results are based on resident responses at the start of residency and the higher rates noted nationally are likely due to graduates enrolling in federal, state, or local loan repayment programs after leaving residency.
Though fourth-year residents perceived that the additional year of training would yield higher salaries after graduation, we did not find this to be the case in our assessment of their pretax annual income derived from the graduate survey. Because we collected data on salaries after just 1 year of independent clinical practice, this may not be an accurate picture given that clinical productivity and other aspects of their training will likely result in higher salaries in the next few years, however both 3YR and 4YR programs are equally affected by this limitation. Regional differences could also be an influence on salaries; however, we matched each 4YR program with a comparable 3YR program in their region, which should take this into account, as we know the majority of family medicine residency training graduates practice within 100 miles of their training program.31
Other residents—some in 4YR programs and some in 3YR programs—commented on lost income due to delaying entry into independent practice as a financial consideration, with one resident estimating the loss to be about $200,000. Other residents preferred not to think about the lost income, suggesting that it is indeed a stressor. Several residents in 4YR programs commented on benefits of additional training that were not finance related, such as gaining additional skills and confidence. Philosophical issues about finances were also a common theme for residents in 4YR programs, who indicated that if money mattered to them, they would have chosen a higher paying discipline. Several of these residents thought that using a financial justification for not moving to 4 years of training was the wrong argument to make, indicating the benefits of additional training outweighed the price tag associated with it. The Medscape Physician Compensation Report for 201932 indicates that family physicians’ average annual income was $231,000 this year, with only pediatrics ($225,000) and public health and preventive medicine ($209,000) being lower. Family considerations were also mentioned as more important than finances in decisions about undertaking an additional year of training.
We found it interesting that many of the residents in 3YR programs identified nonfinancial concerns regarding a fourth year of training, such as concerns about burnout and that a fourth year of training was perceived as unnecessary or that it was unclear what added benefit would occur from the extra training. This is not to say that loan repayment delay was not a concern. It was certainly an emergent theme, as it was for residents in 4YR programs. As mentioned earlier, high debt load is correlated with significant health and professional consequences.19
Length of residency training ranges widely across disciplines from 3 to 8 years, and tends to be longer for the surgical specialties.33,34 Residents who undertake internal medicine or pediatrics residencies complete initial training in 3 years, but approximately 75%-80% of internists and 33% of pediatricians go on to subspecialty training.35,36 Emergency medicine (EM) is one of the few specialties with two ACGME-approved training formats with the 36‐month format (PGY 1-3) being used by 77% of residency programs and the 48‐month format (PGY 1-4) is used by 23%.37 A concern about lengthening training in family medicine is the effect it has on the physician workforce, as additional training would decrease the total number of residency graduates each year nationally if programs choose to keep their program size the same but spread their positions over 4 years instead of 3. This is a topic that will surely receive more attention as the discipline moves toward deciding about its future, though allowing both 3YR and 4YR programs may be desirable as occurs in emergency medicine.
The strengths of this study include the detailed information collected from programs and residents in both 3YR and 4YR programs on financial considerations related to length of training. Participating programs were located in many regions of the United States and matching characteristics were strong. Limitations included the challenge of calculating actual costs of adding a year of training because program directors really do not know how their programs are funded via federal direct and indirect costs, though we did determine what was needed categorically (eg, staff and faculty FTE). This limited our ability to assess detailed costs regarding space and other factors when adding a fourth year of training. This is unsurprising because many published studies have revealed the lack of transparency and accountability in this regard,21, 22 with one survey study with a 72% response rate of residency program directors reporting that 59.3% of directors have attempted to discover this information and fewer than half were successful.22
Generalizability of our findings is limited given the small number of programs (13) enrolled in the LoTP and the relatively small sample of 4YR program graduates, as the 4-year model was not fully implemented in all programs during the entire study period. This is a pilot study by design and such limitations are inherent in studies not statistically powered to achieve certain findings. The representation of female residents in both 3- and 4-year programs was higher than male and higher than the national average of 54.2%.38 It is difficult to determine what effect this difference in female representation may have on our findings. We did observe that information on debt load was missing for 14.1% of 4YR participants and 9.2% was missing for 3YR participants, though we were able to capture 85.9% and 90.8% for this variable, respectively.
In conclusion, we found that adding a fourth year of training was financially feasible and that the financial impact was greatest for programs that had a required rather than optional fourth year. Strategies used to support the residents’ salaries and other costs varied, and consultations with external advisors did help with financial planning. While not a driving factor in their residency selection, concerns about debt load exist among residents, regardless of length of training.
Acknowledgments
Financial Support: The Length of Training Pilot is sponsored by the Accreditation Council for Graduate Medical Education and is funded by the American Board of Family Medicine Foundation. None of the authors have a conflict of interest to declare regarding this article.
References
- Fields KB. More on the 4-year FM residency program. Fam Med. 2005;37(1):8.
- Scherger JE. Residencies: heal thyself before extending. Fam Med. 2006;38(3):158-159.
- Sairenji T, Dai M, Eden AR, Peterson LE, Mainous AG III. Fellowship or further training for family medicine residents. Fam Med. 2017;49(8):618-621.
- Carek PJ. The length of training pilot: does anyone really know what time it takes? Fam Med. 2013;45(3):171-172.
- Orientale E Jr. Length of training debate in family medicine: idealism versus realism? J Grad Med Educ. 2013;5(2):192-194. doi:10.4300/JGME-D-12-00250.1
- Saultz JW, David AK. Is it time for a 4-year family medicine residency? Fam Med. 2004;36(5):363-366.
- Schwenk TL. Residency should be expanded to 4 years. Fam Med. 2004;36(9):614-615.
- Duane M, Phillips RL Jr. Four-year residency training for the next generation of family physicians. Virtual Mentor. 2005;7(6):446-448.
- Kozakowski S, Abercrombie S, Carek P, et al. Perceived impact of proposed institute of medicine duty hours on family medicine residency programs. Ann Fam Med. 2009;7(3):276-277. doi:10.1370/afm.1007
- Antiel RM, Thompson SM, Reed DA, et al. ACGME duty-hour recommendations - a national survey of residency program directors. N Engl J Med. 2010;363(8):e12. doi:10.1056/NEJMp1008305
- Harris JD, Staheli G, LeClere L, Andersone D, McCormick F. What effects have resident work-hour changes had on education, quality of life, and safety? A systematic review. Clin Orthop Relat Res. 2015;473(5):1600-1608. doi:10.1007/s11999-014-3968-0
- Walling A, Merando A. The fourth year of medical education: a literature review. Acad Med. 2010;85(11):1698-1704. doi:10.1097/ACM.0b013e3181f52dc6
- Stevens CD. Commentary: Taking back Year 4: a call to action. Acad Med. 2010;85(11):1663-1664. doi:10.1097/ACM.0b013e3181f53487
- Sklar DP. Making the fourth year more meaningful. Acad Med. 2014;89(4):527-528. doi:10.1097/ACM.0000000000000184
- Bohmer RM. Managing the new primary care: the new skills that will be needed. Health Aff (Millwood). 2010;29(5):1010-1014. doi:10.1377/hlthaff.2010.0197
- Pugno PA. One giant leap for family medicine: preparing the 21st-century physician to practice patient-centered, high-performance family medicine. J Am Board Fam Med. 2010;23(suppl 1):S23-S27. doi:10.3122/jabfm.2010.S1.090291
- Congressional Research Service. Federal Support for Graduate Medical Education: An Overview. December 27th, 2018: https://fas.org/sgp/crs/misc/R44376.pdf. Accessed January 7, 2020.
- Wisenberg BD. Taking the sting out of medical school debt. AAMC News. April 4, 2017. https://news.aamc.org/medical-education/article/taking-sting-out-medical-school-debt/ Accessed September 16, 2019.
- Connelly P, List C. The effect of understanding issues of personal finance on the well-being of physicians in training. WMJ. 2018;117(4):164-166.
- Phillips J. The impact of debt on young family physicians: unanswered questions with critical implications. J Am Board Fam Med. 2016;29(2):177-179. doi:10.3122/jabfm.2016.02.160034
- Chaudhry SI, Khanijo S, Halvorsen AJ, McDonald FS, Patel K. Accountability and transparency in graduate medical education expenditures. Am J Med. 2012;125(5):517-522. doi:10.1016/j.amjmed.2012.01.007
- Committee on the Governance and Financing of Graduate Medical Education; Board on Health Care Services; Institute of Medicine. Graduate Medical Education That Meets the Nation's Health Needs. Eden J, Berwick D, Wilensky G, eds. Washington (DC): National Academies Press (US); 2014 Sep 30.
- Length of Training Pilot Project. http://www.lotpilot.org. Accessed August 12, 2019.
- Johnson B, Christensen LB. Educational research: quantitative, qualitative, and mixed approaches. 4th ed. Thousand Oaks, CA: SAGE Publications; 2012.
- Creswell JW. Qualitative inquiry and research design: choosing among five approaches. 2nd ed. Thousand Oaks, CA: Sage Publications; 2007.
- Accreditation Council for Graduate Medical Education. Specialty-specific references for DIOs: number of faculty members 6/2018. https://www.acgme.org/Portals/0/PDFs/Specialty-specific%20Requirement%20Topics/DIO-Number_of_Faculty.pdf. Accessed February 18 2020.
- Accreditation Council for Graduate Medical Education. Accreditation Data System (ADS). https://www.acgme.org/Data-Collection-Systems/Overview. Accessed March 18, 2020.
- Medscape Residents Salary and Debt Report 2019: https://www.medscape.com/slideshow/2019-residents-salary-debt-report-6011735#3. Accessed March 13, 2020.
- Regenstein M, Snyder JE, Jewers MM, Nocella K, Mullan F. Comprehensive revenue and expense data collection methodology for teaching health centers: a model for accountable graduate medical education financing. J Grad Med Educ. 2018;10(2):157-164. doi:10.4300/JGME-D-17-00542.1
- Association of Family Medicine Resideny Directors. 2018 National Family Medicine Residency Graduate Survey. https://www.afmrd.org/page/national-family-medicine-graduate-survey. Accessed Feb 12, 2020
- Fagan EB, Gibbons C, Finnegan SC, et al. Family medicine graduate proximity to their site of training: policy options for improving the distribution of primary care access. Fam Med. 2015;47(2):124-130.
- Medscape Physician Compensation Report 2019: https://www.medscape.com/slideshow/2019-compensation-overview-6011286#3. Accessed December 19, 2019.
- Accreditation Council for Graduate Medical Education. AMA Green Books. https://www.acgme.org/About-Us/Publications-and-Resources/AMA-Green-Books. Accessed February 18, 2020.
- American Medical Association. FREIDA. https://freida.ama-assn.org/. Accessed Febraury 18, 2020.
- Byrne BJ, Katakam SK, Frintner MP, Cull WL. Early career experiences of pediatricians pursuing or not pursuing fellowship training. Pediatrics. 2015;136(4):672-679. doi:10.1542/peds.2014-3973
- Henderson D. Most internal medicine residents plan subspecialty careers. Medscape, December 4th, 2012: https://www.medscape.com/viewarticle/775601 (Accessed 02/19/20).
- Smith-Coggins R, Baren JM, Beeson MS, et al; Research Committee, American Board of Emergency Medicine. American Board of Emergency Medicine report on residency training information (2013-2014), American Board of Emergency Medicine. Ann Emerg Med. 2014;63(5):637-645. doi:10.1016/j.annemergmed.2014.03.008
- American Academy of Family Physicians. Selected Demographic Characteristics of AAFP Members (as of December 31, 2018). https://www.aafp.org/about/the-aafp/family-medicine-specialty/facts/table-2.htmlAccessed February 12, 2020.





There are no comments for this article.