Background and Objectives: Adverse childhood experiences (ACEs) affect nearly two-thirds of the US population and have long-lasting consequences on health and well-being. Integrating ACEs education into medical curricula is vital to equip future physicians to address these effects. This systematic review evaluates the effectiveness of ACEs educational interventions in US medical education on student and resident knowledge, attitudes, or practice.
Methods: We conducted a comprehensive literature search in January 2025 using MEDLINE (PubMed), ERIC, and PsycInfo databases for studies published between 2013 and 2025, reported using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Inclusion criteria were empirical studies evaluating ACEs training in US medical schools and residency programs in the English language. Study selection, data extraction, and quality assessment were performed independently by two authors, with discrepancies resolved by coauthor consensus.
Results: A total of 608 unique studies were identified from our search and screened, with 15 studies meeting the inclusion criteria. Most interventions relied on lecture-based formats, though 46.7% included interactive components such as small-group discussions and standardized patient interactions. While most studies reported significant increases in ACEs knowledge postintervention, only 20% evaluated objective knowledge changes, with the majority relying on self-assessment. Confidence in addressing ACEs improved in 46.7% of studies, but only 6.7% objectively measured behavioral changes.
Conclusions: ACEs education in medical training is expanding, but current interventions vary and often lack methodological rigor. Most studies show short-term knowledge gains, though few assess lasting behavior change. Future research should prioritize objective and longitudinal outcomes to better prepare physicians to address ACEs in clinical practice.
Adverse childhood experiences (ACEs) encompass traumatic events occurring before age 18, including abuse, neglect, and household dysfunction (eg, substance use, mental illness, parental separation, incarceration, domestic violence).1,2 ACEs are common, with 61% of the US population reporting at least one and 15% reporting four or more;1,2 and their long-term effects on health, development, and overall well-being are well documented.2-4 Prolonged ACE-related stress can dysregulate the sympathetic nervous system, trigger chronic inflammation, and disrupt neurodevelopment.1,5 Those affected may struggle with attention, learning, decision-making, and emotional regulation, and may engage in health-risk behaviors.1,5 Moreover, a dose-dependent relationship exists between ACE exposure and the risk for negative health outcomes, including depression, chronic diseases, and substance misuse.2
Early identification of ACEs is crucial for timely interventions. Fostering social and emotional connections between children and trusted adults while providing families access to community resources is important.5,6 These measures help children build resilience and may prevent ACEs in future generations.5,6 Physicians also can adopt trauma-informed care practices to prevent retraumatization and establish trust,7-11 which increases patients’ likelihood of following health recommendations and supports better long-term health outcomes.7,8
Despite growing recognition of the significance of ACEs and their impact on health outcomes, a substantial gap remains in their identification and management in clinical practice. Many physicians are unaware of ACEs or rarely screen for them, with insufficient training identified as a significant barrier.12-17 Although timing is debated, evidence supports including ACEs training into curricula18-21 and faculty trainings.22 Literature shows continuous learning over longer periods leads to better retention of knowledge and skills.23 Therefore, we conducted a systematic review of ACEs educational interventions targeting earlier stages in a physician’s training (ie, medical school and residency). While two previous systematic reviews were related to this topic,24,25 this is the first US-focused review analyzing ACEs educational interventions among both medical students and residents within undergraduate medical education and residency training programs. We included residents across all specialties to reflect ACEs’ broad health impacts, building on prior work focused on primary care physicians.25 Furthermore, while Ramesh et al (2019)24 focused on medical school curricula, their study preceded the 2020 COVID-19 pandemic, which raised public health concerns about ACEs exposure.26-28 The pandemic was a time of rapid curricula change and influenced how educational materials were delivered and the topics covered.29 Hence, an updated review is important to capture studies implemented postpandemic.
The overall goal of this study was to conduct an updated systematic review that would use the Kirkpatrick model as a guiding framework to build upon previous work and enhance understanding of the medical education gaps in ACEs knowledge and awareness to inform future educational intervention efforts.30 Specifically, we aimed to:
Identify ACEs educational interventions implemented in medical schools and residency programs in the United States;
Assess the effectiveness of ACEs educational interventions in improving student and resident physician knowledge, attitudes, or practice of ACE identification and management; and
Discuss key recommendations for enhancing ACEs educational training and curricula in medical schools and residency programs.
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 202031 and PRISMA-S32 guidelines. It was conducted according to guidance found in the Cochrane Handbook for Systematic Reviews of Interventions.33 This study was deemed nonhuman subjects research by the Michigan State University Institutional Review Board.
Search and Study Selection
MEDLINE (including PubMed Central; PubMed), Education Resources Information Center ([ERIC] EBSCO), and PsycInfo and PsycArticles (ProQuest) databases were searched from January 1, 2013, to January 13, 2025. The search strategy was developed by a health sciences librarian (I.K.G.), and the research team reviewed it for completeness before it was deployed. The search strategies utilized free text keywords and database-specific controlled vocabulary terms using the broad conceptual categories of pediatric population AND ACE AND medical education AND curriculum. Full search strategies for each database are detailed in (Appendix 1). Forward and backward citation chaining of five highly relevant references34-38 was completed using Scopus (December 6, 2023). Deduplication, screening, and data extraction were performed using Covidence systematic review software.39
We included peer-reviewed, English language full-text articles from 2013 to 2025. The date range limitation was chosen because published literature regarding ACEs and medical education has grown exponentially over the past decade. Articles met the inclusion criteria if they were empirical studies examining ACEs educational interventions implemented in medical schools and residency programs in the United States. We included studies that evaluated the impact of ACEs educational interventions on outcomes including participant knowledge, confidence, attitudes, and skills regarding ACE identification and management. We defined “educational interventions” broadly as curricula or training aimed at improving ACEs knowledge, awareness, skills, or practice. We excluded studies that did not focus on ACEs training in the United States, studies evaluating ACEs training outside of medical schools and residency programs, and studies employing a systematic review design.
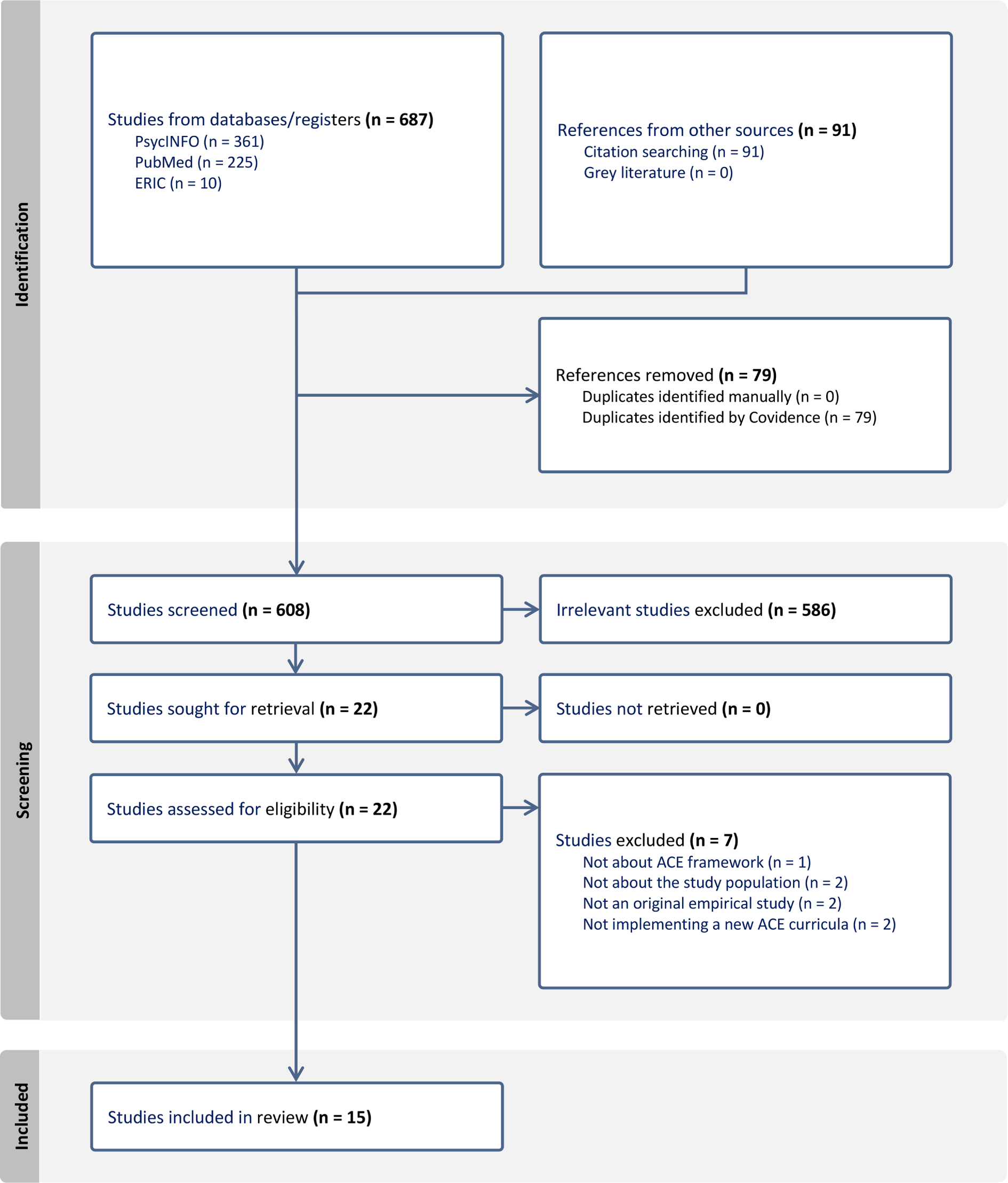
An initial pilot review of the title and abstracts of 16 articles from the search was conducted by two authors (H.F., Y.Z.H.) to iteratively refine and solidify the inclusion criteria and ensure that reviewers were applying the criteria consistently. The reviewers (H.F., Y.Z.H.) had 100% interrater agreeability during piloting. Following piloting of screening criteria, two reviewers (H.F., Y.Z.H.) independently screened all titles and abstracts using these criteria (n=608). Discrepancies in article selection were resolved through discussion with two additional reviewers (J.P., D.W.) to achieve consensus. Full-text review of the remaining articles (n = 22) was then completed by two independent reviewers (H.F., Y.Z.H.). Seven articles were excluded during full-text screening resulting in a final analytic sample of 15 articles. See Figure 1 for the PRISMA flowchart.
Data Extraction
A data extraction template was developed within Covidence, covering parameters such as study population, study design, objectives, program format, training duration, outcomes, and key findings. Due to the diverse array of language used to assess different outcomes across the included articles, we categorized the findings into four general categories based on recurring themes to synthesize and facilitate ease of interpretation. First, we considered knowledge and skills. Next, we examined comfort and confidence in addressing ACEs, then attitudes toward ACEs. Lastly, we considered planned or observed behavior changes after the interventions. In alignment with Medical Education Research Study Quality Instrument (MERSQI)40 domains, we categorized assessments of knowledge as either objectively measured or self-assessed. Two reviewers (H.F., Y.Z.H.) independently extracted data using Covidence to facilitate the creation of the literature review table. Two additional reviewers (J.P., D.W.) reviewed the table for accuracy and completeness.
Data Analysis
We cataloged study characteristics, including objectives, study populations, study design, intervention, outcomes measured, and key findings. To assess the types of outcomes examined in each study, we applied the Kirkpatrick model, focusing on domains such as changes in knowledge, skills, attitudes, confidence, and behavior, which correspond primarily to levels 2 and 3 of the framework.30 We also specified whether these changes were self-reported or objectively measured. After identification of study design, we assessed the quality of each article using the MERSQI tool,40 a 10-item validated instrument utilized to assess the quality of medical education research. Each article underwent independent assessment by two reviewers (H.F., Y.Z.H.), and findings were discussed to achieve consensus.
The database searches and citation chaining produced 687 articles. After deduplication, 608 unique studies were left to screen. Following a review of titles and abstracts, 586 studies were excluded, leaving 22 articles for full-text review. Of these, 15 met the inclusion criteria (Figure 1).
Study Population
Table 1 outlines the study populations and intervention characteristics of each study. Of the 15 ACEs curricula, seven (46.7%) were designed for residents36-45 and seven (46.7%) for medical students. Of the latter, two were for first-year medical students,37,46 three for second-year students,34,47,48 and one for third-year students.49 Additionally, one study implemented its ACEs curriculum across nine health profession programs, including an osteopathic medical school.50 One curriculum (6.7%) was implemented for second-year pediatric residents, primary care attending physicians, pediatric fellows, and medical students rotating in the pediatric hospital.35 All 15 curricula were single institution interventions.34-50
Author |
Objective(s)a |
Study population |
Study design |
Intervention |
Outcomes |
Kirkpatrick model level |
Key findingsb |
MERSQI score |
Chokshi, Chen, & Beers (2020)35 |
To assess the effectiveness of a TIC module on increasing knowledge, skills, attitudes, and confidence regarding trauma-informed approaches and resiliency building in clinical practice |
Primary care practitioners and trainees (N = 35), including second-year pediatric residents (n = 28), attending physicians (n = 4), medical students (n = 2), and fellows (n = 1) |
Pre-post |
Interactive case-based childhood adversity and TIC electronic module:
Four asynchronous online modules. Duration: 2 hours. Start/end dates: cannot be determined. |
Score changes in self-reported knowledge, attitudes, confidence, and practice. |
2 |
Statistically significant score increases in self-reported knowledge, attitudes,c confidence, and intention to practice TIC (P<0.001) for all topics, respectively. |
8.5 |
Chokshi et al (2020)47 |
To determine how a TIC symposium affects student knowledge and understanding of a TIC approach to childhood adversity |
Second-year medical students (N = 179) |
Mixed methods (quantitative descriptive and qualitative content analysis) |
TIC symposium included three interactive mini-lectures and a small group case-based discussion. Duration: 4 hours. Start/end date: cannot be determined. |
Self-reported plans to apply information to clinical practice. Self-reported changes in understanding of ACEs and TIC, understanding of how to incorporate trauma- informed practices in clinical care, and use of concepts in clinical rotations. |
2 |
73% of respondents indicated that they applied the learned information to patient care and procedural skills; 42% to medical knowledge; 67% to interpersonal and communication skills; 35% to professionalism. 92% of participants indicated that they “agreed” or “strongly agreed” that their knowledge increased regarding ACEs health outcomes; 93% “agreed” or “strongly agreed” that they had better understanding of TIC; 87% “agreed” or “strongly agreed” they had a better understanding of how to incorporate TIC during patient interactions; 90% “agreed” or “strongly agreed” that they plan to use concepts learned in clinical rotations (no statistical inference testing). |
9 |
Chokshi & Goldman (2021)43 |
To assess the effectiveness of a TIC training on improving knowledge, attitude, and confidence, and to assess how TIC is practiced in the clinical setting |
Internal medicine residents (N = 91) |
Mixed
methods, (pre-post and qualitative interviews for thematic analysis) |
A virtual lecture and a didactic component with audience response, multiple-choice questions, and breakout rooms. Duration: 4 hours. Start/end date: cannot be determined. |
Changes in self-reported knowledge, attitude, and confidence. Identification of themes relating to application of TIC in clinical practice. |
2 |
Statistically significant score increase in self-assessed knowledge and confidence in TIC (P<0.001 for both topics); no statistically significant score changes in attitudesd (average P = 0.066). Six themes were identified regarding factors that impact the application of TIC in clinical settings, including patient characteristics, timing of TIC, inpatient setting barriers, patient-doctor relationship, inadequate follow-up resources, and need for repetitive TIC practice. |
8 |
Goldstein et al (2018)34 |
To assess the impact of TIC training on increasing ACE-related knowledge, health impacts, and application in clinical practice |
Medical students (N = 20) |
Qualitative content analysis |
Lectures, discussions, and practice delivering TIC via role play. Duration: 6 hours. Start/end date: June 2014–June 2015 |
Self-reported strengths gained from training.
Note: outcomes were not well-defined |
2 |
Self-reported gains in knowledge, recognition, and understanding of trauma’s impact; self-reported increased confidence to discuss trauma with patients; self-reported increased ability to ask about trauma (no statistical inference testing). |
8 |
Lloyd et al (2021)42 |
To assess the effectiveness of standardized patient cases on increasing resident knowledge, confidence, and clinical skills related to trauma and resilience |
Second- through fourth-year categorical and combined pediatric residents (N = 22) |
Pre-post |
Orientation presentation via PowerPoint, reading material, three standardized patient encounters, group debriefing. Duration: 4 hours. Start/end date: March 2019–March 2020 |
Self-reported frequency with which ACEs are considered in patient care, comfort with screening for ACEs, discussing ACEs with patients, explaining how traumatic experiences impact health, identifying protective factors and promoting resilience, and de-escalation. |
2 |
Statistically significant increases in self-reported frequency of considering ACEs in patient care (P = 0.004), comfort discussing and explaining ACEs/trauma to families (P = 0.006), comfort asking patients about an ACE experience (P = 0.019), explaining how trauma impacts health (P = 0.001), identifying protective factors and counseling on resilience (P<0.001), and de-escalating patients (P<0.001). |
9 |
Marsh et al (2019)49 |
To assess the effectiveness of a lecture on improving student knowledge about advocacy and SDOH |
Third-year medical students (N = 75) |
Pre-post |
Small group lectures on advocacy and SDOH. Duration: 45–60 minutes. Start/end Date: October 2016–October 2017 |
Changes in knowledge of advocacy and SDOH. Changes in self-reported advocacy skills. |
2 |
Statistically significant increases in 4/10 test questions on knowledge of ACEs study, childhood hunger, patient advocacy methods, and children’s health insurance (P<0.05); nonsignificant increases in 5/10 knowledge test questions; nonsignificant decrease in knowledge of medical advocacy. Results not reported for self-assessed advocacy skills. |
11.5 |
Marsicek et al (2019)41 |
To assess the effectiveness of a standardized screening tool on increasing ACE screening rates and to assess resident and physician comfort level and familiarity with ACEs screening |
Pediatric residents and physicians (N = 24) |
Pre-post |
Standardized screening tool was implemented; residents attended two educational seminars and participated in a simulated patient experience. Duration: 1 hour. Start/end date: July 2017–July 2018 |
Changes in the percentage of ACE screens completed. Changes in self-reported comfort level and familiarity with ACEs screening. |
3 |
Increased percentage of ACE screens completed (from 0%–60%) screening rates. No statistically significant changes in self-reported physician comfort level (p = 0.219), familiarity with the Felitti et al2 ACEs study (P = 0.258), or likelihood to administer and assess an ACEs questionnaire (P = 0.091). |
8 |
Miller-Cribbs et al (2020)45 |
To evaluate the impact of a trauma-informed training program on level of trauma-informed communication skills acquired by participants and to determine whether changes made to curriculum based on participant feedback is associated with skill improvement |
Family medicine and internal medicine residents, and OT/PT students (N = 53) |
Quantitative descriptive (simulation study) |
The Professional ACEs-Informed Training for Health simulation training program included didactic presentation and discussion, video of a model encounter, simulation experience with standardized patients, group debriefing, and self-care. Duration: 3–4 hours repeated over 3 years with new content introduced each year. Start/end date: cannot be determined. |
Demonstrated use of trauma-informed skills to address ACEs among adults in standardized patient encounters. |
2 |
Most frequently demonstrated trauma-informed communication skills included explaining ACEs and their impacts (8.2%), empathy (8.2%), collaborative treatment planning (9.0%), and stigma reduction (4.7%). Less frequently demonstrated skills were asking permission to discuss ACEs (1.5%) and employing metaphors (1.1%) or infographics (1.6%) for explanation.
Between years 1 and 4, residents demonstrated a higher frequency of explaining ACE impacts on the brain/body (7.8% vs 9.1%), using metaphors (0.1% vs 2.4%) and infographics (0.8% vs 3.15%), attempts at stigma reduction (4.4% vs 5.5%), and using closed questions (6.9% vs 9.8%), but no statistical inference testing was conducted.
Between years 1 and 4, residents demonstrated a decrease in the frequency of empathy (14.9% vs 10.6%), collaborative treatment planning (9.2% vs 7.5%), using open questions (22.3% vs 20.5%), using cues (21.5% vs 20.5%), and missing cues (24.8% vs 16.9%); however, no statistical inference testing was conducted. |
9.5 |
Morrison et al (2021)36 |
To assess whether a simulation-based SDOH training increases resident confidence to discuss four types of SDOH (food insecurity, unsafe housing, access to care, and ACEs) |
First- and third-year pediatric residents (N = 72) |
Pre-post quasi-experimental |
Four simulated patient encounters (one actively participating and three observing) and debrief session. Duration: 90 minutes. Start/end date: cannot be determined. |
Changes in self-reported confidence to discuss four types of SDOH in simulation scenarios. Longitudinal evaluation of self-reported comfort and behavioral changes in practice. |
3 |
Statistically significant increase in self-reported confidence to discuss SDOH posttraining (P<0.01). Self-reported confidence to discuss SDOH was sustained 9–12 months later as reflected by nonsignificant P values. Statistically significant increase in the percentage of first-year residents who reported having clinical conversations about ACEs two or more times in the follow-up survey (P = 0.02). |
10 |
Onigu-Otite & Idicula (2020)37 |
To assess the effectiveness of a lecture in increasing student knowledge of 10 ACE-specific content areas |
First-year medical students (N = 32) |
Pre-post with an additional qualitative component |
In person lecture with PowerPoint presentation, infographics, short videos, an interactive chart from the CDC, and a case-based presentation. Duration: 1 hour. Start/end dates: April 2019. |
Changes in self-reported knowledge of 10 ACE-specific content areas spanning ACE identification, ACE scores, and ACE health impacts. Student self-reported feedback on the training. |
2 |
Statistically significant increase in the mean self-reported score across 10 content areas (P<0.001). Student feedback indicated the training information and format was useful and well-received. |
7.5 |
Osei et al (2022)48 |
To assess the effectiveness of a case-based trauma-informed curriculum in increasing ACE knowledge, skills, attitudes, and behavior changes |
Second-year medical students (N = 65) |
Pre-post |
An asynchronous online module with a clinical case study followed by synchronous virtual discussion of the case, including a large group lecture, small group discussion, and large group debrief. Duration: 90 minutes. Start/end date: cannot be determined. |
Changes in self-reported ACEs knowledge and skills (defining and describing ACEs, ACEs screening, identifying protective factors, and knowledge of resilience tools). Self-reported behavioral changes in clinical care at 3 month follow-up. |
2 |
Statistically significant increase in self-reported ACE knowledge and skills (P<0.001 for both topics). 26% of participants reported using all TIC concepts from the workshop in clinical practice 3 months later. |
9.5 |
Pletcher et al (2019)46 |
To assess the effectiveness of a mandatory workshop in improving ACE-related and TIC-related knowledge, skills, and attitudes. |
First-year medical students (N = 535) |
Quantitative descriptive |
PowerPoint presentation, TEDMED Talk, and small group discussions with a sample case. Duration: 2.5 hours. Start/end date: academic year 2016–2017 to 2018–2019 |
Average postsession quiz grades. Self-reported degree of improved knowledge and skills related to ACEs. Self-reported degree to which workshop components (reading, lecture, video, small group, facilitator) changed attitudes or perspectives regarding ACEs. |
2 |
Quiz grades were above 90% in academic years 2018–2019. Students self-reported that the workshop increased their ACE-related knowledge and/or skills “to a considerable degree” for describing the physical and mental health consequences of ACEs (52%); discussing use of ACE survey in medical home (52%), discussing impact of resilience on mitigating ACEs (52%), and describing how trauma-informed care benefits patients (46%); no statistical inference testing. Students self-reported that all workshop components except for reading contributed to a “considerable” change in their ACE-related attitudes and perspectives: lecture (47% of responses); video (48%); small group (48%), and effectiveness of facilitator (59%); no statistical inference testing. |
9.5 |
Schmitz et al (2019)38 |
To assess the effectiveness of an online module in increasing resident ACE-related knowledge, confidence, and longitudinal behavior changes |
Second- and third-year pediatric and medicine-pediatric residents (N = 91) |
Pre-post |
Asynchronous online module. Duration: 25 minutes. Start/end date: 2016–2017 (total of 19 months). |
Changes in self-reported knowledge and confidence to discuss ACEs. Percentage of residents who report behavioral changes in clinical care at longitudinal 3 month follow-up. |
3 |
Statistically significant increase in self-reported confidence in, knowledge and ability to discuss ACEs (P<0.05 for both topics). Statistically significant increase in the percentage of residents who self-reported discussing ACE-related topics with patients during visits (P<0.01). |
8.5 |
Scott et al (2024)44 |
To assess the effectiveness of a training curriculum in increasing exam room interaction skills |
First-year family medicine residents (N = 39) |
Pre-post |
Didactics, skills training, role play, and coaching. Duration: 4 hours.
Start/end date: cannot be determined. |
Changes in average quiz scores evaluating how to increase connection with a child, apply behavior modification skills, and coach a parent in these skills. Changes in observed enhancement skills and detraction behaviors utilized during patient interaction. |
2 |
Statistically significant increase in quiz scores post training session (P<0.001). Statistically significant increase in the number of enhancement skills (P<0.001) and statistically significant decrease in detraction behaviors demonstrated by residents during patient encounters (P<0.03). |
11 |
Strait & Bolman (2017)50 |
To assess the effectiveness of a TIC curriculum on enhancing the understanding of ACEs and TIC |
Students from nine health profession programs (N = 967) |
Pre-post |
Three small group training sessions with discussions. Duration: 6 hours. Start/end date: cannot be determined. |
Changes in self-reported knowledge of ACEs and TIC and confidence to incorporate TIC in practice. Note: Didn’t report on all measures assessed in survey. |
2 |
Increase in students who self-reported that they were extremely likely to administer and assess an ACE questionnaire (13.6% vs 42%); no statistical inference testing. Increase in the number of students reporting they are “somewhat confident” (37.3% vs 67.5%) or “extremely confident” (7.1% vs 16%) in knowing how to help patients after discussing trauma, and a decrease in the number of students reporting they were “not confident” (55.6% vs 16.6%); no statistical inference testing. |
7.5 |
Educational Intervention Format
Two-thirds of interventions used lectures to deliver the material.34,37,41-49 Six (40%) incorporated small-group discussions and/or breakout rooms.43,46-50 Four (26.7%) used standardized patients,36,41,42,45 three (20%) provided recommended supplemental readings/videos to review prior to the training session,42,46,47 three (20%) used electronic modules to deliver the training materials,35,38,48 one (6.6%) used skills training with coaching,44 and two (13.3%) used participant role-play scenarios.34,44.
Of the 15 interventions, 12 (80%) held the trainings in person,34,36,37,41-50 while three (20%) used a virtual format.35,38,43 A median of 2.5 hours (interquartile range, 1–4 hours) was spent on ACEs training topics and activities.
Outcomes and Key Findings
Table 1 outlines study characteristics, the types of outcomes assessed, corresponding Kirkpatrick model level, and key findings across the 15 studies. Of these, three studies were at Kirkpatrick level 3, and 12 were at Kirkpatrick level 2. None of the studies met the criteria for Kirkpatrick level 4.
Of the 15 articles, 13 (86.7%) included an assessment of knowledge with ACEs before and after completing the intervention.34-50 Eleven of these studies found an increase in self-assessed knowledge,34,35,37,38,41,43,44,46,47,48,50 and three found an increase in objectively assessed knowledge.44,45,49 Of the studies that evaluated for self-assessed knowledge, six studies found a statistically significant increase in knowledge,35,37,38,43,44,48 while four did not perform statistical inference testing,34,46,47,50 and one found no statistically significant changes.41 Additionally, one study found that participants who assessed their own ACEs score had enhanced understanding of the ACEs and trauma-informed care material.50 Of the studies that evaluated objective knowledge, two used multiple-choice quizzes44,49 and one assessed use of an ACE-related clinical skill set during standardized patient encounters.45
Eight articles (53.3%) assessed for changes in confidence and/or comfort levels with ACEs before and after the intervention.34-43,50 Five of these studies found a statistically significant increase in confidence and/or comfort levels following the curricula,35,36,38,42,43 and one study found no statistically significant change.41 Two studies reported an increase in confidence and/or comfort levels; however, no statistical inference testing was performed.34,50
Three articles (20%) evaluated changes in participant attitudes before and after completing the curriculum.35,43,46 Chokshi, Chen, and Beers (2020)35 found a statistically significant increase in learners’ attitudes as reflected by higher self-reported ratings regarding the importance of trauma screening, discussing trauma exposure and health outcomes with patients, and staff training opportunities on childhood trauma and resiliency (P<0.001). Pletcher et al46 found that students most prevalently reported that all components of the intervention contributed to a “considerable” change in their attitudes or perspectives related to ACEs with the exception of reading; however, no statistical testing was performed. Chokshi and Goldman43 found no statistically significant changes in pretest/posttest scores for attitudes, as measured by self-report on the importance of trauma screening, discussing links between trauma history and poor health outcomes, and ensuring staff training on trauma-informed care and resiliency (average P = 0.066).
Seven articles (46.7%) that assessed behavior changes regarding ACE evaluation and management reported increases in either objective observed behavior changes, self-reported behavior changes, or planned behavior changes. Three of these studies evaluated for planned behavior changes,35,47,50 with only one performing statistical inference testing.35 Two studies reported statistically significant increases in self-reported behavior changes,36,38 and one study reported an increase in objective behavior changes, though no statistical inference testing was performed.41 For ease of interpretation, Table 2 summarizes the direction of the findings across the four categories of identified outcomes, and their corresponding Kirkpatrick level, examined in the 15 studies.
Study |
Knowledge/skills |
Confidence/comfort |
Attitudes |
Behavior |
Objectivea |
Self-assessedb |
Objectivea |
Self-reportedc |
Plannedd |
KL 2 |
KL 2 |
KL 2 |
KL 2 |
KL 3 |
KL 3 |
KL 2 |
Chokshi, Chen, & Beers (2020)35 |
N/A |
+ |
+ |
+ |
N/A |
N/A |
+ |
Chokshi et al (2020)47 |
N/A |
‡ |
N/A |
N/A |
N/A |
N/A |
‡ |
Chokshi & Goldman (2021)43 |
N/A |
+ |
+ |
NS |
N/A |
N/A |
N/A |
Goldstein et al (2018)34 |
N/A |
‡ |
‡ |
N/A |
N/A |
N/A |
N/A |
Lloyd et al (2021)42 |
N/A |
N/A |
+ |
N/A |
N/A |
N/A |
N/A |
Marsh et al (2019)49 |
+ |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
Marsicek et al (2019)41 |
N/A |
NS |
NS |
N/A |
‡ |
N/A |
N/A |
Miller-Cribbs et al (2020)45 |
‡ |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
Morrison et al (2021)36 |
N/A |
N/A |
+ |
N/A |
N/A |
+ |
N/A |
Onigu-Otite & Idicula (2020)37 |
N/A |
+ |
N/A |
N/A |
N/A |
N/A |
N/A |
Osei et al (2022)48 |
N/A |
+ |
N/A |
N/A |
N/A |
N/A |
N/A |
Pletcher et al (2019)46 |
N/A |
‡ |
N/A |
‡ |
N/A |
N/A |
N/A |
Scott et al (2024)44 |
+ |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
Schmitz et al (2019)38 |
N/A |
+ |
+ |
N/A |
N/A |
+ |
N/A |
Strait & Bolman (2017)50 |
N/A |
‡ |
‡ |
N/A |
N/A |
N/A |
‡ |
Quality Assessment
The results of our quality assessment review using the MERSQI tool are described in Table 1 and Appendix 2. Scores ranged from 7.5 to 11.5, with nine of the 15 studies (60%) having scores less than or equal to 9, indicating low quality; and six (40%) studies with scores between 9.5 and 13, indicating moderate quality. Within the validity domain of the MERSQI tool, none of the studies fully validated their assessment tools concerning internal structure, content, and relationships to other variables. Two studies demonstrated validity in two domains,37,48 and five in one domain,34,36,42,44 while eight did not report using a validated instrument.34,35,37,38,41,43,46,48
This systematic review assessed the effectiveness of ACEs educational interventions implemented in US medical schools and residency programs. Our findings underscore wide variability in curriculum design, delivery methods, and measured outcomes, reflecting the complexity and evolving nature of ACEs education.
Compared to Ramesh et al,24 who identified 13 articles over 21 years, our review found 15 articles in the past 12 years, 10 of which were published after 2020. This rapid growth, especially post-COVID-19, aligns with our expectation of increasing interest in trauma-informed care. Like Ramesh et al (2020),24 we found most studies reported increases in ACEs knowledge. However, the overall lower methodological quality in our included studies, demonstrated by low MERSQI scores and frequent lack of statistical inference testing, underscores the need for enhanced rigor in future studies. Most studies relied on self-assessed knowledge immediately after the intervention, which has limitations in accurately capturing learning.51 Literature has suggested that self-assessment often leads to overestimations of knowledge and skills in medical trainees compared to objective testing.51-56
Our review also identified some differences from Ramesh et al24 Specifically, we observed that changes in attitudes and confidence varied considerably across intervention formats and durations, while knowledge outcomes were generally more consistent. This finding suggests that while knowledge can be effectively conveyed through a range of formats and shorter interventions, altering deeply held attitudes and sustaining confidence may require more intensive or prolonged interventions. Additionally, while Ramesh et al24 did not include studies examining behavior change, six studies in our review did, indicating higher Kirkpatrick levels of evaluation. However, most relied on self-reports of intention to change, making concluding whether these interventions will lead to long-term behavior changes challenging. Only one study objectively assessed longitudinal behavior changes,41 raising the question of how often these intentions are implemented and sustained.
Similarly, McBain et al (2023)25 found low-strength evidence in studies evaluating clinician knowledge and confidence due to self-assessment, small sample sizes, and single institution studies. Like our review, McBain et al25 identified lack of longitudinal objective data, underscoring the need for more rigorous research with controls, randomization, longitudinal follow-up, objective measurements, and validated tools.
Despite not limiting our search to a specific medical specialty, all included residency studies focused on primary care specialties (internal medicine, pediatrics, internal medicine-pediatrics, family medicine). Given ACEs affect over 65% of the US population,2 all physicians, regardless of specialty, will encounter individuals with ACE histories and would benefit from training on this topic.
A majority (66.7%) of the curricula reviewed relied on lecture formats. While lectures are a traditional method for conveying large amounts of information, incorporating more interactive elements such as small-group discussions, simulated patient interactions, role-play, and web-based modules could enhance the learning experience. These active-learning formats may not only foster a deeper understanding of ACEs, but also improve learners’ retention of information, confidence, and skills in addressing these issues in clinical practice.57,58,59
Three studies provided objective evaluations of knowledge gains. Scott et al44 found a statistically significant increase in knowledge based on multiple-choice quizzes administered immediately before and after the intervention. However, the lack of follow-up assessments limits conclusions about long-term retention. Marsh et al 49 found sustained knowledge improvements across a 6 week pediatrics rotation, and Miller-Cribbs et al45 offered a unique perspective by objectively evaluating skills after a 3 year longitudinal intervention. Although participants improved in explaining ACEs to patients, other behaviors such as screening and stigma reduction showed little change. Miller-Cribbs et al45 also identified a concerning trend that empathy and collaborative treatment planning decreased between residents’ first and fourth years of residency, suggesting potential challenges in maintaining the impact of these interventions over time.
Based on our findings, we propose two key recommendations to strengthen ACEs education and research:
Enhance methodological rigor. Our MERSQI assessment revealed that many existing studies lacked critical methodological elements that are necessary for interpreting their findings. To improve this issue, studies should include objective outcome measures, report response rates clearly, and aim to assess higher-level outcomes such as behavior change and clinical impact (Kirkpatrick levels 3 and 4). Incorporating multi-institutional approaches and randomized controlled trials also can help increase the generalizability of findings.
Incorporate longitudinal assessments. To better understand the long-term impact of ACEs education, future studies should evaluate outcomes at multiple points in time, ideally from early medical school through residency and into early clinical practice. Longitudinal follow-up would allow researchers to assess the educational impact of interventions, including whether early improvements in knowledge and confidence persist, evolve, or diminish. Additionally, tracking outcomes over time could reveal how ACEs education influences trainees’ clinical decision-making, communication skills, and patient interactions in real-world settings. These insights would be essential for informing curriculum development, identifying optimal timing for educational reinforcement, and ultimately ensuring that ACEs training leads to meaningful improvements in patient care.
Our study had some limitations. Notably, our focus on medical students and residents inherently excluded other health care clinicians, including fellows, attending physicians, advanced practice clinicians, psychologists, and social workers, which may limit generalizability to these groups.
Our review also had several key strengths. We provided an updated and comprehensive review of the literature on ACEs educational interventions focused on early and graduate medical education in the United States, using the Kirkpatrick model as a theoretical framework. Collaborating with a health sciences librarian allowed us to conduct a thorough search across multiple databases, ensuring a wide capture of relevant articles.60,61 Importantly, we also assessed the quality of research studies using the well-validated MERSQI tool, specifically geared to assess quality of medical education research.
Overall, our review presents encouraging evidence of a growing focus on ACEs in medical education. While the integration of ACEs training into medical education shows potential benefits in increasing knowledge and awareness, substantial room for improvement in how these trainings are conducted and evaluated remains. With interactive, longitudinal approaches and validated assessments, medical education programs can better prepare future physicians to recognize and manage ACEs, ultimately mitigating the health impacts of ACEs and improving patient outcomes.
References
-
-
Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. the adverse childhood experiences (ACE) Study.
Am J Prev Med. 1998;14(4):245–258. doi:10.1016/s0749-3797(98)00017-8
-
Petruccelli K, Davis J, Berman T. Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis.
Child Abuse Negl. 2019;97:104127. doi:10.1016/j.chiabu.2019.104127
-
Merrick MT, Ford DC, Ports KA, et al. Vital signs: estimated proportion of adult health problems attributable to adverse childhood experiences and implications for prevention - 25 States, 2015-2017.
MMWR Morb Mortal Wkly Rep. 2019;68(44):999–1005. doi:10.15585/mmwr.mm6844e1
-
Roberts BW. Caring for patients with adverse childhood experiences. Radiol Technol. 2019;91(2):141–157.
-
Boullier M, Blair M. Adverse childhood experiences.
Paediatrics and Child Health. 2018;28(3):132–137. doi:10.1016/j.paed.2017.12.008
-
Burkey MD, Ali T, Hobson B, Despins L, Sze S. Addressing adverse childhood experiences (ACEs) in BC: practical approaches. B C Med J. 2020;62(1):14–17.
-
Felitti VJ, Anda RF. The lifelong effects of adverse childhood experiences. : Chadwick DL, Giardino AP, Alexander R, Thackeray JD, Esernio-Jenssen D, eds. Chadwick’s Child Maltreatment: Sexual Abuse and Psychological Maltreatment. . 4th ed. STM Learning, Inc; 2014:203–215
-
Magen E, DeLisser HM. Best practices in relational skills training for medical trainees and providers: an essential element of addressing adverse childhood experiences and promoting resilience.
Acad Pediatr. 2017;17(7S):S102–S107. doi:10.1016/j.acap.2017.03.006
-
Marcoux TB Jr. Adverse childhood experiences and trauma informed care: treating the whole patient with a more complete osteopathic approach.
J Osteopath Med. 2021;121(9):763–769. doi:10.1515/jom-2020-0322
-
Strait J, Meagher S. Trauma-informed care in pediatrics: a developmental perspective in twelve cases with narratives.
Perm J. 2020;24(2). doi:10.7812/TPP/19.045
-
Kerker BD, Storfer-Isser A, Szilagyi M, et al. Do pediatricians ask about adverse childhood experiences in pediatric primary care?
Acad Pediatr. 2016;16(2):154–160. doi:10.1016/j.acap.2015.08.002
-
-
Popp TK, Geisthardt C, Bumpus EA. Pediatric practitioners’ screening for adverse childhood experiences: current practices and future directions.
Soc Work Public Health. 2020;35(1-2):1–10. doi:10.1080/19371918.2020.1711839
-
Bora N, Jones TR, Salada K, Brummel M. Inter-clinician variability in primary care providers’ adverse childhood experience knowledge, training, screening practices, and perceived intervention barriers: an exploratory cross-sectional study.
J Child Adolesc Trauma. 2022;15(2):285–296. doi:10.1007/s40653-021-00365-x
-
Farrow VA, Bosch J, Crawford JN, Snead C, Schulkin J. Screening for history of childhood abuse: beliefs, practice patterns, and barriers among obstetrician-gynecologists.
Womens Health Issues. 2018;28(6):559–568. doi:10.1016/j.whi.2018.09.001
-
Stork BR, Akselberg NJ, Qin Y, Miller DC. Adverse childhood experiences (ACEs) and community physicians: what we’ve learned.
Perm J. 2020;24(2). doi:10.7812/TPP/19.099
-
Loe IM, Froehlich TE, Edrees HH, Spinks-Franklin A, Collaborative R. Racism as an adverse childhood experience: an interactive workshop to train pediatricians to address racism in clinical care.
J Dev Behav Pediatr. 2021;42(6):502–511. doi:10.1097/DBP.0000000000000984
-
Burns CJ, Borah L, Terrell SM, James LN, Erkkinen E, Owens L. Trauma-informed care curricula for the health professions: a scoping review of best practices for design, implementation, and evaluation.
Acad Med. 2023;98(3):401–409. doi:10.1097/ACM.0000000000005046
-
Collins K, Spice C, Ingraham BC, Al Achkar M. Family medicine resident knowledge of adverse childhood experiences.
PRiMER. 2021;5. doi:10.22454/PRiMER.2021.971170
-
Tan J, Dube SR. A Pilot study on the awareness and knowledge of adverse childhood experiences science and trauma-informed care among medical school students.
Perm J. 2021;25(3). doi:10.7812/TPP/20.285
-
Koo A, Irwin J, Sturgis M, et al. Is academic medicine prepared to teach about the intersection of childhood experiences and health? an exploratory survey of faculty.
J Contin Educ Health Prof. 2023;43(4):225–233. doi:10.1097/CEH.0000000000000489
-
Liabsuetrakul T, Sirirak T, Boonyapipat S, Pornsawat P. Effect of continuous education for evidence-based medicine practice on knowledge, attitudes and skills of medical students.
J Eval Clin Pract. 2013;19(4):607–611. doi:10.1111/j.1365-2753.2012.01828.x
-
Ramesh A, Juarez PD, Paul MJ, et al. Curricular interventions in medical schools for assessing adverse childhood experience.
J Health Care Poor Underserved. 2020;31(4S):68–90. doi:10.1353/hpu.2020.0138
-
McBain RK, Levin JS, Matthews S, et al. The effect of adverse childhood experience training, screening, and response in primary care: a systematic review.
EClinicalMedicine. 2023;65. doi:10.1016/j.eclinm.2023.102282
-
Bryant DJ, Oo M, Damian AJ. The rise of adverse childhood experiences during the COVID-19 pandemic.
Psychol Trauma. 2020;12(S1):S193–S194. doi:10.1037/tra0000711
-
Hertz M, Heim Viox M, Massetti GM, et al. Adverse childhood experiences among US adolescents over the course of the COVID-19 Pandemic.
Pediatrics. 2023;151(6). doi:10.1542/peds.2022-060799
-
Anderson KN, Swedo EA, Trinh E, et al. Adverse childhood experiences during the COVID-19 Pandemic and associations with poor mental health and suicidal behaviors among high school students - adolescent behaviors and experiences survey, United States, January-June 2021.
MMWR Morb Mortal Wkly Rep. 2022;71(41):1301–1305. doi:10.15585/mmwr.mm7141a2
-
Restini C, Faner M, Miglio M, Bazzi L, Singhal N. Impact of COVID-19 on medical education: a narrative review of reports from selected Countries.
J Med Educ Curric Dev. 2023;10. doi:10.1177/23821205231218122
-
-
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.
BMJ. 2021;372. doi:10.1136/bmj.n71
-
Rethlefsen ML, Kirtley S, Waffenschmidt S, et al. PRISMA-S: an extension to the PRISMA Statement for reporting literature searches in systematic reviews.
Syst Rev. 2021;10(1). doi:10.1186/s13643-020-01542-z
-
Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. . Cochrane; 2023.
-
Goldstein E, Murray-García J, Sciolla AF, Topitzes J. Medical students’ perspectives on trauma-informed care training.
Perm J. 2018;22(1). doi:10.7812/TPP/17-126
-
Chokshi B, Chen K-LD, Beers L. Interactive case-based childhood adversity and trauma-informed care electronic modules for pediatric primary care.
MedEdPORTAL. 2020;16. doi:10.15766/mep_2374-8265.10990
-
Morrison JM, Marsicek SM, Hopkins AM, Dudas RA, Collins KR. Using simulation to increase resident comfort discussing social determinants of health.
BMC Med Educ. 2021;21(1). doi:10.1186/s12909-021-03044-5
-
Onigu-Otite E, Idicula S. Introducing ACEs (Adverse Childhood Experiences) and resilience to first-year medical students.
MedEdPORTAL. 2020;16. doi:10.15766/mep_2374-8265.10964
-
Schmitz A, Light S, Barry C, Hodges K. Adverse childhood experiences and trauma-informed care: an online module for pediatricians.
MedEdPORTAL. 2019;15. doi:10.15766/mep_2374-8265.10851
-
-
Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Association between funding and quality of published medical education research.
JAMA. 2007;298(9):1002–1009. doi:10.1001/jama.298.9.1002
-
Marsicek SM, Morrison JM, Manikonda N, O’Halleran M, Spoehr-Labutta Z, Brinn M. Implementing standardized screening for adverse childhood experiences in a pediatric resident continuity clinic.
Pediatr Qual Saf. 2019;4(2). doi:10.1097/pq9.0000000000000154
-
Lloyd MC, Ratner J, La Charite J, et al. Addressing trauma and building resilience in children and families: standardized patient cases for pediatric residents.
MedEdPORTAL. 2021;17. doi:10.15766/mep_2374-8265.11193
-
Chokshi B, Goldman E. Using trauma-informed care in practice: evaluation of internal medicine resident training and factors affecting clinical use.
Perm J. 2021;25(4). doi:10.7812/TPP/21.032
-
Scott BB, Kelley L, Schilling S. Skills training for family medicine residents to attenuate the impact of childhood trauma: a pilot study.
Fam Med. 2024;56(3):180–184. doi:10.22454/FamMed.2024.245065
-
Miller-Cribbs J, Bragg J, Wen F, et al. An evaluation of a simulation and video-based training program to address adverse childhood experiences.
Int J Psychiatry Med. 2020;55(5):366–375. doi:10.1177/0091217420951064
-
Pletcher BA, O’Connor M, Swift-Taylor ME, DallaPiazza M. Adverse childhood experiences: a case-based workshop introducing medical students to trauma-informed care.
MedEdPORTAL. 2019;15. doi:10.15766/mep_2374-8265.10803
-
Chokshi B, Walsh K, Dooley D, Falusi O, Deyton L, Beers L. Teaching trauma-informed care: a symposium for medical students.
MedEdPORTAL. 2020;16. doi:10.15766/mep_2374-8265.11061
-
Osei A, Paz CG, Stuparich M, et al. Screening for toxic stress response and buffering factors: a case-based, trauma-informed approach to health equity.
MedEdPORTAL. 2022;18. doi:10.15766/mep_2374-8265.11224
-
Marsh MC, Supples S, McLaurin-Jiang S, Brown CL, Linton JM. Introducing the concepts of advocacy and social determinants of health within the pediatric clerkship.
MedEdPORTAL. 2019;15. doi:10.15766/mep_2374-8265.10798
-
Strait J, Bolman T. Consideration of personal adverse childhood experiences during implementation of trauma-informed care curriculum in graduate health programs.
Perm J. 2017;21(1). doi:10.7812/TPP/16-061
-
Jones R, Panda M, Desbiens N. Internal medicine residents do not accurately assess their medical knowledge.
Adv in Health Sci Educ. 2008;13(4):463–468. doi:10.1007/s10459-007-9058-2
-
-
Von Hoyer J, Bientzle M, Cress U, Grosser J, Kimmerle J, Holtz P. False certainty in the acquisition of anatomical and physiotherapeutic knowledge.
BMC Med Educ. 2022;22(1). doi:10.1186/s12909-022-03820-x
-
-
Rahmani M. Medical trainees and the dunning-kruger effect: when they don’t know what they don’t know.
J Grad Med Educ. 2020;12(5):532–534. doi:10.4300/JGME-D-20-00134.1
-
Pitter D, Indelicato AM, Morley CP, Feuerstein B, Weinstock RS. US fourth-year medical students: diabetes knowledge and confidence dissonance.
PRiMER. 2024;8. doi:10.22454/PRiMER.2024.497586
-
Miller CJ, McNear J, Metz MJ. A comparison of traditional and engaging lecture methods in a large, professional-level course.
Adv Physiol Educ. 2013;37(4):347–355. doi:10.1152/advan.00050.2013
-
Nestel D, Tierney T. Role-play for medical students learning about communication: guidelines for maximising benefits.
BMC Med Educ. 2007;7(1). doi:10.1186/1472-6920-7-3
-
Subramanian A, Timberlake M, Mittakanti H, Lara M, Brandt ML. Novel educational approach for medical students: improved retention rates using interactive medical software compared with traditional lecture-based format.
Journal of Surgical Education. 2012;69(4):449–452. doi:10.1016/j.jsurg.2012.05.013
-
Rethlefsen ML, Brigham TJ, Price C, et al. Systematic review search strategies are poorly reported and not reproducible: a cross-sectional metaresearch study.
J Clin Epidemiol. 2024;166:111229. doi:10.1016/j.jclinepi.2023.111229
-
Pawliuk C, Cheng S, Zheng A, Siden HH. Librarian involvement in systematic reviews was associated with higher quality of reported search methods: a cross-sectional survey.
J Clin Epidemiol. 2024;166:111237. doi:10.1016/j.jclinepi.2023.111237



There are no comments for this article.