Background and Objectives: Accelerated 3-year programs (A3YPs) for an MD degree offer a condensed medical education pathway to residency, often with directed pathways in primary care. Many programs aim to address workforce shortages and decrease debt. As these programs expand, assessing whether A3YP graduates are as prepared for residency as their peers from traditional 4 year programs is critical. This study evaluates milestone attainment of A3YP postgraduates in Year 1 (PGY-1s) compared to non-A3YP PGY-1s within family medicine residency programs.
Methods: We analyzed the Accreditation Council for Graduate Medical Education milestone ratings for family medicine PGY-1s from 2021 to 2023. The study included 109 A3YP graduates across 51 family medicine programs and 1,638 non-A3YP PGY-1s (MD, DO, international medical graduate) in those same programs. PGY-1s were compared across milestone competency domains using mixed-effects regression that accounted for clustering by program and subcompetency.
Results: At midyear, A3YP PGY-1s scored significantly higher in medical knowledge, systems-based practice, and practice-based learning and improvement. Differences were statistically significant but modest. Coefficients ranged from 0.05 for patient care and medical knowledge to 0.10 for practice-based learning and improvement (PBLI; P<0.01). At end-year, A3YP PGY-1s maintained slightly higher scores in medical knowledge, professionalism, PBLI, and communication (coefficients ranged from 0.07 to 0.10; P<0.01).
Conclusions: A3YP graduates demonstrate equal or minimally higher milestone attainment compared to non-A3YP peers during PGY-1, supporting the viability of accelerated pathways. These findings reassure residency programs of A3YP readiness and highlight their potential to address workforce shortages and reduce student debt without compromising educational outcomes.
Accelerated 3-year medical school programs (A3YPs) allow students to achieve an MD degree in 3 years instead of 4 years through a compressed timeline. These programs have seen large growth over the last decade. Currently, close to 40 institutions in the United States either have or are developing an A3YP, and more than 80% are directly linked to family medicine.1 In 2015, a Consortium of Accelerated Medical Pathway Programs (CAMPP) was started, organizing and supporting the increasing number of A3YP schools. Per Cangiarella et al, as of 2024, more than 1,000 students have graduated from accelerated programs.2 Most of the programs have a directed pathway to an affiliated graduate medical education (GME) with a focus on primary care. A directed pathway is where students still enter the official match but are ranked to match with a given residency program, should they choose to rank there. The selection process for primary care A3YPs tends to focus on commitment to specialty as a key driver for admission.3
Given that students from A3YPs enter the residency match alongside peers from traditional 4 year academic programs (MDs, international medical graduates [IMGs], and DOs), ensuring that A3YP graduates are as prepared for residency as the rest of their PGY-1 (intern) residency cohort is important. Recent outcomes from 3 year MD programs have demonstrated that A3YP graduates are equally prepared for starting residency and achieve similar performance, as outlined next.
Leong et al reported that A3YP students were as satisfied with the quality of their education and felt as prepared for residency based on Association of American Medical Colleges graduation questionnaire data.4 Students from A3YPs reported a more positive learning climate (faculty interactions and emotional climate). Students from A3YPs had less debt, and more planned to care for underserved populations and practice primary care.5 Studies of several programs have shown that academic performance was similar across multiple data points.6,7 PGY-1 milestone ratings for A3YP and non-A3YP from the same medical school were found to be equivalent for mid- and end-year of internship in six specialties (internal medicine, emergency medicine, family medicine, general surgery, psychiatry, and pediatrics) in 2021–2022.8 These studies provide evidence that student performance in medical school is equal to that of non-A3YP learners. An area that has not yet been evaluated is the performance of these A3YP graduates compared to non-A3YP graduates within the same residency program and specialty.
Due to the condensed structures of their curricula, ensuring that students from A3YPs are as prepared for residency as their non-A3YP counterparts is important. Students in A3YPs tend to have little to no elective time and less time to prepare for US medical licensing exams, though most require the same primary assessments and objectives. One outcome to consider is how A3YP PGY-1s perform versus non-A3YP PGY-1s on ACGME milestones. Longitudinal milestones help to assess areas of competency and domains for improvement for residents and are an integral part of a resident assessment of specific behaviors and skills.9 In this paper we compare the milestone achievement of A3YPs versus non-A3YP PGY-1s in the same GME program at 6 and 12 months of residency to assess whether A3YP PGY-1s attain at least the same milestones as non-A3YP PGY-1s. With the rapid growth of A3YPs, family medicine residencies will most certainly encounter residents from A3YPs, and ensuring that family medicine residency educators are confident that the learners they are accepting into their program have the chance to be as successful as their non-A3YP residents is important. This study adds to the growing body of literature supporting equal preparation and attainment of knowledge, skills, and behaviors compared to non-A3YPs.
Participants
We included only residency programs with at least one PGY-1 from an A3YP. Subjects were A3YP medical school graduates in 2021, 2022, and 2023 (three cohorts) who were compared to all other graduates in the same residency program. These included traditional 4-year MD, DO, and IMG graduates at the residency program that accepted A3YP graduates. The research group of the Consortium of Accelerated Medical Pathway Program provided the residents’ name, medical school, residency program, and National Provider Identifier for matching to their milestones in the ACGME accreditation data system. We were able to identify 97.3% of A3YP graduates.
Study Design
We used a retrospective case-controlled comparison study design, hypothesizing that matched PGY-1s from A3YPs were comparable to other matched PGY-1s in their residency milestone scoring.8 The outcome was based on the milestone scoring that residency programs submitted to ACGME, which has years of validity evidence since its launch more than a decade ago.10,11,12 The milestone assessment system includes the competency domains of medical knowledge (MK), patient care (PC), interpersonal and communication skills (ICS), professionalism (PROF), systems-based practice (SBP), and practice-based learning and improvement (PBLI).13 Residents are assessed from level 1 (resident demonstrates performance expected of an incoming resident) to level 5 (advanced performance demonstrating aspirational goals beyond graduation target) with 0.5 intervals between the levels. Level 4 (labeled as proficiency) is designated as the target for residents by the time of graduation. Programs also can indicate that the residents were not assessed and have not yet achieved level 1. Programs report all subcompetencies for each 6 month reporting period (midyear reporting period in December and end-year reporting period in June). Milestone assignment decisions are based on consensus of the clinical competency committee and the program director. Each competency domain, for example MK, has several subcompetency descriptions of the knowledge and skills. Subcompetency scores were aggregated at the competency domain level, generating six core competency milestone scores for PC, MK, ICS, PROF, PBLI, and ICS. For the purpose of this paper, we refer to the aggregated subcompetency ratings of the competency domains as milestones.
Analysis
We used descriptive statistics and box plots to examine data trends between treatment of A3YP and non-A3YP residents. The data used in this project included graduates from medical schools that matched into different family medicine programs. Performance of graduates from discrete medical schools as well as residency programs is different and needs to be considered. Therefore, the analysis created a cross-classification matrix of varying learners clustered within medical schools to matriculate into different residency programs that also have varying program-specific variance. To account for both school and residency program effects (medical school-specific variability and residency program-specific variability), we used cross-classified random-effects regression to account for clustering and to estimate group differences. An indicator variable for A3YP was created as a binary factor (1 = A3 YP, 0 = not A3YP) to examine milestone differences. We used unstandardized coefficients to interpret findings—that is, the impact of A3YP on first-year residency milestone residency ratings for PC, MK, ICS, PROF, PBLI, and ICS. A two-sided P<0.05 was considered statistically significant. Secondary analysis compared A3YP and US MD non-A3YP PGY-1s using the same methodology.
The analysis was performed in collaboration with ACGME (Y.S.P. and S.O.H.). Data compilation and analyses were conducted using Stata software version 18/MP (StataCorp). The University of Illinois at Chicago Institutional Review Board approved this study.
The 109 A3YP family medicine PGY-1s from 13 medical schools matched to 51 unique residency programs. We compared these to the all the non-A3YP PGY1 (1,638 residents) from those same programs (Table 1). Included were 156 US medical schools accredited by the Liaison Committee on Medical Education, 40 osteopathic medicine schools accredited by the Commission on Osteopathic College Accreditation, and 119 non-US medical schools. The majority of non-A3YP (59%) graduated from US MD schools.
|
2020 |
2021 |
2022 |
2023 |
Total |
A3YP |
18 |
17 |
39 |
35 |
109 |
Doctor of osteopathic medicine |
99 |
78 |
95 |
102 |
374 |
International medical graduates |
78 |
69 |
72 |
77 |
296 |
US medical degree |
234 |
275 |
236 |
223 |
968 |
Descriptive Statistics
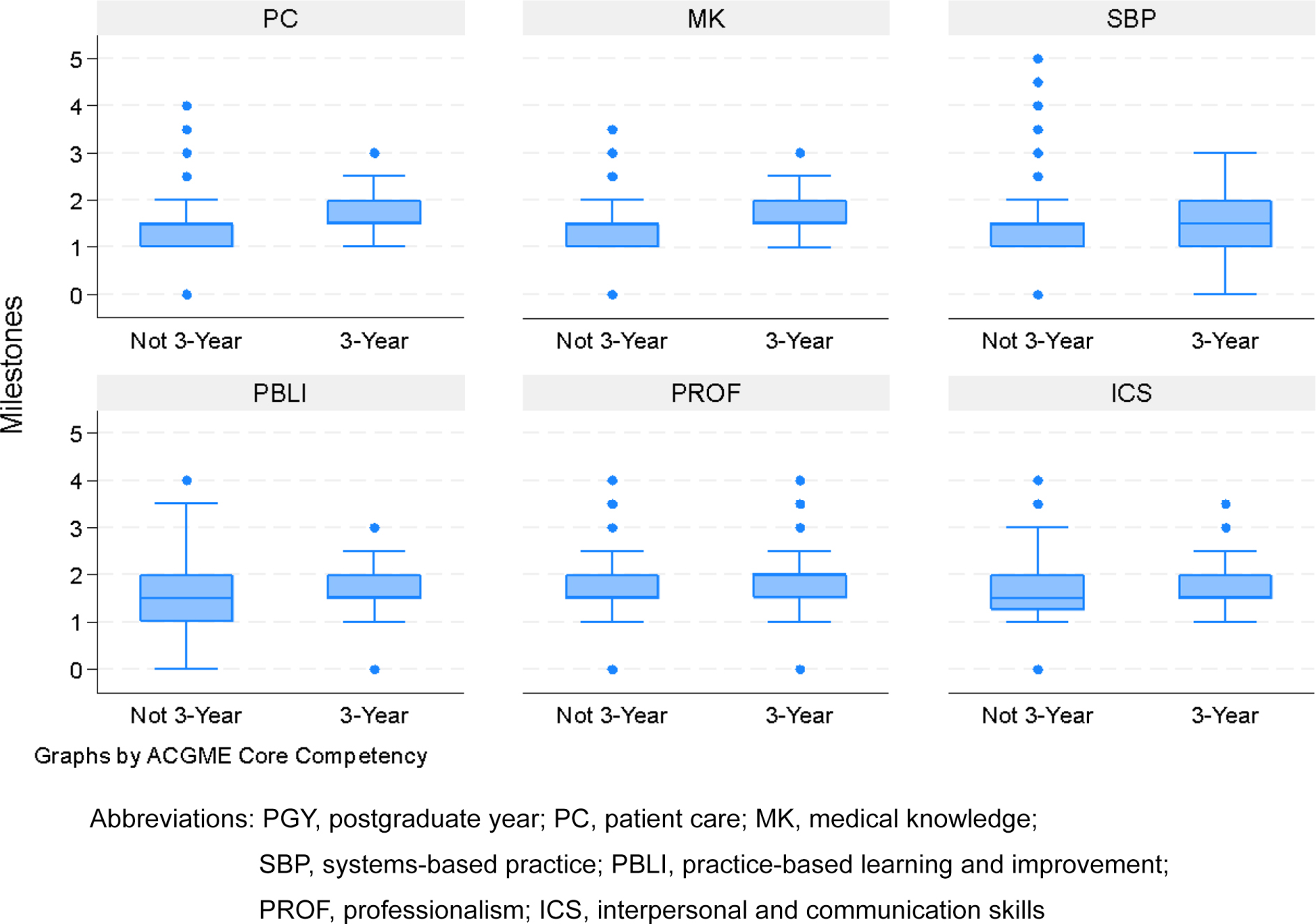
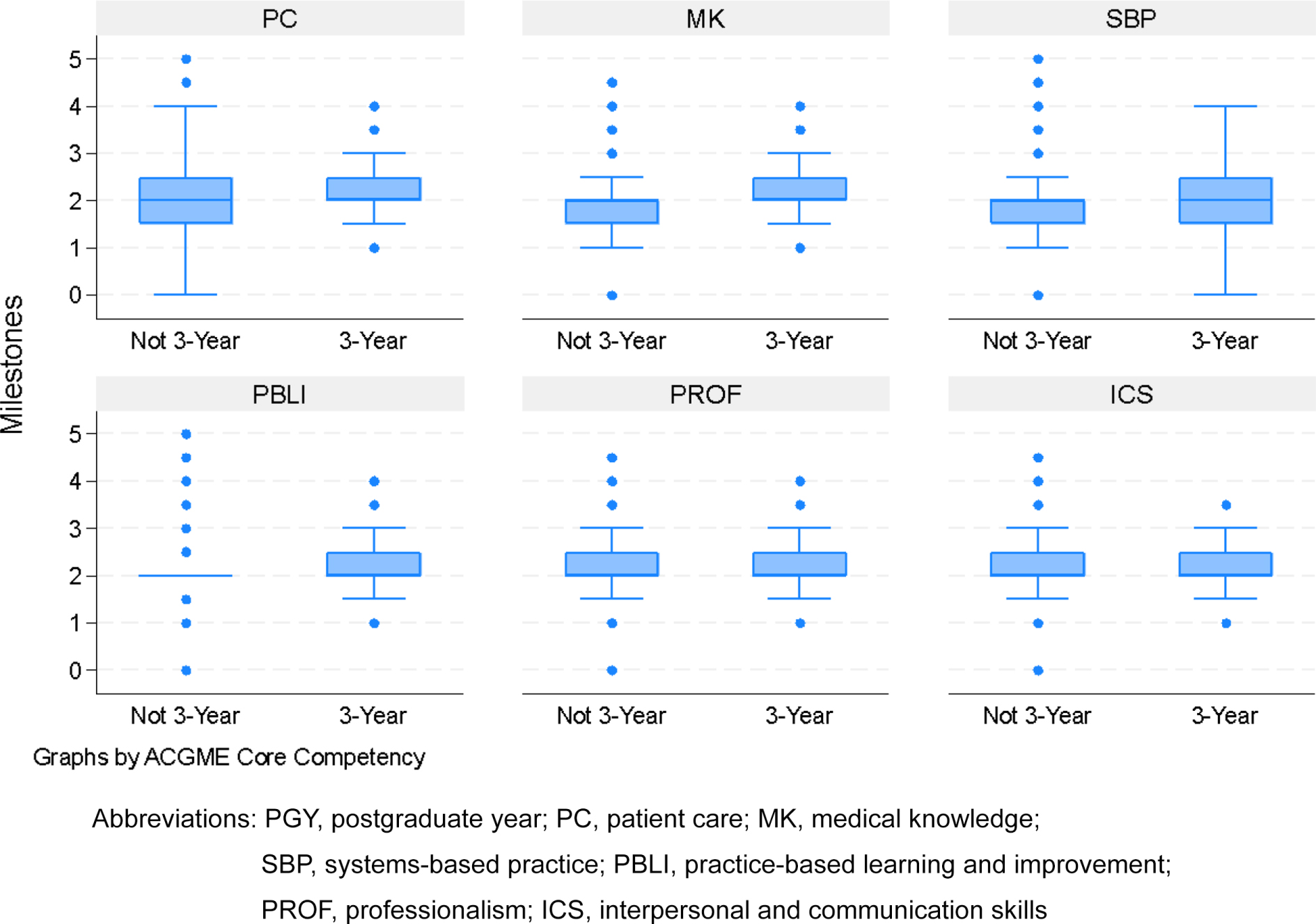
Overall, milestone ratings during PGY-1 midyear and end-year reporting periods are comparable with interquartile ranges overlapping between the A3YP and non-A3YP groups. See Figures 1 and 2 for box plots of both A3YP and non-A3YP PGY-1. Figure 1, midyear competency ratings, demonstrates the mean and interquartile ranges for each competency domain. These box and whisker plots show overlapping values and demonstrate the similarity on milestone assessments between the two cohorts. Figure 2 shows the end-year competency ratings where the mean rating is expectedly higher for both cohorts. The box plots are similar for A3YP and non-A3YP cohorts. More variability existed in the performance of the non-A3YP PGY-1 possibly due to more variability in medical schools (US MD, DO, IMG).
Comparison Between A3YP and Non-A3YP PGY-1s
We next completed the cross-classification analysis, taking into account both medical school and residency to determine whether differences existed between A3YP and non-A3YP PGY-1s. Table 2 shows differences in milestone ratings between groups. The table represents the results of this regression analysis examining differences in milestone ratings between A3YP and non-A3YP PGY-1s at midyear and end-year training. The analysis accounted for clustering by medical school and residency programs. The significant findings are bolded. Positive coefficients indicate higher milestone ratings for A3YP PGY-1s compared to non-A3YP PGY-1s. For PC, MK, SBP, and PBLI at midyear, the A3YP PGY-1s were slightly better than the other PGY-1s (coefficient range 0.5 to 0.9). At end-year assessment, we found similar small differences in MK, PBLI, PROF, and ICS. This type of analysis demonstrates effect size through the coefficients. To interpret the coefficient estimate of 0.10, for example, A3YP PGY-1s were scored 0.1 milestone units higher on the PBLI compared to the non-A3YP PGY-1s; P<0.001. Therefore, the associated effect of being A3YP residents was to have a 0.1 higher score on the milestones. The secondary analysis comparing A3YP and US MD non-A3YP residents had a smaller sample size and showed significant coefficients for ICS at midyear and MK at end of year (Table 3).
|
Midyear |
End-year |
Competency |
Coef |
SE |
P value |
Coef |
SE |
P value |
PC |
0.05 |
(0.02) |
.013 |
0.05 |
(0.03) |
.161 |
MK |
0.05 |
(0.02) |
.002 |
0.07 |
(0.03) |
.022 |
SBP |
0.09 |
(0.03) |
.006 |
0.05 |
(0.03) |
.080 |
PBLI |
0.10 |
(0.03) |
<0.001 |
0.07 |
(0.03) |
.006 |
PROF |
0.04 |
(0.02) |
.068 |
0.10 |
(0.03) |
<0.001 |
ICS |
0.04 |
(0.02) |
.074 |
0.07 |
(0.02) |
.004 |
|
Midyear |
End-year |
Competency |
Coef |
SE |
P value |
Coef |
SE |
P value |
PC |
0.03 |
(0.02) |
.170 |
0.03 |
(0.02) |
.139 |
MK |
0.05 |
(0.03) |
.169 |
0.06 |
(0.03) |
.027 |
SBP |
0.02 |
(0.02) |
.362 |
0.02 |
(0.02) |
.308 |
PBLI |
0.03 |
(0.04) |
.440 |
0.05 |
(0.03) |
.067 |
PROF |
0.03 |
(0.03) |
.285 |
0.04 |
(0.03) |
.099 |
ICS |
0.08 |
(0.03) |
.007 |
0.04 |
(0.02) |
.130 |
The mean value for each of the six competency domain assessments was higher for the A3YP PGY-1s compared to the non-A3YP PGY-1s at the midyear point. Controlling for program, A3YP PGY-1s had statistically significantly higher milestone assessments at 6 months compared to non-A3YP PGY-1s in all competency domains except PROF and ICS. Additionally, A3YP PGY-1s had statistically significantly higher milestone assessments at end-year compared to non-A3YP PGY-1s in all competency domains except for PC and SBP. When comparing the smaller sample of US MD graduates, the only differences were in ICS at midyear and MK at end-year.
The differences in the competency domain assessments were demonstrated by the coefficients, which indicate the size of the effect of the A3YP compared to the non-A3YP. At 6 months, the coefficients ranged from 0.05 for PC and MK to 0.10 for PBLI. In other words, the milestones were 0.10 points higher for A3YP PGY-1s than for non-A3YP PGY-1s while accounting for the program. Whether the coefficients are educationally significant is difficult to know. While the results showed statistically significance achievement in all milestones, these differences may not be educationally significant.
If these differences are meaningful, we offer several reasons that A3YP PGY-1s may have had higher scores. Learners in A3YPs often have earlier and more sustained clinical exposure, which is more in alignment with their planned field of residency over their 3 years. This could lead to improved performance on milestones. Possibly students in A3YPs perform better on milestones because they are committed to their specialty and train for the known specialty while in medical school—in essence training to be a better family physician versus a learner who is training to be a better medical student and, in theory, a better physician; however, more study would be needed to confirm this hypothesis. Additionally, an interesting observation is the higher degree of dispersion (variability) among the non-A3YP PGY-1s (demonstrated in the box plots) compared to the A3YP PGY-1s. We hypothesize that this was due to the structure of A3YP programs and directed pathways (linking of undergraduate medical education and GME); the GME programs know the students better before they enter and therefore have a lower variability among the assignment of milestones. This possibility requires additional evaluation and study to understand the program impact.
Medical schools are currently grappling with key issues, including medical student debt and workforce shortages, while addressing the need to incorporate competency-based education and emerging technology innovations. A3YPs demonstrate a viable pathway to reducing medical student debt and reducing workforce shortages with equal or better attainment of milestones during the PGY-1 year. More than 80% of the A3YPs have family medicine as a specific specialty with a directed pathway to residency. This means that medical students can train in the same institution to which they ultimately match for residency. The structure of accelerated programs typically includes earlier and more frequent integration into the clinical setting compared to the structures for 4 year students. This structure may account for the higher initial scores in several domains of competency. When students reach residency, they are known by the faculty, they know the clinics and procedures, and integration into residency has a less steep learning curve. Interestingly, at the end of the year, different milestones were statistically significant, although all coefficients were still higher than students who participated in 4 year programs. PC and SBP were no longer statistically significant, which suggests that the structural benefit of having trained where you do residency diminishes over time.
Additional elements that possibly support improved PGY-1 milestone ratings are that A3YP students do not have a significant break between core medical school content and the start of residency. While many non-A3YP students do pursue electives throughout their training, a several month gap is typical between clinical experiences and residency, which could allow an erosion of certain competencies.
This study had several limitations to consider. First, milestones rely on assessments of the learners by residency program directors and competency committees. The milestone assessments submitted to ACGME have inherent limitations. In programs where the residents are medical student trainees, prior knowledge of the student may result in a favorable bias when assessing the initial milestones. Additionally, ascribing a relationship between milestone ratings and actual patient care outcomes is difficult. The small sample size of family medicine A3YPs should be considered; while several milestones demonstrated statistical significance, the impact of these differences in ratings is uncertain. Finally, because the A3YP sample was relatively small; the results may be influenced by outliers in milestone reporting.
Future studies should consider longitudinal assessments of milestones to identify whether the increases are sustained over time. As the cohorts of A3YPs grow, more family medicine residents from A3YP curricula will match into programs outside of their medical school institution. Once sample size is big enough to determine the milestones of those students and whether they also demonstrate increased milestone attainment, considering a similar study will be important. Additionally, a qualitative or mixed-methods evaluation would help to further understand the variability in the milestones, faculty and student experience, and impact on education.
A3YPs prepare students equally for residency training as evidenced by similar attainment of milestone ratings at 6 and 12 months. Therefore, these programs may be a viable curricular option, especially for specialties such as family medicine, where a workforce shortage is projected.
Catherine L. Coe’s work previously started while at the Department of Family Medicine, University of North Carolina School of Medicine, Chapel Hill, NC.
We acknowledge the Medical Education Research and Program Evaluation of the American Medical Association (AMA) for partial support and ACGME for support in pulling data, merging the dataset, and analysis. The thoughts and ideas expressed in this article are those of the authors and may not represent official AMA policy (J.R.).
References
-
Coe CL, Santen SA, Reboli AC, et al. Accelerated 3YMD programs: the last decade of growth of the Consortium of Accelerated Medical Pathway Programs (CAMPP).
Med Educ Online. 2024;29(1). doi:10.1080/10872981.2024.2400394
-
Cangiarella J, Gonzalez-Flores A, Fancher TL, Santen SA, Coe CL. Accelerated 3-year MD programs in the United States: key features, innovations, growth, outcomes, and lessons learned.
Acad Med. 2025;100(5):536–540. doi:10.1097/ACM.0000000000005981
-
Tran-Reina ML, Hollander-Rodriguez J, Fancher TL, Roberts C, Co JPT, Coe CL. Training more physicians for medically underserved communities: the power of regional medical education collaboratives across the training continuum.
J Grad Med Educ. 2025;17(2 Suppl):19–23. doi:10.4300/JGME-D-24-00476.1
-
Leong SL, Gillespie C, Jones B, et al. Accelerated 3-year MD pathway programs: graduates’ perspectives on education quality, the learning environment, residency readiness, debt, burnout, and career plans.
Acad Med. 2022;97(2):254–261. doi:10.1097/ACM.0000000000004332
-
Santen SA, Gonzalez-Flores A, Coe CL, et al. Return on investment of three-year accelerated programs for students, medical schools, departments, and community.
Med Sci Educ. 2024;34(4):919–925. doi:10.1007/s40670-024-02043-7
-
Cangiarella J, Eliasz K, Kalet A, Cohen E, Abramson S, Gillespie C. A preliminary evaluation of students’ learning and performance outcomes in an accelerated 3-year MD pathway program.
J Grad Med Educ. 2022;14(1):99–107. doi:10.4300/JGME-D-21-00284.1
-
Chen F, Jordan KA, Li W, Lam Y, Pascarella L, Coe CL. Academic performance of students in an accelerated medical pathway.
Med Educ Online. 2024;29(1). doi:10.1080/10872981.2024.2345444
-
Santen SA, Yingling S, Hogan SO, et al. Are they prepared? comparing intern milestone performance of accelerated 3-year and 4-year medical graduates.
Acad Med. 2024;99(11):1267–1277. doi:10.1097/ACM.0000000000005855
-
Holmboe ES, Yamazaki K, Nasca TJ, Hamstra SJ. Using longitudinal milestones data and learning analytics to facilitate the professional development of residents: early lessons from three specialties.
Acad Med. 2020;95(1):97–103. doi:10.1097/ACM.0000000000002899
-
-
-
Park YS, Hamstra SJ, Yamazaki K, Holmboe E. Longitudinal reliability of milestones-based learning trajectories in family medicine residents.
JAMA Netw Open. 2021;4(12). doi:10.1001/jamanetworkopen.2021.37179
-



There are no comments for this article.