Designed as a scholarship pathway for research-curious faculty clinicians in a combined academic family medicine/public health department, the Clinician Scholars Program is a structured engagement between clinicians and research faculty who collaborate on two research projects over 1 to 2 years with support from master-level research staff. The program covers academic time of both the clinician and the research faculty without reduction of salary level, and it provides teams with research funds and dedicated staff effort. Five clinicians completed the 2-year pilot program; outcomes thus far include five manuscripts, one internal grant, and acceptance of one clinician into an institutional 2-year research mentoring program toward the development of a National Institutes of Health career development (K) proposal. Funded in part by a department-level endowment and independent of other institutional and national research pathways programs, the Clinician Scholars Program shows promise in building family medicine research capacity and fostering collaboration between clinicians and research faculty.
The Department of Family Medicine and Public Health (DFMPH) at the University of Utah includes the Division of Family and Community Medicine, composed primarily of clinician faculty (physicians and advanced practice clinicians), and the Division of Public Health, where most faculty are nonclinician researchers. At program launch, DFMPH had 49 faculty in Family and Community Medicine, 18 in Public Health, and 17 in the Division of Physician Assistant Studies, which has since become a stand-alone entity.
Although DFMPH routinely ranks among the top five family medicine departments for National Institutes of Health (NIH) funding, most extramurally funded research is led by Public Health faculty, with limited participation from Family and Community Medicine clinicians. This pattern of strong departmental research with limited clinician engagement is common in academic family medicine.1,2 Strengthening primary care research increasingly requires participation from practicing clinicians who contribute clinically grounded research perspectives.3-5 National6-11 and departmental12,13 initiatives have developed mentoring programs and structured pathways for clinicians interested in research while maintaining clinical roles.
The Clinician Scholars Program at DFMPH was designed to increase collaboration between clinical and research divisions and provide structured research mentoring for clinicians. The program launched as a pilot in 2022 with five clinician faculty.
The program has no relationship with the National Clinician Scholars Program;6,14 the similarity in name is coincidental. Evaluation of the pilot was exempted by the University of Utah Institutional Review Board (IRB 00130505).
The Clinician Scholars Program is a structured collaboration between clinician faculty (“scholars”) and research faculty (“mentors”) that runs for 1 year with the option for renewal.
Research teams are organized as pods consisting of two scholars, one mentor, and shared departmental research staff (clinical research coordinator and biostatistician). Pods meet biweekly to review progress and address methodological or logistical issues. Within the pod structure, each scholar participates in the mentor’s research activities and peer-mentors the second scholar in the pod. Pods were designed so that scholars can observe one another’s progress and provide guidance. Although scholars receive no formal training in peer mentoring, the structure creates opportunities to practice giving and receiving feedback.
Each scholar completes two projects mutually agreed upon with the mentor prior to program entry. A secondary data analysis, typically using the mentor’s project data or public datasets, provides a well-scoped project that builds experience with data analysis and manuscript development. A second project initiated by the scholar allows the clinician to develop and refine their own research question, study design, and longer-term scholarly agenda.
Expected outcomes include submission of at least one manuscript to a PubMed-indexed journal with the scholar as first and corresponding author. This expectation was specified a priori in program materials. Scholars also are expected to present at the North American Primary Care Research Group (NAPCRG) conference; participation in NAPCRG was added as a program component in year 2 of the pilot. Finally, scholars are encouraged to pursue internal pilot funding.
Prospective scholars first discuss their interest with their division chief, who confirms alignment with career goals and agrees to provide 10% funded academic time and to support conference participation. The chief effectively prescreens applicants by assessing readiness for mentored research and the division’s capacity to reduce clinical effort. Applicants then partner with a research mentor to develop a two-page proposal describing planned projects and anticipated career benefits.
Prospective mentors are identified by the vice chair for research, who serves as program director, based on mentoring experience, expertise in study design and data analysis, externally funded research, and available effort. The program director reviews proposed mentor-scholar dyads, considering topical fit, complementary skills, and interpersonal compatibility.
Program funding is shared between the clinical division and a departmental research endowment. The division supports 10% of funded academic time for scholars (roughly equivalent to a half-day of clinic), and departmental funds support mentor and research staff effort, research expenses, and conference participation. Additional operational details are summarized in Tables 1 and 2.
|
Month |
Activity |
1 year program period: 0.1 FTE dedicated time; biweekly pod meetings* |
July |
Orientation |
August |
|
September |
Quarterly meeting |
October |
|
November |
|
December |
Quarterly meeting |
January |
|
February |
|
March |
Quarterly meeting |
April |
NAPCRG abstract due |
May |
|
June |
Quarterly meeting; project report due |
Outside the program period** |
July |
|
August |
|
September |
Pilot grant application option (DFMPH) |
October |
|
November |
NAPCRG presentation/participation |
December |
Pilot grant application option (School of Medicine) |
|
Funded by endowment |
Funded by division |
Total |
Personnel* |
0.1 FTE mentor |
|
0.1 FTE scholar |
|
|
0.33 FTE master-level research staff |
|
0.1 FTE scholar |
|
|
$55,300 |
|
$55,000 |
Other direct costs |
NAPCRG conference participation for two scholars ($3,000 each) |
$6,000 |
|
|
Research funds for two scholars ($5,000 each) |
$10,000 |
|
|
Publication costs for two scholars ($1,500 each) |
$3,000 |
|
|
Hospitality for quarterly program meetings |
$600 |
|
|
Total |
|
$74,900 |
|
$55,000 |
$129,900 |
OUTCOMES AND LESSONS LEARNED
Five clinician faculty completed the pilot program between 2022 and 2024 (Table 3). Outcomes included five published papers,15-19 two manuscripts under development, one internal award of $40,000, and acceptance of one clinician into an institutional research mentoring program supporting development of an NIH career development (K) proposal.20,21
Degree(s) |
Title |
Gender identity |
Years of postresidency clinical practice at program entry |
# of publications at program entry |
MD, MPH |
Assistant professor (clinical) |
Female |
3 |
9 |
MD |
Assistant professor (clinical) |
Female |
8 |
2 |
MD |
Assistant professor (clinical) |
Female |
8 |
7 |
PA-C, MMSc |
Assistant professor (clinical) |
Male |
7 |
0 |
DScPAS, MS, PA-C |
Assistant professor (clinical) |
Female |
14 |
0 |
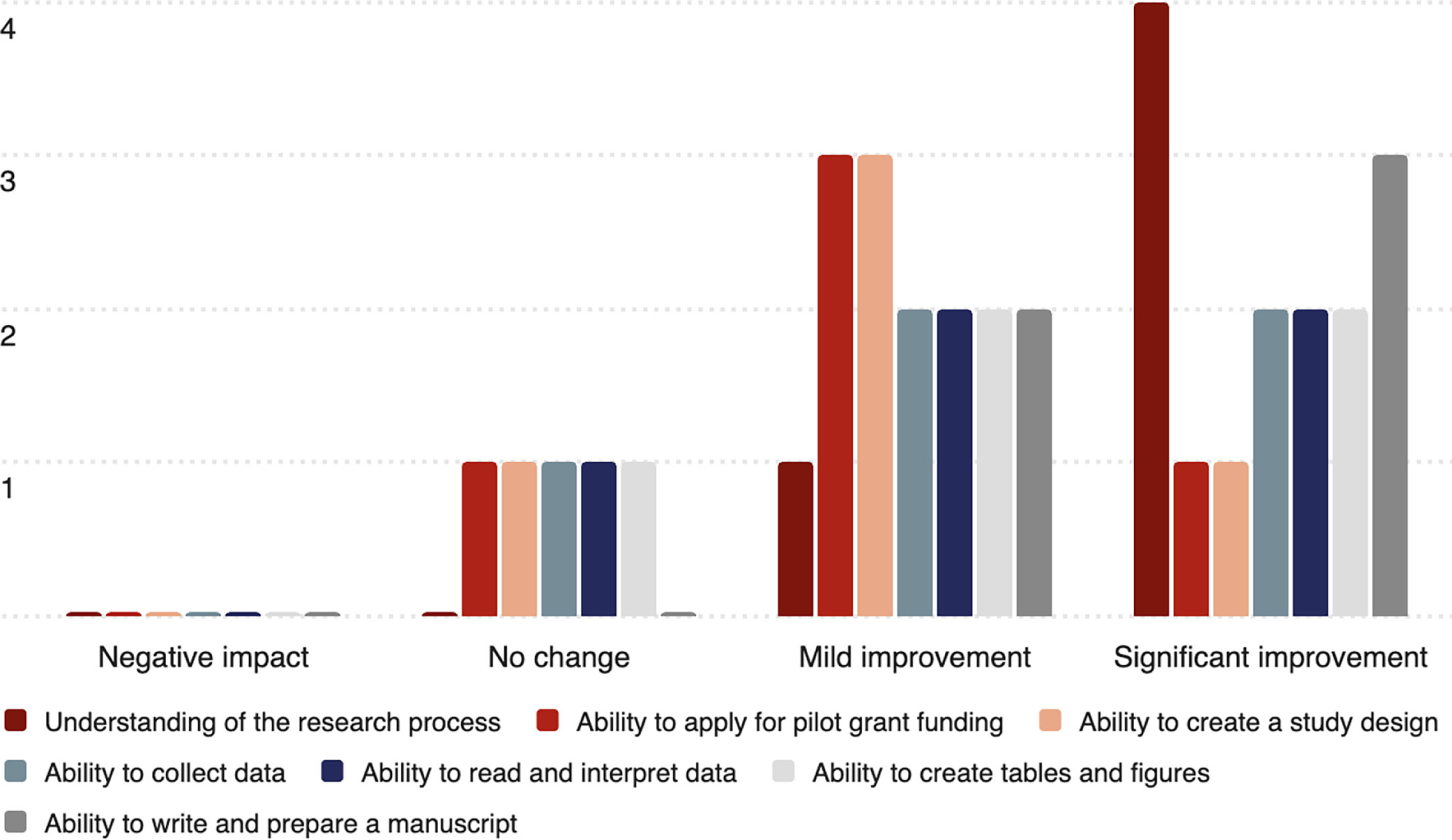
Evaluation of the pilot program was descriptive and intended to inform program refinement. At the end of year 1, scholars completed a survey with structured questions on perceived changes in research skills and open-ended questions about program experience. Survey questions were developed by program leadership based on familiarity in research mentoring and faculty development. No formal quantitative or qualitative analyses were conducted.
All scholars saw mild or significant improvement in their understanding of the research process and preparing a manuscript (Figure 1). Four scholars also reported improvements in study design, pilot grant applications, data collection and interpretation, and preparation of tables and figures. Mentors were not surveyed during the pilot program.
Based on consensus among program leadership, the following characteristics were identified as effective:
-
Requiring scholars and mentors to jointly define projects before program entry helps ensure feasibility and alignment of expectations;
-
Providing funded academic time for both scholars and mentors enables sustained engagement without reduction in salary;
-
The program benefits scholars and mentors: clinicians explore scholarly activities as part of an academic career, while researchers gain experience in mentoring clinicians
-
Access to shared research staff supports scholars with literature review, regulatory processes, data management, and statistical analysis; and
-
Program costs are shared rather than relying solely on clinical income.
Several practical observations emerged:
A minimum of 10% full-time equivalent academic time appears necessary for clinicians to meet program milestones;
Mentor-mentee compatibility requires attention from program leadership;
Clinicians with prior research exposure (eg, MPH degree) are likely to progress more quickly; and
Participation in appropriately scaled research opportunities may contribute to clinician job satisfaction.
Program capacity is limited by funding and research staff effort and currently allows one or two pods (up to four scholars) at a time. In 2024, two clinicians enrolled, although one withdrew before program start because of competing responsibilities. Department restructuring that year also contributed to a smaller second cohort.
This pilot Clinician Scholars Program suggests that modest, well-structured support—funded academic time, mentorship, and research staff assistance—can help clinician faculty engage in meaningful scholarly activity across clinical and research divisions. While none of these elements is innovative individually, their combination creates a feasible pathway for research-curious clinicians without the expectation of becoming clinician-scientists.
As a single-department pilot with a small cohort, these observations should be interpreted cautiously. Future evaluations will examine longer-term outcomes, including sustained research participation and career development among participating clinicians.
USE OF ARTIFICIAL INTELLIGENCE
During manuscript revision, the authors used ChatGPT Edu (OpenAI) to reduce the word count from 1,900 to 1,200 words. The authors reviewed, revised, and verified all content and are fully responsible for the final manuscript.
José Rodríguez is Deputy Editor of Family Medicine. The other authors declare no conflicts.
The Clinician Scholars Program in the Department of Family Medicine and Public Health (DFMPH) at the University of Utah received funds from the DFMPH Health Studies Fund, an endowment to support the advancement of research and scholarly activities in the department.
Authors M.S., E.T., B.K., K.O., and J.B.S. presented the design and implementation of the Clinician Scholars Program at the annual conferences of the North American Primary Care Research Group (poster presentation; San Francisco, CA, October 30–November 3, 2023) and the Association of Departments of Family Medicine (oral presentation; Palm Springs, CA, February 21–24, 2024).
The authors acknowledge the intellectual contributions of Drs Mia Hashibe, Jennifer P. Leiser, Leigh Elrod, Steven Lacey, and James A. VanDerslice to the design and implementation of the program and thank Tanis Garcia for financial and logistical management.
References
-
Weidner A, Peterson LE, Mainous AG III, Datta A, Ewigman B. The current state of research capacity in US family medicine departments.
Fam Med. 2019;51(2):112–119. doi:10.22454/FamMed.2019.180310
-
Indelicato AM, Weidner A, Morley CP. Family medicine: finding its way on the federal research roadmap.
J Am Board Fam Med. 2024;37(suppl 2):S85–S91. doi:10.3122/jabfm.2024.240118R1
-
Stacey SK, Seidenberg PH, Meadows LM, Schneider D, Ewigman B. Building research capacity (BRC): purposes, components, and activities to date.
J Am Board Fam Med. 2025;37(suppl 2):S96–S101. doi:10.3122/jabfm.2024.240033R1
-
Robinson SK, Meisnere M, Phillips RL Jr, McCauley L, eds. Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care.
National Academies Press. 2021. .
http://www.ncbi.nlm.nih.gov/books/NBK571810
-
Asif I, Elwood S, Weidner A. Transforming family medicine research: strategic planning, summits, and a special issue.
J Am Board Fam Med. 2025;37(suppl 2):S27–S29. doi:10.3122/jabfm.2024.240301R0
-
Piccirillo JF. The Robert Wood Johnson Clinical Scholars Program: a research training plan.
Otolaryngol Head Neck Surg. 1992;106(1):25–26. doi:10.1177/019459989210600123
-
Workman M, Albert AYK, Norman WV. Training family physicians as researchers: outcomes over 15 years for Canada’s first clinician scholar program.
Can Fam Physician. 2019;65(1):45–51. https://www.cfp.ca/content/65/1/45
-
Barreto EF, McCoy RG, Larson JJ, et al. Evaluation of the academic achievements of clinician health services research scientists involved in “pre-K” career development award programs.
J Clin Transl Sci. 2021;5(1):e122. doi:10.1017/cts.2021.780
-
Markman KM, Brewer SK, Magnuson B. Developing an engaging and accessible clinical research training program for new investigators.
J Clin Transl Sci. 2023;7(1):e53. doi:10.1017/cts.2022.446
-
Bartlett G, Carver T, Elder N, Archibald D. The grant generating project: giving primary care researchers tools to succeed.
Ann Fam Med. 2023;21(5):474–475. doi:10.1370/afm.3035
-
-
Buffington ALH, Lange C, Bakker C, et al. The collaborative scholarship intensive: a research-intensive course to improve faculty scholarship.
Fam Med. 2021;53(5):355–358. doi:10.22454/FamMed.2021.534614
-
Hersch D, Loth KA, Adam P, et al. ncreasing family medicine research capacity at the University of Minnesota: publication trends and research culture.
J Am Board Fam Med. 2024;37(6):1047–1054. doi:10.3122/jabfm.2024.240059R1
-
-
Ho TF, Zenger B, Mark B, et al. Characteristics of a transgender and gender-diverse patient population in Utah: use of electronic health records to advance clinical and health equity research.
PLoS ONE. 2024;19(5):e0302895. doi:10.1371/journal.pone.0302895
-
Spiess S, Owens R, Charron E, et al. The role of family medicine in addressing the maternal health crisis in the United States.
J Prim Care Community Health. 2024;15. doi:10.1177/21501319241274308
-
Ho TF, Fortenberry KT, Gardner E, et al. Perceived impact of virtual visits on access to care in family medicine during the COVID-19 pandemic: a qualitative study of benefits and challenges.
J Prim Care Community Health. 2023;14. doi:10.1177/21501319231220118
-
Owens RW, Dahlin M, Adediran E, et al. Pregnancy-care intentions and practice among family medicine physicians: residents, obstetric fellows, and fellowship alumni.
Fam Pract. 2025;42(5):cmaf006. doi:10.1093/fampra/cmaf006
-
Trollan A, Mark B, Spiess S, Moreno LE, Stanford J, Sleeth DK. Characteristics associated with miscarriages in Utah nail technicians.
Utah Women’s Health Rev. 2025;11. doi:10.26054/D-0KS3-WDBM
-
-
Byington CL, Keenan H, Phillips JD, et al. A matrix mentoring model that effectively supports clinical and translational scientists and increases inclusion in biomedical research: lessons from the University of Utah.
Acad Med. 2016;91(4):497–502. doi:10.1097/ACM.0000000000001021



There are no comments for this article.