Background and Objectives: Despite being critical to maternity care access, family physicians attending births continue to decrease in number. We aimed to determine the level of obstetric training at family medicine residencies and to use this variable to quantify the impact of residency training on the maternity care workforce.
Methods: We used data from the 2016 to 2023 American Board of Family Medicine National Graduate Survey and the 2018 Council of Academic Family Medicine Educational Research Alliance residency program director survey. Our exposure variable was created from a self-reported number of births attended in residency and tested using bivariate analyses with eight survey items that may indicate strong obstetric training. We then included residency obstetric training in a multilevel multiple logistic regression with attending births in practice as the outcome.
Results: Sixty percent of residencies train all the family physicians who attend births. Of the 11,728 family physicians included, the higher the obstetric training exposure for their residency, the higher the rate of attending births in practice (35.8% for average 81 + births per resident across residency vs 22.6% average 61–80 births per resident vs 10.9% average 41–60 births per resident). After adjusting for multiple other variables, graduating from a residency with higher exposure was significantly associated with attending births in practice.
Conclusions: Independent of other factors, residency obstetric training exposure has a significant impact on whether a family physician attends births in practice. Policies protecting and developing residencies with the highest exposure may improve access to safe maternity care.
Family physicians are an important part of the maternity care workforce. Unfortunately, the proportion of family physicians who attend births has decreased from 29% in 1988, to 8% in 2016, and 7.5% in 2021.1,2,3 Having family physicians who attend births is essential for access to care, particularly in rural and underserved communities.4,5 Family physicians attend births in 67% of rural hospitals and are the only clinicians attending births in 27% of rural hospitals.6 Smaller hospitals are much less likely to have obstetricians or midwives and instead rely on family physicians to provide maternity care.7 Working to support and further develop the family medicine obstetric workforce is critical to maternal health.
The decrease in the number of family physicians attending births is likely multifactorial. Factors identified in past research include increasing difficulty finding a job that allows family physicians to attend births, the lifestyle impact of attending births, and the costs and stress of malpractice insurance.8,9,10 Family physicians who are compensated for their time with laboring patients and not just using a fee for service model are more likely to stay in the family medicine obstetric workforce.11 Other family physicians would like to continue attending births, but they lose that ability through the closure of their labor and delivery units or policies forcing family physicians out of the maternity care workforce.12,13
Labor and delivery has historically been a key element of family medicine training.14 Of family medicine residency program graduates who intended to attend births in practice but do not, less than 10% of them reported lack of training as a reason.15 While family physicians generally feel well trained to provide maternity care, the strength of that training varies. Notably, being a residency with stronger maternity care training involves more than just attending many births or having many maternity focused didactic sessions. Variations exist in mentorship and in experience of the culture on labor and delivery. Some residencies have a single family medicine faculty member who attends births, and some have a full family medicine obstetric care service with multiple family medicine faculty attending births and performing cesarean deliveries. Some programs see patients on labor and delivery units where the obstetricians, midwives, and nurses are generally supportive of family medicine obstetrics and other programs do not. The recent Family Medicine Residency Outcomes Project study found that number of births attended, family medicine faculty role modeling, and increased curricular time were all associated with graduates being more likely to provide maternity care and deliver babies in practice.16 Another study identified characteristics of residencies that reported more than 25% of graduates attend births in practice: placing high importance on continuity deliveries, having family medicine faculty involved in privileging of obstetric procedures, giving a high degree of independence in obstetric management, and having family physicians supervise the majority of vaginal births.17 The added mentorship from multiple faculty members attending births and the experience of training in a culture that is more accepting of family physicians including obstetrics in their practice may contribute to more family physicians attending births after graduating residency.
The goal of this study was to determine which variables capture the strength of obstetric training in residencies and to use those data to quantify the impact of obstetric training exposure on the workforce of family physicians who attend births. If residencies with high obstetric training exposure contribute large numbers of physicians to the maternity care workforce, work supporting high exposure may be a viable way to increase the size of the workforce.
Data Sources
We used data from multiple sources. First, we used the 2016 to 2023 American Board of Family Medicine (ABFM) National Graduate Survey (NGS). The NGS is administered to early-career ABFM-certified family physicians 3 years after residency graduation and asks about practice organization, type, and location; scope of practice; loan repayment residency participation; and residency training experience and satisfaction. The respondents are representative of the eligible graduates.18 Second, we used data from a 2018 Council of Academic Family Medicine Educational Research Alliance (CERA) residency program director survey on curricula and structure that included a residency identifier.19 Third, we used Area Health Resources Files (AHRF) to obtain county level data on population demographics and health care availability. Finally, we gathered demographic and training information from ABFM administrative databases.
Study Variables
Our primary outcome was graduates currently attending births. From the NGS, we created control variables for practice site, size, and ownership. For the graduate, we used standard demographics of self-reported gender and race/ethnicity, degree type, age, and US/Canada or international training. For race/ethnicity, we created a variable indicating whether the family physician belonged to a group that is historically underrepresented in medicine.20
We geocoded the practice address and, from that, assigned county-level rurality using the Rural-Urban Continuum Codes, county-level Health Professional Shortage Area, and Census Region. From the AHRF, we created an indicator for the county having a hospital with an obstetric unit. To model demand for obstetric services, we calculated the percentage of the population in the county that are reproductive age (15–49 years) females. To model obstetric workforce competition, we created a variable for the number of certified nurse midwives and obstetrics and gynecology (OB/GYN) physicians per 10,000 reproductive age females in the county.
Our main exposure variable of residency obstetric training was created from a self-reported number of births attended in residency from the 2016 to 2023 NGS. The data are categorical with<20, 21–40, 41–60, 61–80, 81–100, and 100 + as options. Due to the small sample size in the 100 + category, we merged 81–100 and 100 + into an 81 + category. We then created a unique weighted average by treating each training exposure category as an ordinal value between 1 and 5 then rounded to the lower whole number, also called flooring, and translated back to the reflected categorical representation. For example, if one graduate was 21–40, one was 41–60, and four were 61–80, then the weighted average would be 3.5 and thus would fall in the 41–60 exposure category as a residency. The final categories 1 through five were (1) “lowest exposure” with the weighted average of<20 births, (2) “low exposure” with 21–40 births, (3) “moderate exposure” with 41–60 births, (4) “high exposure” with 61–80 births, and (5) “highest exposure” with 81 + births. We determined the exposure category for each residency and used it as the exposure variable.
Data Analysis
To test our obstetric training exposure variable, we performed bivariate analyses with eight items reported by residency directors in the CERA survey that may indicate strong obstetric training. These eight items included the presence of an advanced maternity care track, whether the residency requires continuity deliveries, the number of months required in maternity care, the number of family physician faculty who supervise deliveries, whether residency faculty supervise cesarean births, the presence or absence of OB/GYN residents where family medicine residents receive maternity care training, and the presence of OB/GYN residents where family medicine residents receive intrapartum training (Appendix A).
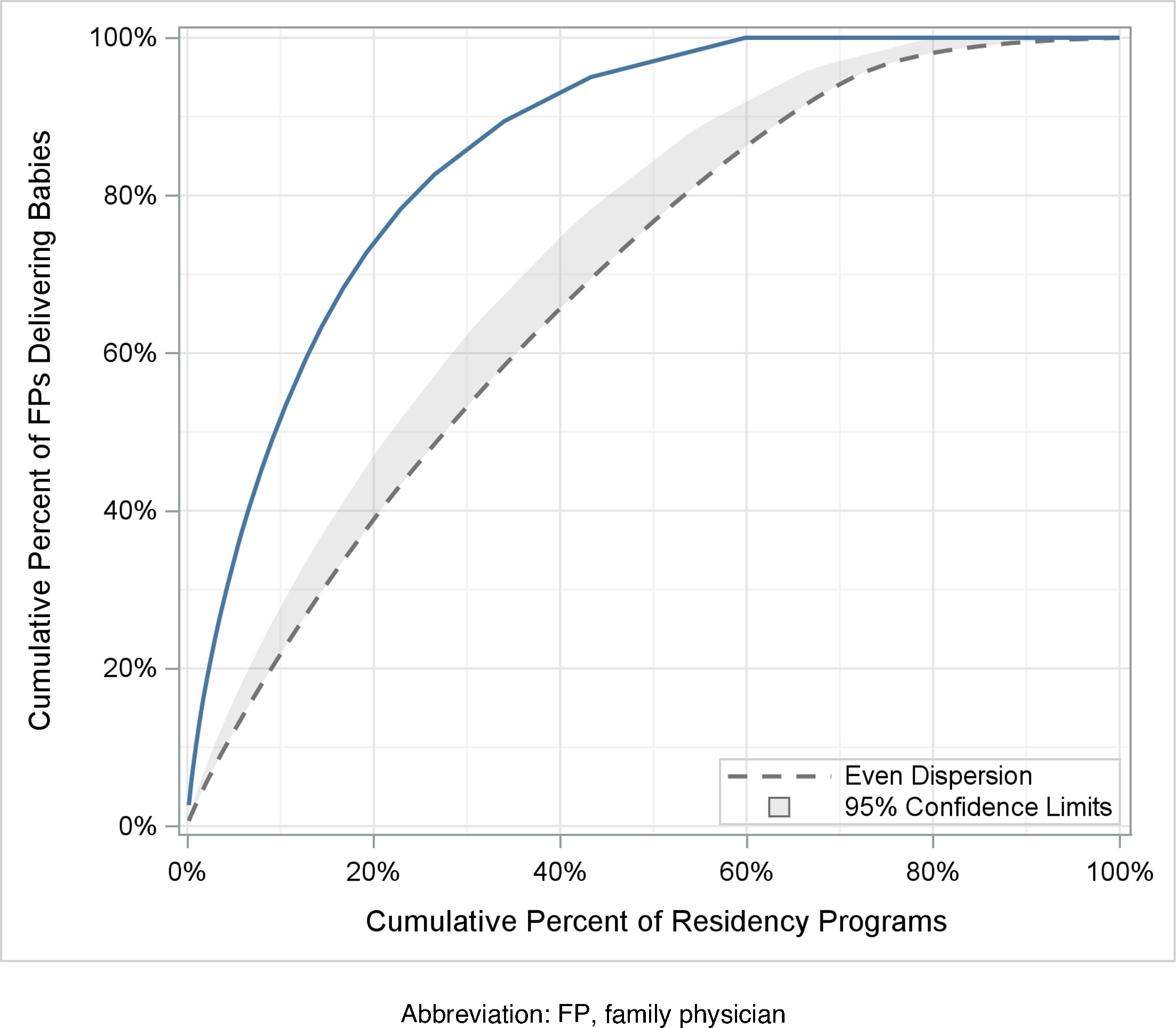
After determining the exposure variable was reliable, we proceeded with the rest of the data analysis. First, we described our data. Second, we determined the residency level distribution of graduates performing obstetrics by plotting the cumulative percentage of graduates by residency. Third, we assessed the stability of the obstetric training exposure variable over time by breaking up the data into 3 year rolling averages and looking for change. We also performed a linear regression to assess global stability. Fourth, we performed bivariate analyses of demographics, attending births, practice features, and county characteristics by obstetric training. Fifth, we conducted additional bivariate testing for the same variables as well as for the obstetric training exposure variable by whether the family physician attended births. Bivariate testing was by χ2, t test, or analysis of variance, and P values were adjusted for multiple comparison using the false discovery rate. Finally, we conducted a multilevel multiple logistic regression with attending births as the outcome. The exposure variable was the main effect. We adjusted for clustering by residency and included covariates. We mapped the state level distribution of residency obstetric training exposure. SAS version 9.4 (SAS Institute) was used for all analyses. This study was approved by the American Academy of Family Physicians Institutional Review Board (#22–448).
Sixty percent of all 533 residencies in our sample trained 100% of the family physicians who attended births. In other words, 40% of residencies in our sample have not produced a single family physician who attends births since 2016 (Figure 1). Our obstetric training exposure variable was significantly and positively associated with residency program director reported measures of obstetric training, including the number of family medicine faculty attending births and performing cesarean births, the number of months of obstetric care required during residency, and the requirement of continuity deliveries (Appendix A). Testing the stability of the exposure variable over time, 19 of 487 residencies with multiple years of data changed obstetric training exposure over time. Many of these were newer residencies with fewer years of data. Given that 96.1% of residencies remained in the same exposure variable category over time, we determined that this exposure variable is stable and proceeded with the analysis plan.
Of the 11,728 family physicians included in this study, 1,300 (11.1%) graduated from residencies with the highest exposure (81 + births). Those who graduated from residencies with the highest exposure had the highest rates of attending births in practice (35.8%, P<0.001; Table 1). They also tended to be younger and more likely to be participating in a loan repayment, specifically in the military (10.7% from the highest obstetric training exposure vs 1.6% from the lowest exposure) or National Health Service Corps (7.9% vs 4.0%). Those who graduated from residencies with lower levels of obstetric training exposure were more likely to be international medical graduates or from a group historically underrepresented in medicine.
|
Categorical proportion of births attended by program |
|
|
Lowest
<20 births
N = 577
n (%) |
Low
21–40 births
N = 3624
n (%) |
Moderate
41–60 births
N = 3890
n (%) |
High
61–80 births
N = 2337
n (%) |
Highest
81 + births
N = 1300
n (%) |
Total
N = 11,728
n (%) |
P values |
Attends births as part of practice |
|
11 (1.9) |
136 (3.8) |
423 (10.9) |
529 (22.6) |
465 (35.8) |
1,564 (13.3) |
<0.0001 |
Individual and practice characteristics |
|
|
|
|
|
|
|
|
Age by category |
<38 |
459 (79.5) |
2,799 (77.2) |
3,154 (81.1) |
1,938 (82.9) |
1,125 (86.5) |
9,475 (80.8) |
<0.0001 |
≥38 |
118 (20.5) |
825 (22.8) |
736 (18.9) |
399 (17.1) |
175 (13.5) |
2,253 (19.2) |
|
Gender |
Female |
303 (52.5) |
2,028 (56.0) |
2,153 (55.3) |
1,318 (56.4) |
693 (53.3) |
6,495 (55.4) |
.0101 |
Male |
271 (47.0) |
1,587 (43.8) |
1,719 (44.2) |
1,004 (43.0) |
598 (46.0) |
5,179 (44.2) |
|
Nonbinary |
|
2 (0.1) |
3 (0.1) |
6 (0.3) |
3 (0.2) |
14 (0.1) |
|
Prefer not to answer |
3 (0.5) |
7 (0.2) |
15 (0.4) |
9 (0.4) |
4 (0.3) |
38 (0.3) |
|
Prefer to self-describe |
|
|
|
|
2 (0.2) |
2 (0.0) |
|
Degree type |
MD (vs DO) |
346 (60.0) |
3,094 (85.4) |
3,096 (79.6) |
1,817 (77.7) |
1,040 (80.0) |
9,393 (80.1) |
<0.0001 |
Underrepresented in medicine |
|
70 (12.3) |
729 (20.4) |
531 (13.9) |
288 (12.4) |
95 (7.4) |
1,713 (14.8) |
<0.0001 |
International medical graduate (US/CAN) |
|
175 (30.3) |
1,599 (44.1) |
1,296 (33.3) |
470 (20.1) |
87 (6.7) |
3,627 (30.9) |
<0.0001 |
Participation in a loan repayment residency |
Military |
9 (1.6) |
51 (1.4) |
125 (3.2) |
191 (8.2) |
139 (10.7) |
515 (4.4) |
<0.0001 |
NHSC |
23 (4.0) |
130 (3.6) |
194 (5.0) |
162 (6.9) |
103 (7.9) |
612 (5.2) |
|
None |
307 (53.2) |
2,231 (61.6) |
2,070 (53.2) |
1,083 (46.3) |
505 (38.8) |
6,196 (52.8) |
|
Other |
238 (41.2) |
1,212 (33.4) |
1,501 (38.6) |
901 (38.6) |
553 (42.5) |
4,405 (37.6) |
|
Principal practice site |
Academic health center/faculty practice |
60 (12.7) |
400 (13.6) |
414 (12.9) |
239 (11.8) |
132 (11.1) |
1,245 (12.7) |
<0.0001 |
Federally qualified health center or look-alike |
43 (9.1) |
317 (10.8) |
315 (9.8) |
251 (12.4) |
148 (12.4) |
1,074 (10.9) |
|
Hospital/health system owned medical practice |
212 (44.9) |
1,298 (44.2) |
1,405 (43.9) |
878 (43.3) |
454 (38.1) |
4,247 (43.2) |
|
Independently owned medical practice |
94 (19.9) |
436 (14.8) |
479 (15.0) |
211 (10.4) |
134 (11.3) |
1,354 (13.8) |
|
Managed care/HMO practice |
12 (2.5) |
173 (5.9) |
146 (4.6) |
74 (3.6) |
25 (2.1) |
430 (4.4) |
|
Other |
28 (5.9) |
210 (7.1) |
282 (8.8) |
257 (12.7) |
188 (15.8) |
965 (9.8) |
|
Rural health clinic (federally qualified) |
23 (4.9) |
105 (3.6) |
160 (5.0) |
118 (5.8) |
110 (9.2) |
516 (5.2) |
|
Principal practice ownership |
No ownership (vs partial or full) |
323 (85.4) |
2,081 (90.2) |
2,173 (88.9) |
1,262 (90.0) |
652 (87.5) |
6,491 (89.2) |
.0247 |
Principal practice size |
Solo practice |
19 (4.0) |
113 (3.8) |
107 (3.3) |
53 (2.6) |
21 (1.8) |
313 (3.2) |
<0.0001 |
|
2–5 clinicians |
196 (41.5) |
1,169 (39.8) |
1,201 (37.5) |
677 (33.4) |
374 (31.4) |
3,617 (36.8) |
|
6–20 clinicians |
171 (36.2) |
1,057 (36.0) |
1,217 (38.0) |
877 (43.2) |
542 (45.5) |
3,864 (39.3) |
|
>20 clinicians |
86 (18.2) |
600 (20.4) |
676 (21.1) |
421 (20.8) |
254 (21.3) |
2,037 (20.7) |
|
Area level variables |
|
|
|
|
|
|
|
|
Rurality (RUCC) |
Nonmetropolitan (vs metropolitan) |
100 (17.3) |
382 (10.5) |
659 (16.9) |
478 (20.5) |
376 (28.9) |
1,995 (17.0) |
<0.0001 |
Census region |
Northeast |
114 (19.8) |
768 (21.2) |
649 (16.7) |
310 (13.3) |
60 (4.6) |
1,901 (16.2) |
<0.0001 |
Midwest |
90 (15.6) |
838 (23.1) |
1,239 (31.9) |
776 (33.2) |
577 (44.4) |
3,520 (30.0) |
|
South |
328 (56.9) |
1,819 (50.2) |
1,495 (38.5) |
700 (30.0) |
319 (24.5) |
4,661 (39.8) |
|
West |
44 (7.6) |
199 (5.5) |
505 (13.0) |
550 (23.5) |
344 (26.5) |
1,642 (14.0) |
|
Presence of a hospital with OB services in the county in which they live |
|
470 (81.5) |
3,182 (87.8) |
3,343 (85.9) |
1,968 (84.2) |
1,105 (85.0) |
10,068 (85.8) |
<0.0001 |
Practicing in an HPSA |
|
519 (89.9) |
3,344 (92.3) |
3,576 (91.9) |
2,143 (91.7) |
1,170 (90.0) |
10,752 (91.7) |
0.0594 |
Social deprivation index |
Under 25 |
120 (20.8) |
859 (23.7) |
1,124 (28.9) |
600 (25.7) |
465 (35.8) |
3,168 (27.0) |
<0.0001 |
25–75 |
329 (57.0) |
1,844 (50.9) |
1,914 (49.2) |
1,372 (58.7) |
710 (54.6) |
6,169 (52.6) |
|
Over 75 |
128 (22.2) |
921 (25.4) |
852 (21.9) |
365 (15.6) |
125 (9.6) |
2,391 (20.4) |
|
Reproductive age female population |
Under 18 |
145 (25.1) |
746 (20.6) |
849 (21.8) |
576 (24.6) |
360 (27.7) |
2,676 (22.8) |
<0.0001 |
18–21 |
292 (50.6) |
1,740 (48.0) |
1,887 (48.5) |
1,097 (46.9) |
569 (43.8) |
5,585 (47.6) |
|
Over 21 |
140 (24.3) |
1,138 (31.4) |
1,154 (29.7) |
664 (28.4) |
371 (28.5) |
3,467 (29.6) |
|
Presence of nurse midwives per 10,000 female reproductive age population |
None |
113 (19.6) |
341 (9.4) |
558 (14.3) |
374 (16.0) |
283 (21.8) |
1,669 (14.2) |
<0.0001 |
One or fewer |
204 (35.4) |
1,244 (34.3) |
1,206 (31.0) |
586 (25.1) |
349 (26.8) |
3,589 (30.6) |
|
Greater than 1 |
260 (45.1) |
2,039 (56.3) |
2,126 (54.7) |
1,377 (58.9) |
668 (51.4) |
6,470 (55.2) |
|
Presence of OB/GYNs per 10,000 female reproductive age population in the county |
None |
49 (8.5) |
155 (4.3) |
284 (7.3) |
205 (8.8) |
206 (15.8) |
899 (7.7) |
<0.0001 |
Five or fewer |
182 (31.5) |
1,074 (29.6) |
1,207 (31.0) |
734 (31.4) |
468 (36.0) |
3,665 (31.3) |
|
Greater than 5 |
346 (60.0) |
2,395 (66.1) |
2,399 (61.7) |
1,398 (59.8) |
626 (48.2) |
7,164 (61.1) |
|
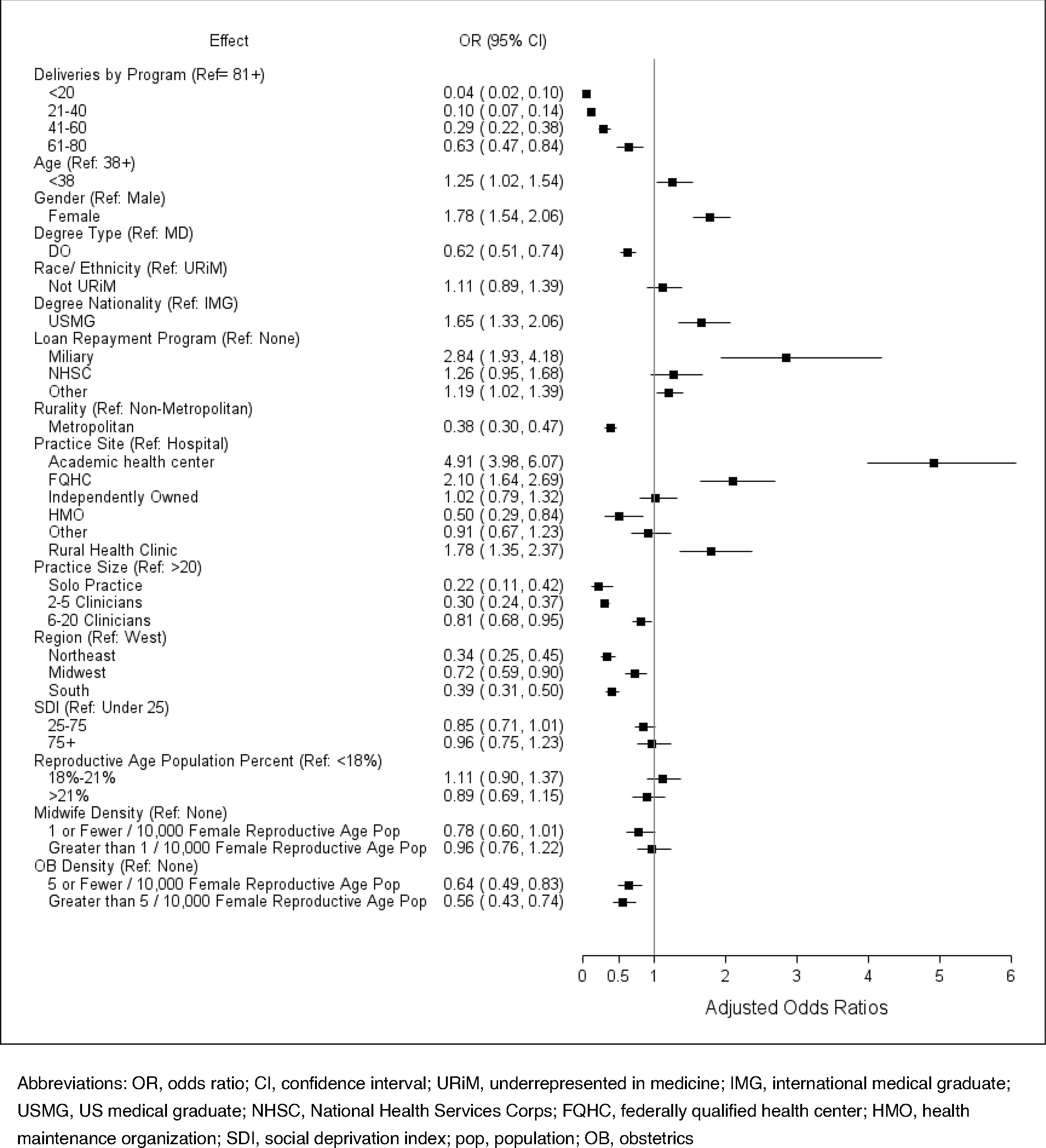
Family physicians who graduated from residencies with high or the highest obstetric training exposure are significantly overrepresented in the population of family physicians attending births, making up only 31% of the study population but 63.5% of those attending births (Table 2). This finding is also seen in the adjusted model with those graduating from residencies with the highest exposure being significantly more likely to attend births than all other groups (Figure 2).
|
Do not attend births
N = 10,164
n (%) |
Attend births
N = 1564
n (%) |
Total
N = 11,728
n (%) |
Categorical proportion of births by programa |
<20 |
566 (5.6) |
11 (0.7) |
577 (4.9) |
21–40 |
3,488 (34.3) |
136 (8.7) |
3,624 (30.9) |
41–60 |
3,467 (34.1) |
423 (27.0) |
3,890 (33.2) |
61–80 |
1,808 (17.8) |
529 (33.8) |
2,337 (19.9) |
81+ |
835 (8.2) |
465 (29.7) |
1,300 (11.1) |
Individual and practice characteristics |
|
|
|
|
Agea |
<38 |
8,127 (80.0) |
1,348 (86.2) |
9,475 (80.8) |
≥38 |
2,037 (20.0) |
216 (13.8) |
2,253 (19.2) |
Gendera |
Female |
5,480 (53.9) |
1,015 (64.9) |
6,495 (55.4) |
Male |
4,638 (45.6) |
541 (34.6) |
5,179 (44.2) |
Nonbinary |
12 (0.1) |
2 (0.1) |
14 (0.1) |
Prefer not to answer |
33 (0.3) |
5 (0.3) |
38 (0.3) |
Prefer to self-describe |
1 (0.0) |
1 (0.1) |
2 (0.0) |
Degree typea |
DO |
2,063 (20.3) |
272 (17.4) |
2,335 (19.9) |
MD |
8,101 (79.7) |
1,292 (82.6) |
9,393 (80.1) |
Underrepresented in medicinea |
|
1,567 (15.6) |
146 (9.5) |
1,713 (14.8) |
International medical graduate (US/CAN)a |
|
3,435 (33.8) |
192 (12.3) |
3,627 (30.9) |
Participating in a loan repayment residencya |
Military |
388 (3.8) |
127 (8.1) |
515 (4.4) |
NHSC |
445 (4.4) |
167 (10.7) |
612 (5.2) |
None |
5,631 (55.4) |
565 (36.1) |
6,196 (52.8) |
Other |
3,700 (36.4) |
705 (45.1) |
4,405 (37.6) |
Principal practice sitea |
Academic health center/faculty practice |
883 (10.6) |
362 (24.4) |
1,245 (12.7) |
Federally qualified health center or Look-Alike |
836 (10.0) |
238 (16.1) |
1,074 (10.9) |
Hospital/health system owned medical practice |
3,822 (45.8) |
425 (28.7) |
4,247 (43.2) |
Independently owned medical practice |
1,235 (14.8) |
119 (8.0) |
1,354 (13.8) |
Managed care/HMO practice |
410 (4.9) |
20 (1.4) |
430 (4.4) |
Other |
821 (9.8) |
144 (9.7) |
965 (9.8) |
Rural health clinic (federally qualified) |
343 (4.1) |
173 (11.7) |
516 (5.2) |
Principal practice ownership |
No ownership |
5,658 (89.1) |
833 (90.0) |
6,491 (89.2) |
Ownership |
692 (10.9) |
93 (10.0) |
785 (10.8) |
Principal practice sizea |
2–5 clinicians |
3,347 (40.1) |
270 (18.2) |
3,617 (36.8) |
6–20 clinicians |
3,103 (37.2) |
761 (51.4) |
3,864 (39.3) |
>20 clinicians |
1,600 (19.2) |
437 (29.5) |
2,037 (20.7) |
Solo practice |
300 (3.6) |
13 (0.9) |
313 (3.2) |
Area level variables |
|
|
|
|
Rurality (RUCC)a |
Metropolitan |
8,708 (85.7) |
1,025 (65.5) |
9,733 (83.0) |
Nonmetropolitan |
1,456 (14.3) |
539 (34.5) |
1,995 (17.0) |
OB hospital |
|
8,736 (86.0) |
1,332 (85.2) |
10,068 (85.8) |
HPSA |
|
9,315 (91.6) |
1,437 (91.9) |
10,752 (91.7) |
Census regiona |
Northeast |
1,752 (17.2) |
149 (9.5) |
1,901 (16.2) |
Midwest |
2,877 (28.3) |
643 (41.2) |
3,520 (30.0) |
South |
4,321 (42.5) |
340 (21.8) |
4,661 (39.8) |
West |
1,212 (11.9) |
430 (27.5) |
1,642 (14.0) |
Social deprivation indexa |
Under 25 |
2,676 (26.3) |
492 (31.5) |
3,168 (27.0) |
25–75 |
5,353 (52.7) |
816 (52.2) |
6,169 (52.6) |
Over 75 |
2,135 (21.0) |
256 (16.4) |
2,391 (20.4) |
Percent female reproductive age populationa |
Under 18 |
2,191 (21.6) |
485 (31.0) |
2,676 (22.8) |
18–21 |
4,915 (48.4) |
670 (42.8) |
5,585 (47.6) |
Over 21 |
3,058 (30.1) |
409 (26.2) |
3,467 (29.6) |
Rate midwives per 10,000 female reproductive age populationa |
None |
1,319 (13.0) |
350 (22.4) |
1,669 (14.2) |
One or fewer |
3,274 (32.2) |
315 (20.1) |
3,589 (30.6) |
Greater than 1 |
5,571 (54.8) |
899 (57.5) |
6,470 (55.2) |
Rate OB per 10,000 female reproductive age populationa |
None |
623 (6.1) |
276 (17.6) |
899 (7.7) |
Five or fewer |
3,178 (31.3) |
487 (31.1) |
3,665 (31.3) |
Greater than 5 |
6,363 (62.6) |
801 (51.2) |
7,164 (61.1) |
In adjusted regression models, we found that younger age (aOR = 1.254, CI [1.022, 1.538]), female gender (aOR = 1.780, CI [1.542, 2.055]), and working in an academic health center or faculty practice (aOR = 4.912, CI [3.975, 6.070]) were associated with increased odds of attending births. Participation in military loan repayment also was associated with higher odds of attending births (aOR = 2.841, CI [1.932, 1.384]), while National Health Service Corps participation was not associated with attending births (Figure 2). The presence of nurse midwives in the county was not associated with attending births, but family physicians practicing in a county with greater than five OB/GYNs per 10,000 females of reproductive age had lower odds of attending births (aOR = 0.561, CI [0.425, 0.740]; Figure 2).
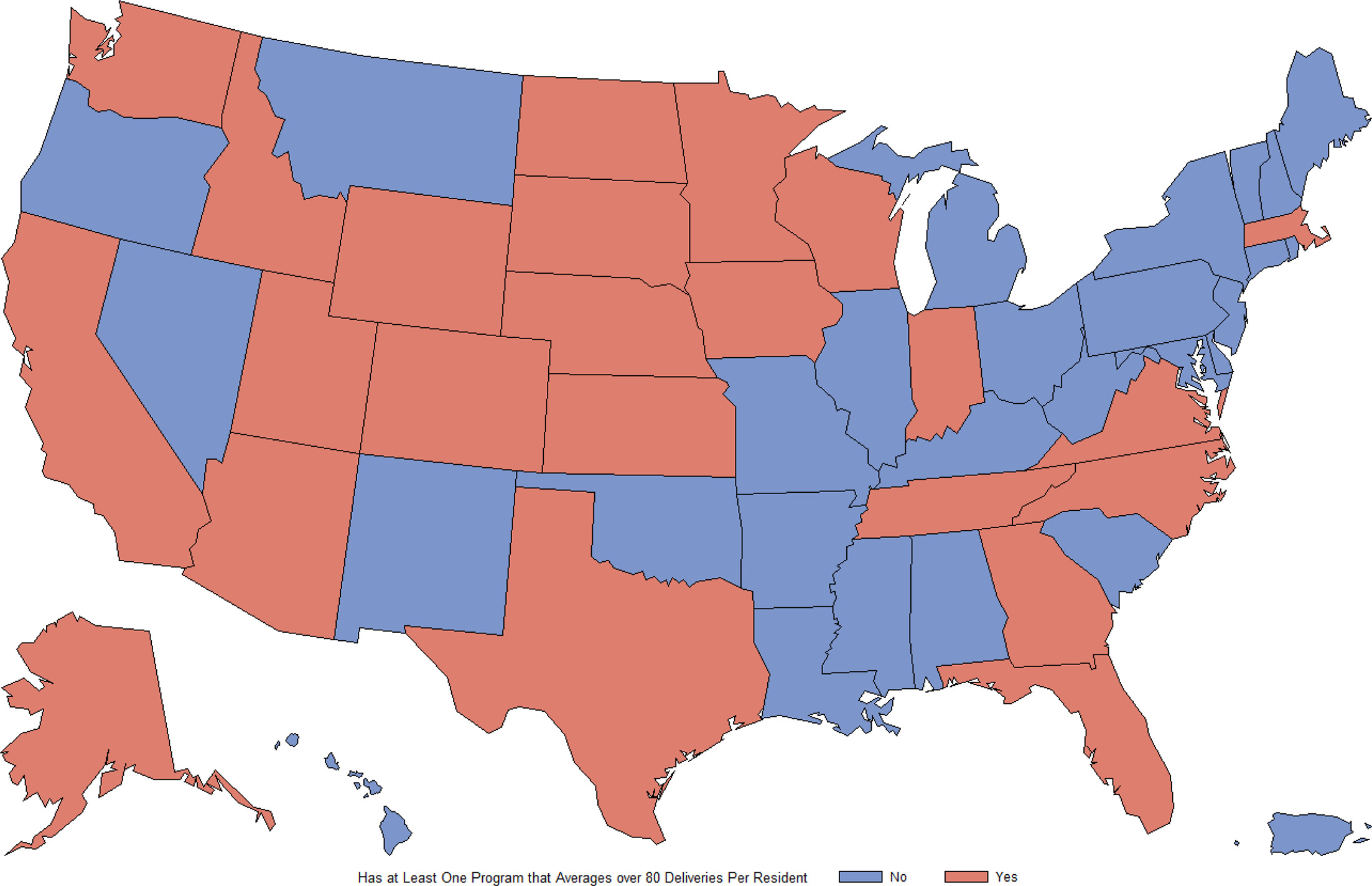
High obstetric training exposure is concentrated in the Midwest and West Census Regions. Eight of the 12 states in the Midwest (66.7%) and eight of the 13 states in the West (61.5%) have at least one residency with the highest obstetric training exposure. Whereas only one of the nine states in the Northeast (11.1%) and six of 16 states in the South (37.5%) have a single residency in the highest exposure (Figure 3).
Using data from multiple sources, we determined that a categorical variable of the average number of births attended by graduates during residency is an adequate surrogate for obstetric training exposure because it correlated with multiple markers of obstetric training quality. Obstetric training exposure is a significant independent predictor of whether a family physician attends births in practice. Policies supporting the continuation and development of high obstetric training exposure may be one strategy to strengthen the maternity care workforce.
While residencies with moderate and high obstetric training exposure contribute a lower percentage of their residents to the maternity care workforce, there is a larger absolute number of residents from these programs. We identified 3,890 residents from programs with moderate training exposure, 2,337 from programs with high exposure, and 1,300 residents from highest exposure programs. Developing the culture of moderate and high obstetric training exposure residencies with the goal of shifting toward the highest exposure category could make a large impact on the maternity care workforce. For example, many more graduates come from residencies with a moderate obstetric training exposure (N = 3,890) than the highest exposure (N = 1,300). If current residencies with moderate exposure were adding to the workforce at the same rate as residencies with high obstetric training exposure (22.6%), that would be an additional 457 family physicians attending births added to the workforce from just the graduates in this sample. For new programs that are developing or programs that currently have low obstetric training exposure, this study supports the importance of increasing obstetric training exposure to the highest level possible for the training environment and creating a program-wide culture that supports providing maternity care.
In 2023, the Accreditation Council for Graduate Medical Education (ACGME) implemented revised residency requirements that put back a minimum delivery number requirement for all residents of 20 vaginal births and introduced for the first time new requirements for residents who want to obtain competency in intrapartum management for independent practice in a labor and delivery setting.21 This new requirement for those residents raised the minimum requirement of births attended to 80 and at least 4 months of focused curricular experience, along with requiring those programs to have at least one supervising family physician attending births. The requirement for all residents reflects our lowest obstetric training exposure programs, but the intrapartum management requirement reflects our highest obstetric training exposure programs (if the majority of residents obtain this level of training). Programs with moderate or high obstetric training exposure are likely providing this option for their residents as well. Supporting more programs to be able to provide this level of training is important to grow and strengthen the maternity care workforce.
Only one state in the Northeast had a single residency with the highest obstetric training exposure, and family physicians are less likely to attend births in the Northeast. The Northeast region of the United States also has the highest rate of severe maternal morbidity at 173 per 10,000 births.22 We wonder whether a regional culture that supports high obstetric training exposure might also support lower maternal morbidity. Previous studies have shown that labor and delivery units staffed exclusively by family physicians have stronger nursing rated safety cultures and lower cesarean birth rates.23 Also important to note is that family physicians provide care to patients with increased social risk factors without compromise to care.24 Whether the presence of more residencies with higher obstetric training exposure could impact maternal outcomes is not known. Perhaps family physicians with a focus on relationship-based care and the ability to care for socially and medically complex patients would be an asset to maternity care in a region of the country with high maternal morbidity and mortality. Whatever the reason for the association, increasing the number of family medicine residencies in the Northeast that offer higher levels of obstetric training exposure might improve maternity care outcomes. Current residencies in the Northeast with moderate or high obstetric training exposure should be supported to develop the culture and resources needed to have the highest exposure to promote more programs of excellence in this region.
Unfortunately, threats to residencies with high obstetric training exposure have been increasing over the last several years. Many residencies with high exposure are located in urban areas that serve vulnerable populations. These residencies and the associated family physicians provide maternity care services to medically underserved populations in institutions with large OB/GYN groups as well. Often when leadership in hospitals or OB/GYN groups changes, these institutions question the value of having family physicians attend births and, in some extreme cases, will change hospital policies to exclude them.13 The harms of these threats and in some cases closures of these residencies is not only the direct loss of care to the communities these programs serve but also may decrease the number of family physicians attending births as part of their practice after graduating residency. This study showed that residencies with high obstetric training exposure graduate a disproportionate share of family physicians who attend births in practice, so the loss of these programs has a disproportionately high negative impact on the future US maternity care workforce.
We found that the higher level of obstetric training exposure a residency had, the greater proportion of graduate attending births in practice. In addition to strategically increasing exposure at residencies, other modifiable factors associated with higher rates of family physicians attending births to improve the maternity care workforce are worth identifying. We found that loan repayment is significantly associated with a positive likelihood of attending births in practice. Loan repayment programs are of many different types and structures, and a full assessment of all types and combinations of loan repayment was outside the scope of this study. Future studies should explore specific structures of loan repayment and whether loan repayment could be leveraged to improve the maternity care workforce. Smaller practice size was associated with lower likelihood of attending births. This association is consistent with previous studies that found a lack of methods for call sharing to be a barrier to new family physicians attending births as part of their practice.9 Identifying and removing barriers to call sharing, not only among family physicians but also among other maternity care clinicians (eg, OB/GYNs and nurse midwives), might be a way to modify and improve the maternity care workforce. Residencies might explicitly teach strategies to establish call sharing in future practice.
One strategy some programs have used to strengthen obstetric training exposure is to offer an obstetric track where residents self-select as interested in obstetrics and complete additional training. This study did not specifically assess obstetric tracks. Prior work has found that programs that self-determined not to need an obstetric track due to strength of obstetric training reported a higher proportion of graduates attending births (21%) than programs with an obstetric track.25 A recent study found that supporting residencies that create a culture where most of the residents are obtaining a high volume of training is important.16
Our study is subject to multiple limitations. First, our main exposure variable was based on resident self-report and is subject to potential bias. With broad categories of numbers of births and motivated family physicians needing to report how many births they attended in residency for credentialing, we believe this is less of an issue. Second, our data were cross-sectional, and we cannot make causal inferences. Third, we lacked robust data on whether graduates completed a maternity care fellowship, which would influence whether the graduate attends births in practice. Finally, these data reflect the training completed by residents prior to the implementation of the new ACGME requirements and do not speak to the impact of those requirements.
In this study we found that in the last 10 years, only 60% of residencies have trained all the family physicians who attend births. Further we found that the average number of births attended across all graduates in a residency is a valid and reliable measure of the level of obstetric training exposure for a residency. Further studies could identify concrete strategies to improve obstetric training exposure. Policies to improve the maternity care workforce should focus on strategies to protect current residencies with high obstetric training exposure and to support other residencies to develop the culture, clinical experiences, and curricular structures needed for high exposure. Protecting and developing high obstetric training exposure for family medicine residents may improve access to safe maternity care.
References
-
Kahn NB Jr, Schmittling G. Obstetric privileges for family physicians: a national study.
J Am Board Fam Pract. 1995;8(2):120–127. doi:10.3122/jabfm.8.2.120
-
-
Walter G, Jetty A, Topmiller M, Huffstetler A. Family physicians provide maternity care in and around the maternity care shortage areas, particularly rural.
J Rural Health. 2024;40(4):664–670. doi:10.1111/jrh.12848
-
-
Barreto T, Jetty A, Eden AR, Petterson S, Bazemore A, Peterson LE. Distribution of Physician Specialties by Rurality.
J Rural Health. 2021;37(4):714–722. doi:10.1111/jrh.12548
-
Deutchman M, Macaluso F, Bray E, et al. The impact of family physicians in rural maternity care.
Birth. 2022;49(2):220–232. doi:10.1111/birt.12591
-
Kozhimannil KB, Casey MM, Hung P, Han X, Prasad S, Moscovice IS. The rural obstetric workforce in US hospitals: challenges and opportunities.
J Rural Health. 2015;31(4):365–372. doi:10.1111/jrh.12112
-
Tong ST, Makaroff LA, Xierali IM, Puffer JC, Newton WP, Bazemore AW. Family physicians in the maternity care workforce: factors influencing declining trends.
Matern Child Health J. 2013;17(9):1576–1581. doi:10.1007/s10995-012-1159-8
-
Eden AR, Barreto T, Hansen ER. Experiences of new family physicians finding jobs with obstetrical care in the USA.
Fam Med Community Health. 2019;7(3). doi:10.1136/fmch-2018-000063
-
Barreto TW, Eden A, Hansen ER, Peterson LE. Opportunities and barriers for family physician contribution to the maternity care workforce.
Fam Med. 2019;51(5):383–388. doi:10.22454/FamMed.2019.845581
-
Barreto TW, Taylor MK, Goldstein JT, Eden AR. Retaining the perinatal care workforce: lessons learned from experienced physicians who no longer attend deliveries.
Health Serv Res. 2024;59(1). doi:10.1111/1475-6773.14224
-
Hung P, Kozhimannil KB, Casey MM, Moscovice IS. Why are obstetric units in rural hospitals closing their doors?
Health Serv Res. 2016;51(4):1546–1560. doi:10.1111/1475-6773.12441
-
-
Peterson LE, Fang B, Puffer JC, Bazemore AW. Wide gap between preparation and scope of practice of early career family physicians.
J Am Board Fam Med. 2018;31(2):181–182. doi:10.3122/jabfm.2018.02.170359
-
Barreto TW, Eden AR, Hansen ER, Peterson LE. Barriers faced by family medicine graduates interested in performing obstetric deliveries.
J Am Board Fam Med. 2018;31(3):332–333. doi:10.3122/jabfm.2018.03.170427
-
Rosener SE, Peterson LE, Fleischer S, Barr WB. Residency characteristics associated with pregnancy care among graduates: a family medicine residency outcomes project study.
Fam Med. 2025;57(10):704–713. doi:10.22454/FamMed.2025.945690
-
-
Peterson LE. Using the family medicine national graduate survey to improve residency education by monitoring training outcomes.
Fam Med. 2021;53(7):622–625. doi:10.22454/FamMed.2021.719992
-
Barr WB, Peterson LE, Fleischer S, Seehusen DA. National family medicine residency outcomes project methodology.
PRiMER. 2024;8. doi:10.22454/PRiMER.2024.588860
-
-
-
Declercq E, Zephyrin LC. Severe maternal morbidity in the United States. a primer.
The Commonwealth Fund. 2021. doi:10.26099/r43h-vh76
-
VanGompel EW, Singh L, Carlock F, Rittenhouse C, Ryckman KK, Radke S. Family medicine presence on labor and delivery: effect on safety culture and cesarean delivery.
Ann Fam Med. 2024;22(5):375–382. doi:10.1370/afm.3157
-
Partin M, Sanchez A, Poulson J, Berg A, Parascando J, Ramirez SI. Social inequities between prenatal patients in family medicine and obstetrics and gynecology with similar outcomes.
J Am Board Fam Med. 2021;34(1):181–188. doi:10.3122/jabfm.2021.01.200279
-
Roskos SE, Barreto TW, Phillips JP, King VJ, Eidson-Ton WS, Eden AR. Maternity care tracks at US family medicine residency programs.
Fam Med. 2021;53(10):857–863. doi:10.22454/FamMed.2021.237852



There are no comments for this article.