Background and Objectives: The Primary Care Exception (PCE) in US graduate medical education allows billing for low complexity outpatient primary care visits with indirect faculty supervision, where the faculty does not directly see the patient. The PCE historically applied only to lower complexity billing codes; but during the COVID-19 public health emergency (PHE) from March 2020 to May 2023, the PCE was expanded to include moderate and high complexity visits. Prior PCE studies have evaluated family medicine residencies before the 2021 update to the Evaluation and Management Services guidelines, which include different definitions of complexity. This is the first study to evaluate the billing impact of PCE in a primary care residency of internal medicine after the Evaluation and Management Services update.
Methods: We conducted a retrospective billing data evaluation of 99213, 99214, and 99215 billing codes from July to September 2022 (during PHE) and July to September 2023 (post-PHE) in a single institution internal medicine residency clinic. We assessed the frequencies using χ2.
Results: A total of 11,358 patient visits met criteria. During the PHE, the majority were billed 99214 (4,602 of 5,557, or 82.8%) followed by 99213 (870 of 5,557, or 15.7%). Post-PHE, the majority were 99213 (4,000 of 5,801, or 68.3%) followed by 99214 (1,742 of 5,801, or 30.6%).
Conclusions: We observed an absolute 52.2% higher use of 99214 during the COVID-19 PHE expansion of the PCE. This finding has important implications for both clinic operations and education.
The Primary Care Exception (PCE) allows resident physicians to perform specific services with indirect attending physician supervision, without an attending directly seeing the patient.1 PCE frequency has been evaluated in family medicine, but not in other primary care specialties like internal medicine.2,3 The PCE is limited to the primary care setting when the resident has completed 6 months of training, and the supervising physician must ensure the quality of care. PCE applies to low-level complexity visits such as Current Procedural Terminology (CPT) 99213, whereas moderate and high level complexity, 99214 and 99215, are historically ineligible. Supervising physicians weigh multiple factors when electing to use the PCE, including resident autonomy, education, patient safety, and efficiency.4 During the COVID-19 Public Health Emergency (PHE), the PCE was expanded to moderate and high complexity visits, 99214 and 99215, from March 2020 to May 2023.5,6
PCE use during the PHE impacted billing in family medicine, as assessed by Cummings et al, specifically when comparing faculty and resident physicians.7 Importantly, that study predated the update to the Evaluation and Management Services billing guidelines, which included dramatically changed requirements for moderate and high complexity visits. Whether PCE frequency changed at other institutions and primary care specialties such as internal medicine is unknown. This study aimed to fill this gap.
We conducted a retrospective evaluation of a single residency continuity clinic with approximately 145 residents and 35 precepting faculty. The typical resident:faculty ratio was 3 : 1. The setting was an urban, hospital-based outpatient clinic. We performed analysis on billing data for CPT 99213, 99214, and 99215. Clinic policy required direct supervision for all new patients, preventive visits, and Medicare annual wellness visits, so we excluded those billing codes. Additional scenarios where the supervising physician directly saw patients included the first 6 months of residency training, posthospitalization visits, or request; all other visits used indirect supervision, a practice unchanged during the PHE.
We compared a 3 month sample of the PHE period (July–September 2022) with the post-PHE period (July–September 2023). We selected this period because all post-graduate year (PGY) one visits would have been conducted without the PCE, serving as a control for visit complexity. We used χ2 to determine the difference in use of 99213, 99214, and 99215 during (2022) and after (2023) the PCE expansion. Statistical analysis was performed using SPSS version 28.0 (IBM). The institutional review board reviewed and approved this study with ID number 202311074.
A total of 11,358 visits met our criteria. During the PHE, the majority were 99214 (4,602 of 5,557, or 82.8%) followed by 99213 (870 of 5,557, or 15.7%). In contrast, post-PHE, the majority were 99213 (4,000 of 5,801, or 68.3%) followed by 99214 (1,742 of 5,801, or 30.6%). These results are demonstrated in Table 1. The CPT 99215 billing code was infrequently used. The difference in CPT usage was statistically significant with a P value less than .001.
|
Billing code
|
During PHE, n (%)
|
Post-PHE, n (%)
|
P value
|
|
99213
|
870 (15.7)
|
4,000 (68.3)
|
<.001
|
|
99214
|
4,602 (82.8)
|
1,742 (30.6)
|
|
99215
|
85 (1.5)
|
59 (1.0)
|
|
Total
|
5,557
|
5,801
|
|
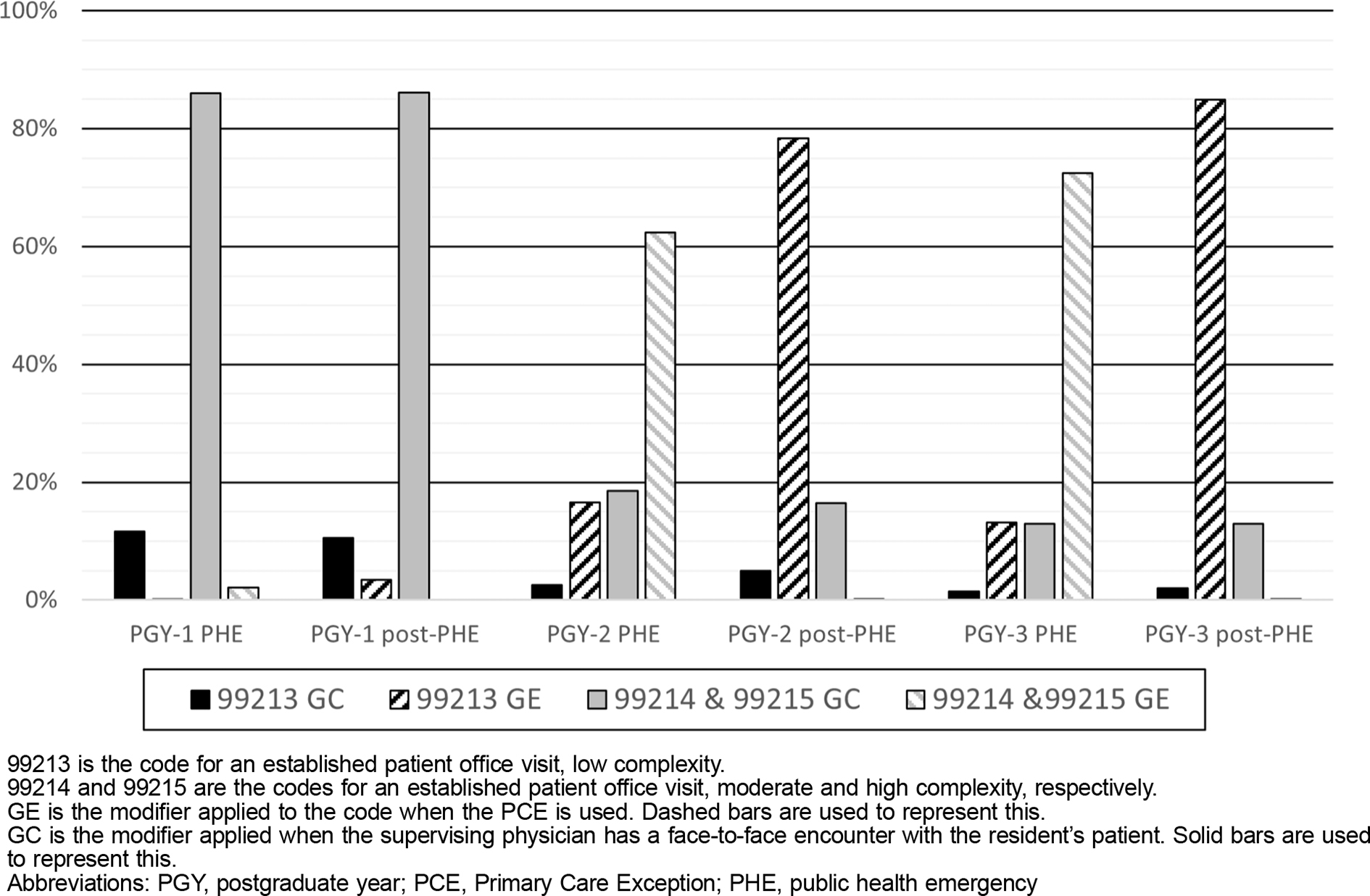
PGY-2 and PGY-3 residents had a near reversal of the frequency of 99213 and combined higher complexity 99214 and 99215 visits between the PHE and post-PHE periods (Table 2). Comparing the 2 years, PGY-3 residents went from having a higher rate of 99214 or 99215 use during the PHE (85.3% vs 80.8%) to a lower rate in the post-PHE period (13.0% vs 16.6%). The distribution of billing code use was similar for PGY-1 residents during the PHE and post-PHE periods, which was expected because they only had direct supervision.
|
Billing code
|
PGY-1 during PHE, n (%)
|
PGY-1 post-PHE, n (%)
|
PGY-2 during PHE, n (%)
|
PGY-2 post-PHE, n (%)
|
PGY-3 during PHE, n (%)
|
PGY-3 post-PHE, n (%)
|
|
99213
|
167 (11.8)
|
182 (13.9)
|
401 (19.2)
|
1,997 (83.4)
|
302 (14.7)
|
1,821 (87.0)
|
|
99214 & 99215
|
1,244 (88.2)
|
1,130 (86.1)
|
1,692 (80.8)
|
398 (16.6)
|
1,751 (85.3)
|
273 (13.0)
|
|
Total encounters
|
1,411
|
1,312
|
2,093
|
2,395
|
2,053
|
2,094
|
We found an absolute 52.2% higher use of 99214 during the PHE as compared to the post-PHE period. The main difference of decreased 99214 or 99215 visits appeared similar to the increased 99213 visits. This finding suggests that patients seen by PGY-2 and PGY-3 residents were typically moderate or high complexity but billed as 99213 during the post-PHE period because they were seen independent of the teaching physician (Figure 1). Additionally, 99214 or 99215 use was similar by PGY-1 residents during both periods at approximately 86%–88%, indicating this is the typical complexity for an established patient visit. The lower rate of 99214 or 99215 use by PGY-3 compared to PGY-2 residents in the post-PHE period suggests a higher use of indirect supervision, possibly due to progressive autonomy for residents over the course of their training. Importantly, this study adds to the literature by examining an additional primary care specialty and reporting specific rates of 99213, 99214, and 99215 visits, which has not been performed since the 2021 Evaluation and Management Services guidelines update.
We identified noteworthy implications of these results. Financially, the estimated revenue difference of 52.2% increased 99214 visits extrapolated to a full fiscal year, using estimated Medicare payment, could result in annual revenue increases exceeding $300,000.8 This amount likely underestimates revenue impacts, assuming commercial insurance reimburses higher than Medicare and Medicaid, and resident visit templates increase during typical year progression. Uncertainty exists regarding the optimal use of PCE for billing. Data and anecdotes from prior studies have suggested that 99214 and 99215 complexity visits may be billed as 99213 with indirect supervision.2,3,7 Proposed reasons for this finding include rule interpretation, preceptor availability, and resident physician autonomy.
Education is another important aspect of the PCE. Indirect supervision empowers greater resident physician autonomy, potentially promoting their patient care relationship and learning.9 Supervising faculty assess competence in residents through continuity clinic with longitudinal faculty-resident relationships and resident-patient relationships.10 Once competence is achieved, then expanded indirect supervision could follow, given observed increased use for PGY-3 residents compared to PGY-2. Additionally, residents need preparation in billing for independent primary care practice at the end of their training. If the majority of encounters bill 99213 with indirect supervision, then residents may not learn correct billing practices, an essential skill for lifelong clinical practice. Lack of formal education and feedback on billing during residency is cited as a reason for inaccuracies in faculty practice.11 Lastly, for education, policy limiting the PCE to low complexity visits is incongruent with competency-based training despite calls for this practice to be reexamined.12,13 For example, the majority of PGY-3 residents likely can address hypertension not at goal with adjustments in therapy plan with indirect supervision, yet this is a 99214 level of complexity. A change in the PCE from visit complexity-based to resident physician competency-based could result in focused use of direct supervision to those residents not yet demonstrating competence.
Importantly, this was a single institution study, and likely wide variations exist in clinic structure and use of the PCE by specific specialties and programs. The financial benefit of PCE expansion would vary by clinic in relationship to the average visit complexity. We hope our study prompts further assessment of additional outcomes, including patient care-related outcomes. While the PCE impact on these can be speculated, we believe that the current data support the position that re-expansion of the PCE would promote financial health of primary care clinics in multiple specialties.
In conclusion, this retrospective review of 11,358 patient visits found an absolute 52.2% higher use of 99214 during the COVID-19 PHE expansion of PCE as compared to after expansion ended. This finding has notable implications for financial success of residency continuity clinics and education.
The data from the study described in this manuscript were presented as an oral presentation at the University of Colorado Academy of Medical Educators in May 2024 and a poster presentation at the Society of General Internal Medicine Northwest Regional Meeting in March 2025. The content herein is substantially different from those presentations.
References
-
-
-
Harper PG, Adam P, Wooten M, et al. Financial impact of universal precepting in family medicine residency clinics.
Fam Med. 2020;52(1):24–30. doi:10.22454/FamMed.2019.690858
-
Patel R, Marquis TJ, Cook A, Gielissen K. A qualitative study of drivers for use of the primary care exception among internal medicine teaching faculty.
J Gen Intern Med. 2024;39(2):255–262. doi:10.1007/s11606-023-08406-x
-
Centers for Medicare & Medicaid Services. Medicare and Medicaid Programs; Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency. 85 Fed. Reg 19230. April 6, 2020. To be codified at 42 CFR parts 400, 405, 409, 410, 412, 414, 415, 417, 418, 421, 422, 423, 425, 440, 482, and 510. 2020. .
https://www.federalregister.gov/documents/2020/04/06/2020-06990/medicare-and-medicaid-programs-policy-and-regulatory-revisions-in-response-to-the-covid-19-public
-
-
Cummings A, Chiu N, Evans DV, Andrilla CHA, Cawse-Lucas J. Impact of primary care exception expansion on family medicine resident billing during the COVID-19 pandemic.
Fam Med. 2023;55(10):680–683. doi:10.22454/FamMed.2023.548357
-
-
Cantillon P, Macdermott M. Does responsibility drive learning? Lessons from intern rotations in general practice.
Med Teach. 2008;30(3):254–259. doi:10.1080/01421590701798703
-
Penner JC, Hauer KE, Julian KA, Sheu L. How preceptors develop trust in continuity clinic residents and how trust influences supervision: a qualitative study.
Perspect Med Educ. 2022;11(2):73–79. doi:10.1007/s40037-021-00694-5
-
Burks K, Shields J, Evans J, Plumley J, Gerlach J, Flesher S. A systematic review of outpatient billing practices.
SAGE Open Med. 2022;10. doi:10.1177/20503121221099021
-
Tobin DG, Doolittle BR, Ellman MS, Ruser CB, Brienza RS, Genao I. Modifying the primary care exception rule to require competency-based assessment.
Acad Med. 2017;92(3):331–334. doi:10.1097/ACM.0000000000001293
-
Gallagher BD, Vohra-Khullar PD, Fuest S, et al. The primary care exception rule in internal medicine residency clinic: benefits, disadvantages, best practices, and recommendations for reform.
J Gen Intern Med. 2025;40(6):1419–1423. doi:10.1007/s11606-024-09230-7



There are no comments for this article.