
Point-of-care ultrasound (POCUS) provides family physicians with real-time diagnostic and procedural capabilities, enhancing accuracy and efficiency in diverse settings. The Accreditation Council for Graduate Medical Education (ACGME) now recommends its inclusion in family medicine residency education.1 POCUS is increasingly essential in residency training; 53% of programs reported an established or developing curriculum, with top barriers being lack of trained faculty, equipment, and discomfort interpreting images.2,3 Evidence supports POCUS as a valuable tool in musculoskeletal (MSK), obstetric, abdominal, cardiopulmonary, and procedural care.4,5 Without a national standardized curriculum, individual programs must tailor training to faculty expertise, equipment availability, and patient populations. This paper details how we used an alumni survey to evaluate the effectiveness of our ultrasound program over the past 10 years by evaluating most useful teaching methods and barriers to use in practice.
BRIEF REPORTS
Evaluating the Point-of-Care Ultrasound Curriculum in a Family Medicine Residency: Challenges and Successes From a 10-Year Experience
Michael Henehan, DO† | William Hui, MD
Fam Med.
Published: 5/20/2026 | DOI: 10.22454/FamMed.2026.537627
Background and Objectives: Point-of-care ultrasound (POCUS) is increasingly recognized as a vital skill for family physicians, yet no standardized curriculum exists for its implementation in residency programs. This study used a survey of program graduates to evaluate a decade-long experience integrating POCUS into a family medicine residency.
Methods: We surveyed resident program graduates to assess the usefulness of POCUS training elements, frequency of use, and barriers to POCUS adoption in clinical practice.
Results: Survey results indicated that portable ultrasound access, workshops, and small-group sessions were the most valued training methods. Despite high participation in hands-on training, most graduates reported using POCUS infrequently in practice, citing barriers such as insufficient training, lack of access to devices, and time constraints. Notably, POCUS was most commonly used in musculoskeletal, obstetric, and soft tissue applications.
Conclusions: The implementation of a structured POCUS curriculum in family medicine residency is feasible and beneficial, particularly when supported by institutional resources and faculty engagement. However, persistent barriers to routine use in clinical practice highlight the need for ongoing support, access to equipment, and mentorship postgraduation to enhance POCUS adoption among family physicians.
Program Development
Our POCUS journey began in 2012 when the affiliated sports medicine fellowship adopted ultrasound for musculoskeletal applications. Simultaneously, family medicine obstetrics faculty used ultrasound in prenatal care with our first cart-based unit. Early resident exposure was informal and focused on faculty interests.
Formal curriculum development began in 2016 using a cart-based unit and loaner devices from Sonosite. In 2019, the program purchased handheld ultrasound units for all 24 residents and 12 core faculty, enabling consistent inpatient and outpatient practice. Concurrently, monthly workshops were included as part of the curriculum. In 2025, we launched a POCUS track with enhanced competency documentation via study overreads and observed structured clinical exams (OSCEs).
Four faculty members have extensive MSK expertise, five are proficient in obstetric ultrasound, three use ultrasound occasionally, and three are not comfortable scanning independently. The POCUS lead is trained across MSK and diagnostic applications.
The POCUS lead has 0.3 full-time equivalent of faculty time dedicated to structured teaching, including weekly half-day MSK ultrasound training for sports medicine fellows, monthly 2 hour workshops for all residents, weekly inpatient POCUS rounds, and quarterly scanning sessions for POCUS track residents.
Curriculum Structure
Applications Taught
- Inpatient: Cardiac, lung, kidney/bladder, deep vein thrombosis, gallbladder, soft tissue
-
Outpatient: MSK (shoulder, knee, hip, elbow, hand/wrist), soft tissue, and ultrasound-guided procedures
Teaching Strategies
-
Hands-on workshops featuring a POCUS core topic each month
-
Small group scanning sessions (POCUS parties)
-
Inpatient POCUS rounds
-
Learner-as-teacher model (senior residents training juniors)
-
Faculty overreads of saved images
-
Online resources and directed readings
Competency Assessment
-
OSCEs for technical and interpretive skills (introduced in 2021; 28% of surveyed graduates had participated)
-
Scan logs
-
Faculty overread verification (asynchronous)
In May and June 2025, we sent a 13-question online survey to Stanford–O’Connor Hospital family medicine residency program graduates from 2012 to 2024. The survey included multiple choice, ranked, and open-ended questions, and collected information on POCUS training, fellowships, clinical practice settings, perceived usefulness of POCUS training elements, average number of POCUS scans, POCUS utility, and barriers. This project was exempt from Stanford University’s Institutional Review Board process.
Survey Results
A survey of alumni with a response rate of 61% (59/96) provided insight into training effectiveness and postresidency POCUS use. The pre-2019 cohort (pre-handheld US implementation) had 33 responses; the post-2020 cohort (post-handheld US implementation) had 26 responses.
Practice Settings
Nearly all graduates worked in outpatient settings (97%). A minority also work in inpatient care (25%), urgent care (25%), or labor and delivery (7%). Regarding procedures, 44% performed outpatient procedures and 3% performed inpatient procedures.
Useful Training Elements
The most useful elements were personal handheld ultrasound access, workshops, and small-group sessions. Overall, 79% of respondents ranked having a portable ultrasound device in their top three most useful elements, followed by 78% for workshops, and 65% for small-group training sessions. Conversely, overreads, directed readings, and OSCE were rated least useful. A total of 77% ranked overreads in their bottom three, followed by 35% for directed readings, and 38% for OSCEs.
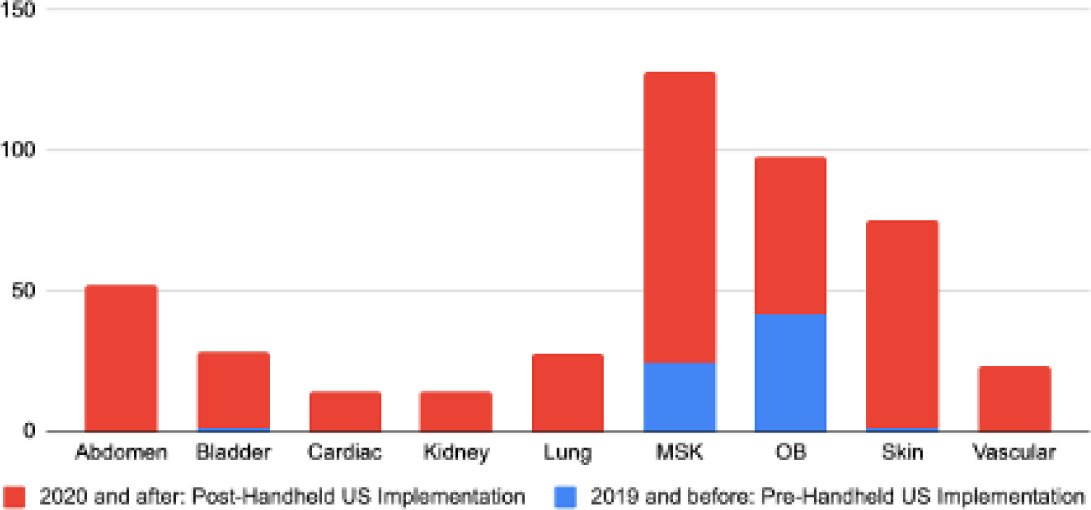
Common Applications in Practice
Obstetric and MSK studies accounted for the majority of the POCUS use, followed by soft tissue, abdomen, and bladder. This finding was consistent with several European and Canadian primary care studies (Figure 1).4,6,7
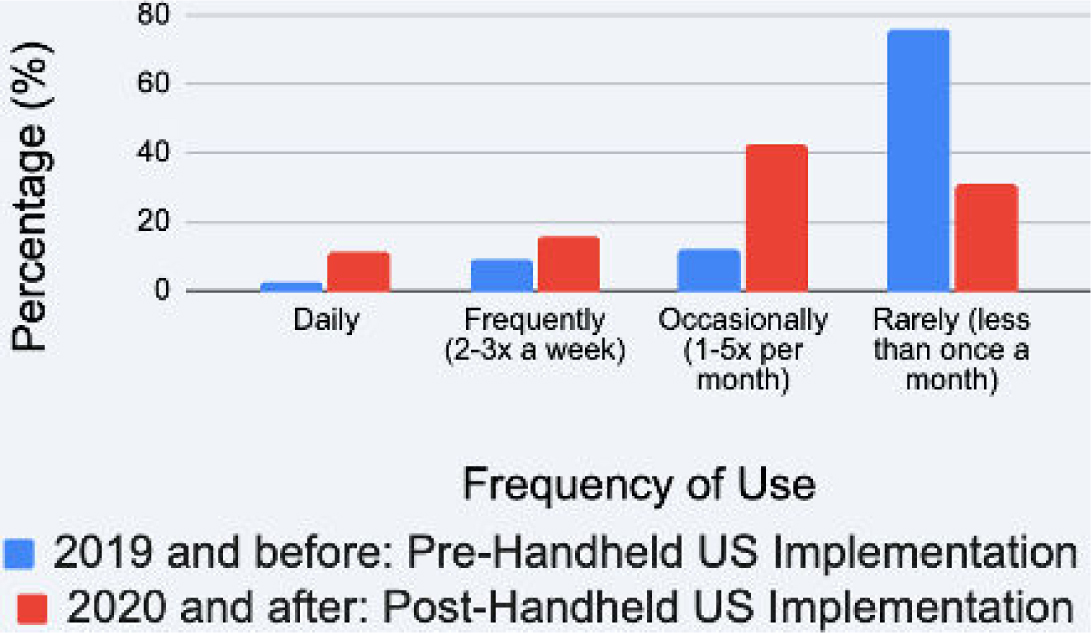
Frequency of Use Postgraduation and Barriers
Residents with handheld access during training reported more frequent postgraduation POCUS use (Figure 2). For graduates trained before handheld US implementation (before 2019), top barriers were insufficient training in image acquisition (61%), insufficient interpretation skills (61%), and lack of ultrasound access (42%). After handheld US implementation (2020 and after), top barriers were time (54%), inability to save images directly to the electronic medical record (EMR; 54%) and inability to receive feedback for saved images (46%; Table 1).
Top POCUS barriersa |
2019 and before: |
2020 and after: |
|---|---|---|
Not enough training for image acquisition |
20 (60.61) |
9 (34.62) |
Not enough training for image interpretation |
20 (60.61) |
11 (42.31) |
No ultrasound unit accessible |
14 (42.42) |
5 (19.23) |
Time |
13 (39.39) |
14 (53.8) |
Inability to receive feedback for saved images |
8 (24.24) |
12 (46.15) |
Inability to bill for limited POCUS studies |
6 (18.18) |
9 (34.62) |
Inability to save images directly into an electronic medical record |
5 (15.15) |
14 (53.8) |
Worried about inadequate documentation |
5 (15.15) |
6 (23.08) |
No barriers. I use POCUS regularly. |
3 (9.09) |
3 (11.54) |
aBarriers receiving only one response were excluded.
Abbreviation: POCUS, point-of-care ultrasound
Successes and Outcomes
Survey results reinforced the program’s emphasis on teaching methods that are hands-on and learner-centered, with the highest-rated training elements being portable US access, workshops, and small-group training sessions. These findings align with literature showing that repeated supervised practice drives skill retention.8,9,10,11,12
Implementation of a structured curriculum increased resident and faculty use, particularly in MSK, obstetric, and skin applications. Personal handheld devices spurred greater POCUS utilization in practice (Figure 2). Participants who engaged more in hands-on training reported higher confidence and continued, though infrequent, use after graduation.
Challenges
Challenges identified through both program experience and graduate feedback included.
Lack of faculty breadth. Early expertise was concentrated in MSK and obstetrics, with slower uptake in abdominal and cardiopulmonary applications.
Equipment access. Handhelds improved access during residency, but many graduates lacked devices usable in current practice.
Workflow integration. Time constraints, limited ability to save images to EMR, and inability to receive feedback for saved images were notable barriers in the post-handheld cohort.
Competency and confidence. Insufficient training for image acquisition and interpretation remained a barrier, though less so after handheld US implementation.
Systems issues. Limited EMR integration, feedback opportunities, and billing capabilities deterred adoption.
Handheld ultrasound access, workshops, and small-group sessions were the most impactful training methods, earning the highest usefulness ratings and aligning with studies showing that interactive, case-based learning outperforms passive approaches.9,13,14
However, skill retention and translation into routine practice remained limited. Barriers to continued training, device access, and time constraints mirrored POCUS study findings in primary care.3 Residency training alone may not ensure routine use; ongoing practice support, reliable device access, and postgraduation mentorship may be necessary.
Applications practiced most during residency are most likely to be used in practice. The predominance of MSK, obstetric, and soft tissue scans during training and postgraduation underscores the importance of aligning curricula with common clinical needs and feasible outpatient workflows. Faculty champions and institutional support are critical. Program growth depended on dedicated teaching time, device investment, and faculty development. Sustaining a POCUS curriculum without these elements is challenging. Based on survey results, we will prioritize hands-on scanning and strengthen our competency-based evaluation. Our survey cohort largely predated the POCUS track. Future evaluation will assess whether the enhanced track reduces barriers and increases adoption.
With institutional support, faculty champions with dedicated teaching time, and emphasis on practical training, a structured POCUS curriculum can be successfully implemented in family medicine residency. Survey results confirmed the value of hands-on learning but highlighted persistent barriers to routine use, particularly postgraduation. Addressing time constraints, EMR integration and feedback, and postresidency support may increase adoption.
†Drs Michael Henehan and William Hui contributed equally to this study.
References
-
ACGME Program Requirements for Graduate Medical Education in Family Medicine. ACGME; 2025. Accessed April 20, 2026. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/120_familymedicine_2025_reformatted.pdf
-
Point of care ultrasound in family medicine residency programs: a CERA Study. Fam Med. 2015;47(9):706–711. https://www.stfm.org/familymedicine/vol47issue9/Hall706
-
Point-of-care ultrasound in family medicine residencies 5-year update: a CERA study. Fam Med. 2020;52(7):505–511. doi:10.22454/FamMed.2020.223648
-
Point-of-care ultrasound for general practitioners: a systematic needs assessment. Scand J Prim Health Care. 2020;38(1):3–11. doi:10.1080/02813432.2020.1711572
-
Point-of-care ultrasonography. N Engl J Med. 2021;385(17):1593–1602. doi:10.1056/NEJMra1916062
-
Use and impact of point-of-care ultrasonography in general practice: a prospective observational study. BMJ Open. 2020;10(9). doi:10.1136/bmjopen-2020-037664
-
Point of care ultrasound training needs for primary care physicians: Practice setting matters. Cogent Education. 2019;6(1):1617826. doi:10.1080/2331186X.2019.1617826
-
Not just hocus POCUS: implementation of a point of care ultrasound curriculum for internal medicine trainees at a large residency program. Mil Med. 2019;184(11-12):901–906. doi:10.1093/milmed/usz124
-
Point-of-care ultrasound track in an academic family medicine department. PRiMER. 2024;8. doi:10.22454/PRiMER.2024.363716
-
Skill retention with ultrasound curricula. PLoS One. 2020;15(12). doi:10.1371/journal.pone.0243086
-
Is ultrasound training sustainable? A systematic review of competency retention in healthcare trainees. Med Educ. 2025;59(12):1290–1305. doi:10.1111/medu.15751
-
General practitioners’ scanning competence following tailored ultrasound training: a hybrid effectiveness-implementation study. BMC Med Educ. 2025;25(1). doi:10.1186/s12909-025-07356-8
-
Comparison of the didactic lecture with the simulation/model approach for the teaching of a novel perioperative ultrasound curriculum to anesthesiology residents. J Clin Anesth. 2014;26(6):443–454. doi:10.1016/j.jclinane.2014.01.018
-
Integration of point of care ultrasound into undergraduate medical education at texas tech university health sciences center school of medicine: a 6 year review. BMC Med Educ. 2024;24(1). doi:10.1186/s12909-024-06483-y
Lead Author
Michael Henehan, DO†
Affiliations: Family Medicine Residency, Stanford–O’Connor Hospital, San Jose, CA | † Drs Michael Henehan and William Hui contributed equally to this study.
Co-Authors
William Hui, MD - Division of Primary Care and Population Health, Department of Medicine, Stanford University School of Medicine, Stanford, CA
Corresponding Author
William Hui, MD
Correspondence: Division of Primary Care and Population Health, Department of Medicine, Stanford University School of Medicine, Stanford, CA
Email: whui@stanford.edu
Fetching other articles... 
Loading the comment form...
Submitting your comment...

There are no comments for this article.