Background and Objectives: Point-of-care ultrasound (POCUS) is increasingly used in inpatient settings to evaluate patients. Common applications include cardiac, lung, hemodynamic assessment, and venous access. Teaching and achieving competency in these applications are highly resource intensive and require hours of dedicated faculty support. We evaluated the impact of a hybrid asynchronous and hands-on inpatient POCUS curriculum for family medicine residents transitioning from intern to senior roles.
Methods: Family medicine residents participated in an inpatient POCUS course during a dedicated 2 week transition period between postgraduate years (PGYs) 1 and 2. The curriculum included 100 minutes of asynchronous precourse videos followed by a 4 hour in-person session with POCUS trained faculty. The hands-on session included scanning live patients and ultrasound-guided venous access on homemade task trainers. Participants completed pre- and postintervention surveys as well as a written examination.
Results: Thirteen family medicine residents completed the course. Participants reported an increase in overall comfort with inpatient POCUS, with a mean improvement of 0.9 points on a 5-point Likert scale composite score (p<0.001). Self-reported comfort improved across all domains, including image acquisition, image interpretation, and clinical integration. Written examination scores did not improve preintervention (64.1%) to postintervention (65.4%) intervention (P = 0.78).
Conclusions: A brief hybrid inpatient POCUS course was associated with improved confidence in performing and integrating POCUS exam types for the inpatient setting, but did not result in improvement in a written knowledge assessment. These findings suggest that a short introductory boot camp can be beneficial and may be strengthened with a longitudinal curricula and more robust competency assessments.
Point-of-care ultrasound (POCUS) is increasingly recognized as a valuable tool in inpatient settings. Specifically, cardiopulmonary ultrasound has been shown to improve hospital efficiency, highlighting its clinical utility to improve diagnostic accuracy and inform medical decision-making.1 For family physicians providing inpatient care, competency in core applications such as cardiac, lung, hemodynamic assessment, and venous access is becoming more relevant to daily practice.
In recognition of the growing importance of POCUS, the Accreditation Council on Graduate Medical Education recently mandated POCUS as a required skill for family medicine residency training.2 However, many family medicine training programs face significant challenges in developing robust curricula that cover a wide range of clinical settings.3,4 Achieving competency in inpatient POCUS is resource intensive because trainees must reach competency in all three domains of POCUS: image acquisition, image interpretation, and clinical integration. It requires longitudinal exposure and deliberate practice with dedicated faculty who can provide lectures, bedside teaching, image review, and quality assurance.5
A paucity of literature exists evaluating the impact of either a short-term or longitudinal inpatient POCUS curriculum tailored for family medicine residents.6,7 Existing literature on this topic has focused primarily on emergency medicine and internal medicine programs.8,9
To address this gap at our institution, we developed an educational intervention that sought to evaluate the impact of a brief introductory hybrid inpatient POCUS curriculum targeted at family medicine residents transitioning from postgraduate year (PGY) 1 to 2. We hypothesized that participation would be associated with increased self-reported comfort and improved knowledge in inpatient POCUS across all three core domains.
Study Design
This was a single institution pre-post educational intervention evaluating a hybrid inpatient POCUS curriculum. Our institutional review board reviewed and determined this intervention to be program evaluation and not human subjects research.
Participants
All eligible PGY-1 residents from a single family medicine residency program were enrolled. The course was delivered at the end of the 2024–2025 academic year during a dedicated 2 week transition period designed to help prepare PGY-1 residents for increasing inpatient responsibilities as PGY-2 residents. Family medicine faculty teach and perform POCUS during inpatient rotations at this residency.
Curriculum Content
The curriculum was developed using the American Academy of Family Physician recommended POCUS guidelines.5 Content was selected based on common applications relevant to family medicine inpatient practice, including basic ultrasound physics and knobology, cardiac (left ventricular systolic function, right ventricular assessment, pericardial effusion), lung (pneumothorax, pulmonary edema, pleural effusion, pneumonia), hemodynamic assessment (RUSH [rapid ultrasonography in shock and hypotension], FAST [focused assessment with sonography for trauma] protocols), and ultrasound-guided vascular access.
Educational Intervention
Participants were given approximately 100 minutes of mandatory online videos to complete prior to an in-person session with POCUS-trained faculty (https://coreultrasound.com). Additional textbooks, articles, and videos were provided as optional supplementary resources. All materials were curated using Free Online Access Medical Education sources.
Residents participated in a 4 hour faculty-led session with a learner-to-faculty ratio of no more than three to one. Hands-on scans were performed on five to 10 emergency department patients. Participants practiced ultrasound-guided vascular access using homemade task trainers. Cart-based ultrasound machines (Mindray TE-X) were used for all scans and procedures.
Participants completed surveys and written examinations before the in-person session (after online videos had been completed) and again after the hands-on session. The survey included questions on prior ultrasound experience and comfort with the POCUS domains on four exam types: cardiac, lung, inferior vena cava, and hemodynamic assessment. Participants also rated their comfort in performing ultrasound-guided vascular access. Responses were based on a 5-point Likert scale ranging from “very NOT confident” to “very confident”.
Participants were assigned one of two 12-question exams (Form A or B) to assess objective knowledge in identifying sonographic anatomy, image optimization, pathology identification, and clinical integration with three questions assessing each of these areas. Following the intervention, participants took the alternate exam.
Statistical Analysis
We analyzed data in SPSS (IBM) using Wilcon nonparametric testing after identifying nonnormally distributed confidence and test scores. For confidence scores, we compared precourse and postcourse scores directly. We calculated the change in confidence scores across each of the aforementioned POCUS domains, exam type, and composite score for overall confidence (excluding vascular access). For test scores, we compared performance pretest to posttest for each topic area and for overall scores.
Thirteen family medicine residents completed the course. Baseline self-reported experience varied among participants, although most reported limited prior experience. Ten out of 13 residents reported 10 or fewer prior studies in each of the four applications, with a wide range of reported numbers of exams overall (Table 1).
Study type |
Self-reported prior studies performed: Median (IQR) [range] |
Cardiac |
6 (4–10) [3–50] |
Lung |
5 (3–10) [1–50] |
Inferior vena cava |
3 (3–10) [0–30] |
Hemodynamic assessment (RUSH or FAST protocol) |
3 (1–10) [0–50] |
Vascular access |
0 (0–3) [0–100] |
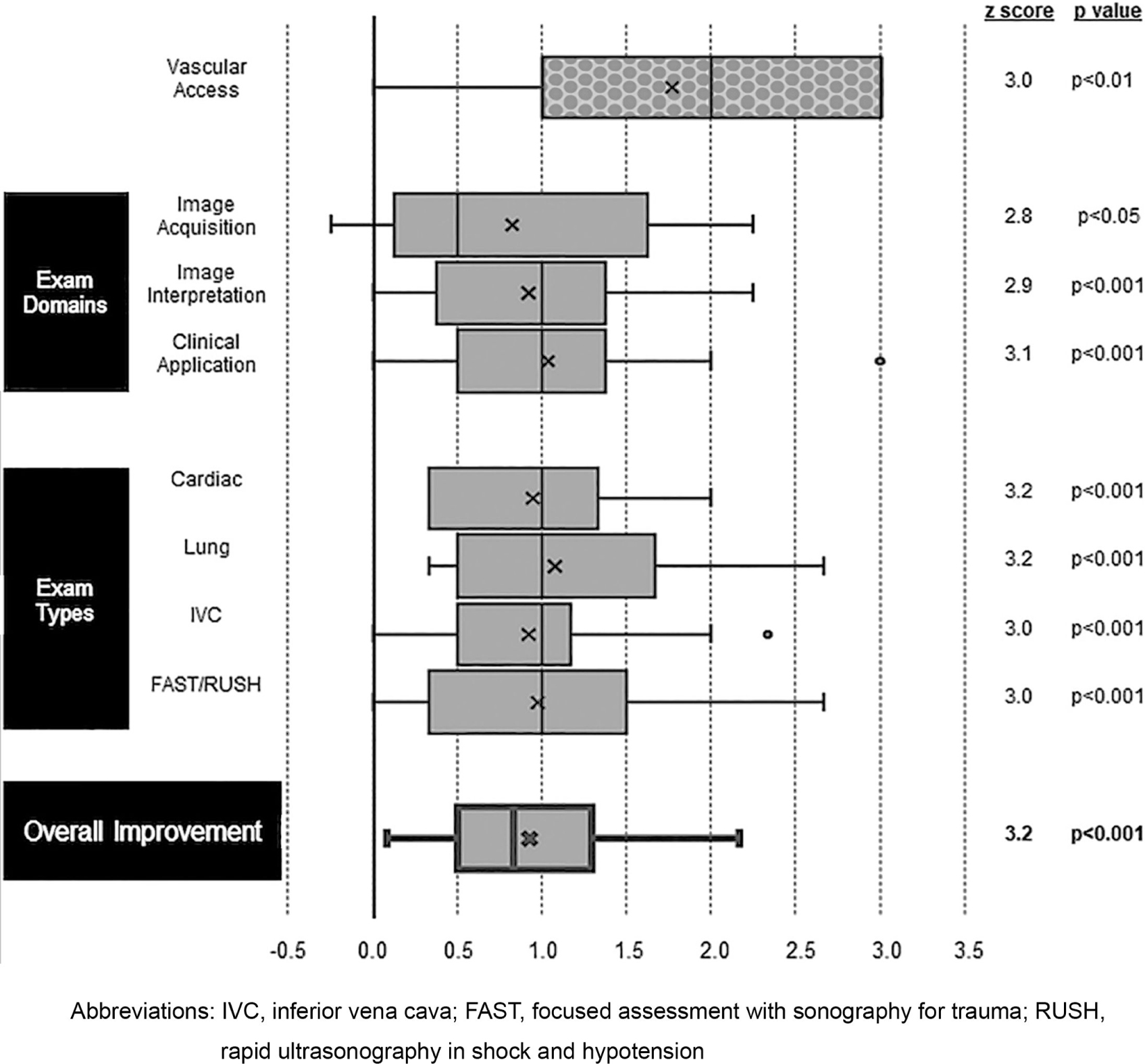
Participants rated improved postcourse comfort in all individual exam types and domain pairings. When averaged across all domain and exam types, participants reported a mean improvement of 0.9 points, corresponding to an overall shift from “neutral” to “somewhat comfortable” (z score: 3.2, 95% CI: 0.6 to 1.5, P<0.001; Figure 1). Participants rated improved confidence in performing ultrasound-guided vascular access, with a mean categorical improvement of 1.8 points, corresponding to an improvement from “somewhat uncomfortable” to “somewhat comfortable” (z score: 3.0, 95% CI: 0.8 to 2.5, P<0.01).
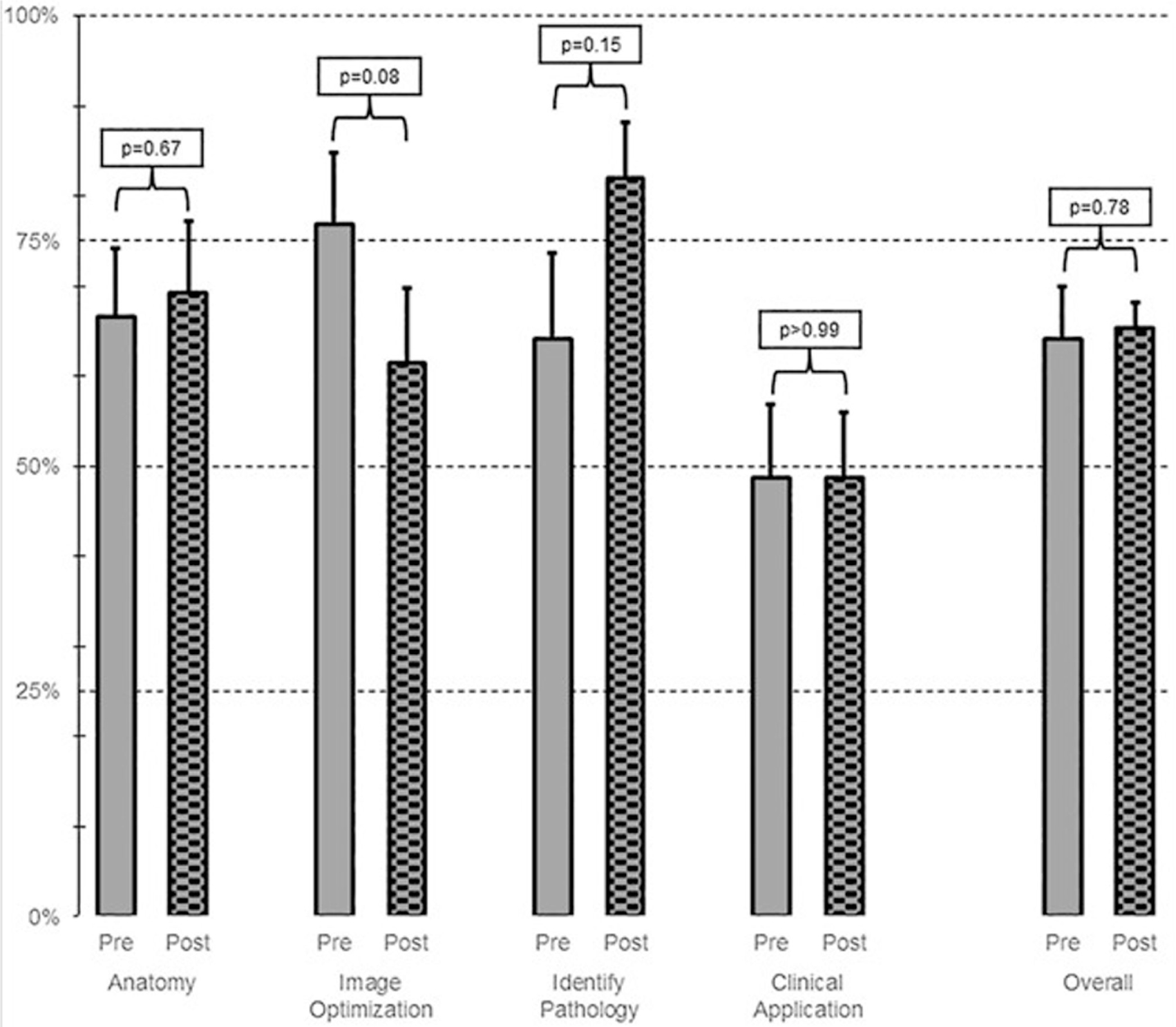
Written exam performance did not significantly change from precourse to postcourse (64.1%–65.4%, P = 0.78). Participants had an improved ability to identify pathology, a trend that did not reach statistical significance (Figure 2).
In this pre-post educational intervention, a brief inpatient hybrid POCUS course was associated with a meaningful increase in self-reported comfort across core inpatient applications and the domains of image acquisition, image interpretation, and clinical interpretation.
Although self-reported comfort improved, written exam performance did not. This discordance may be explained by several factors. First, the baseline pretest was administered after completion of the online videos, likely affecting our ability to assess knowledge gains from the curriculum as a whole. Secondly, a written assessment tool has limited ability to assess competency in image acquisition, which may be better assessed with performance-based tools such as an objective structured clinical examination or standardized direct observation tool. Furthermore, given the variety of patients encountered during the in-person session, variation in hands-on training was likely. Future courses could incorporate standardized patients to streamline hands-on training and reduce variability in scanning opportunities. Lastly, confidence possibly can increase while objective knowledge is still developing. This possibility underscores that self-reported comfort should not be uniformly equated with competence in all domains of POCUS.
Nevertheless, early exposure to inpatient POCUS may still be valuable during the transition from PGY-1 to PGY-2, especially at a training program where inpatient POCUS is used. A focused introductory curriculum during this transition period offers a safe venue to build foundational skills, increase learner confidence, and identify gaps that require longitudinal reinforcement during inpatient rotations.
Limitations of this educational intervention included single institution design, small sample size, reliance on self-reported confidence, and use of a written knowledge test. Future work should evaluate retention of skills, integration on inpatient rotations, and the validity of assessment tools for family medicine–relevant inpatient POCUS competency.
Overall, our findings suggest that an inpatient POCUS bootcamp can serve as an introduction but not as a standalone pathway to competency. As a family medicine program facing limited time with POCUS-trained faculty and other competing curricular demands, a brief hybrid course was feasible and scalable.
References
-
Maganti K, Chen C, Jamthikar AD, Parikh P, Yanamala N, Sengupta PP. Cardiopulmonary point-of-care ultrasonography for hospitalist management of undifferentiated dyspnea.
JAMA Netw Open. 2025;8(9). doi:10.1001/jamanetworkopen.2025.30677
-
-
Capizzano JN, O’Dwyer M-C, Furst W, et al. Current state of point-of-care ultrasound use within family medicine.
J Am Board Fam Med. 2022;35(4):809–813. doi:10.3122/jabfm.2022.04.220019
-
Ludden-Schlatter A, Kruse RL, Mahan R, Stephens L. Point-of-care ultrasound attitudes, barriers, and current use among family medicine residents and practicing physicians.
PRiMER. 2023;7. doi:10.22454/PRiMER.2023.967474
-
-
Andersen CA, Holden S, Vela J, Rathleff MS, Jensen MB. Point-of-care ultrasound in general practice: a systematic review.
Ann Fam Med. 2019;17(1):61–69. doi:10.1370/afm.2330
-
Hall JWW, Holman H, Barreto TW, et al. Point-of-care ultrasound in family medicine residencies 5-year update: a CERA study.
Fam Med. 2020;52(7):505–511. doi:10.22454/FamMed.2020.223648
-
Mandavia DP, Aragona J, Chan L, Chan D, Henderson SO. Ultrasound training for emergency physicians--a prospective study.
Acad Emerg Med. 2000;7(9):1008–1014. doi:10.1111/j.1553-2712.2000.tb02092.x
-
Mellor TE, Junga Z, Ordway S, et al. implementation of a point of care ultrasound curriculum for internal medicine trainees at a large residency program.
Mil Med. 2019;184(11-12):901–906. doi:10.1093/milmed/usz124



There are no comments for this article.