I read Dr Schrager’s recent editorial1 with great interest. As an international medical graduate preparing for family medicine residency and an academic career, I found her call for structured leadership curricula particularly resonant. However, teaching leadership skills is only one piece of the puzzle; the other crucial piece is how to effectively support underrepresented in medicine (URiM) trainees—specifically Hispanics/Latinos—who aspire to academic leadership but lack representative role models, sponsors, and institutional guides.
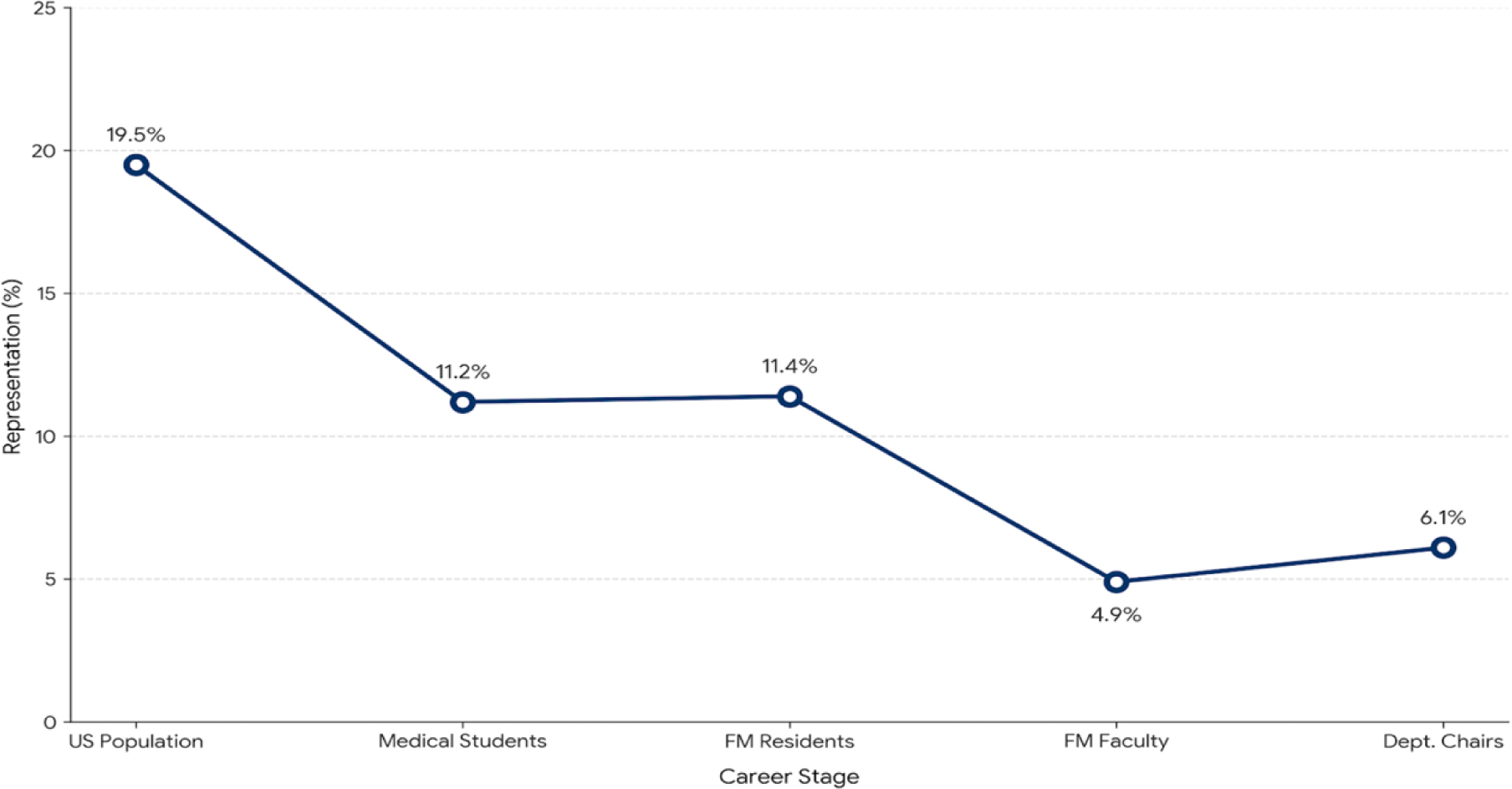
To complement her perspective, I analyzed Association of Academic Medical Colleges and US Census data2,3,4,5 to describe the structural landscape that URiM aspiring leaders face, visualizing Hispanic/Latino representation across the academic medical trajectory (Figure 1).
The data reveal a disrupted pathway. While Hispanics/Latinos comprise 19.5% of the US population, they represent 11.2% of medical school matriculants and 11.4% of family medicine residents. However, this participation drops sharply to 4.9% among family medicine faculty and 6.1% at the department chair level.
To quantify this decline, I employed a beta-binomial Bayesian probabilistic analysis (BPA). BPA quantifies disparities in small, imbalanced samples where frequentist models fail.6 A BPA of this trajectory reveals a steep decline [Relative Proportion 0.43; 95% Credible Interval (CrI): 0.40–0.46], indicating that Hispanic/Latino family medicine residents have a 57% lower likelihood of entering academic roles compared to their representation in training and 46% lower likelihood of attaining leadership roles as chairs (Relative Proportion 0.54; 95% CrI: 0.30–0.85). This mathematically confirms previously identified gaps7,8, transforming qualitative observations into a measurable structural deficit.
This disruption in the academic pathway creates a vicious cycle: without Hispanic/Latino faculty in decision-making roles, residents lack the mentors who share their lived experiences and identities to help them envision themselves as future academic leaders.
These findings underscore the structural challenges facing Dr Schrager’s call to action and highlight the potential need for targeted interventions. Effective leadership training for URiM family physicians requires more than standard mentorship; it demands “institutional navigation” and “strategic sponsorship.” These two are intrinsically connected: while navigation provides the understanding of the academic landscape, sponsors actively use their political capital to advocate for the protégés’ advancement through it. This is especially urgent given that residents cite a lack of mentorship as their primary fear regarding academic careers.9 Future studies comparing institutions with varying representation levels could help identify successful models of sponsorship and institutional guidance.
Aggregated data likely mask deeper inequities among Hispanic/Latino subgroups. Therefore, disaggregating these data in future research is essential, as current literature is only scratching the surface of underrepresentation. While the financial allure of nonacademic roles also impacts recruitment,10 the persistent representation gap within the academy underscores a structural deficit.
For URiM residents, institutional navigation is an essential leadership tool, not an optional soft skill. To learn and hone these skills, trainees require guidance from senior, supportive URiM faculty. We need more representative leaders, and we need them now— strong leadership training without representative role models will fall short when it comes to our ultimate goals of diversifying our workforce and better serving our most vulnerable patients.



There are no comments for this article.