Background and Objectives: Increasing the representation of female and Black, Indigenous, and People of Color (BIPOC) identities among family medicine faculty leaders is important for improving community health outcomes. While prior studies show rising percentages, they don’t clarify whether these gains stem from recruitment or retention. We examined the proportion of leaders who are female and BIPOC to determine how long they’ve held their roles.
Methods: We conducted a secondary analysis of Council of Academic Family Medicine Educational Research Alliance (CERA) survey data from 2011 to 2023. Leadership duration was classified as <1 year (recruitment) and ≥5 years (retention). Descriptive statistics and Pearson’s correlation test evaluated trends in duration across leadership roles over time.
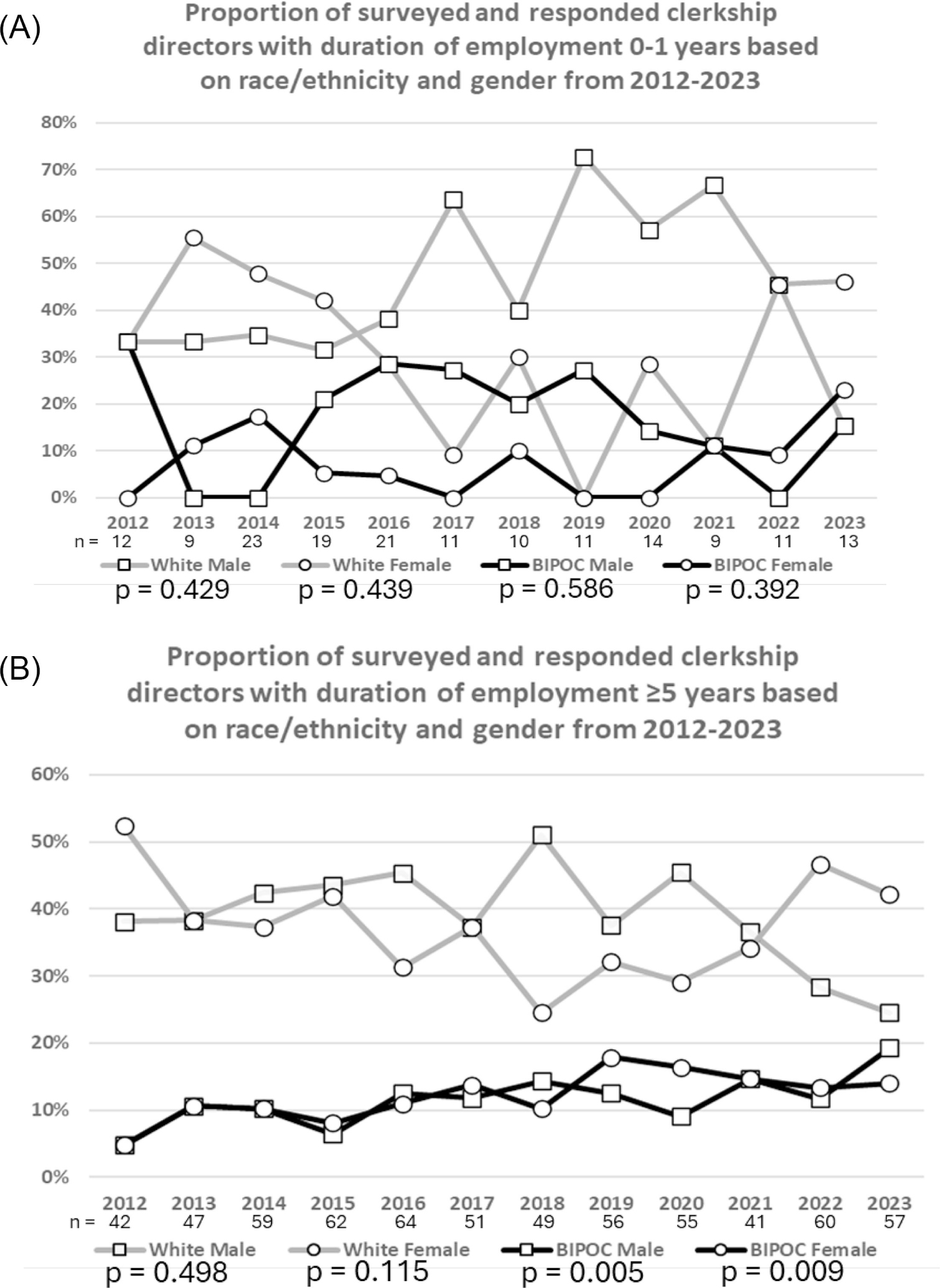
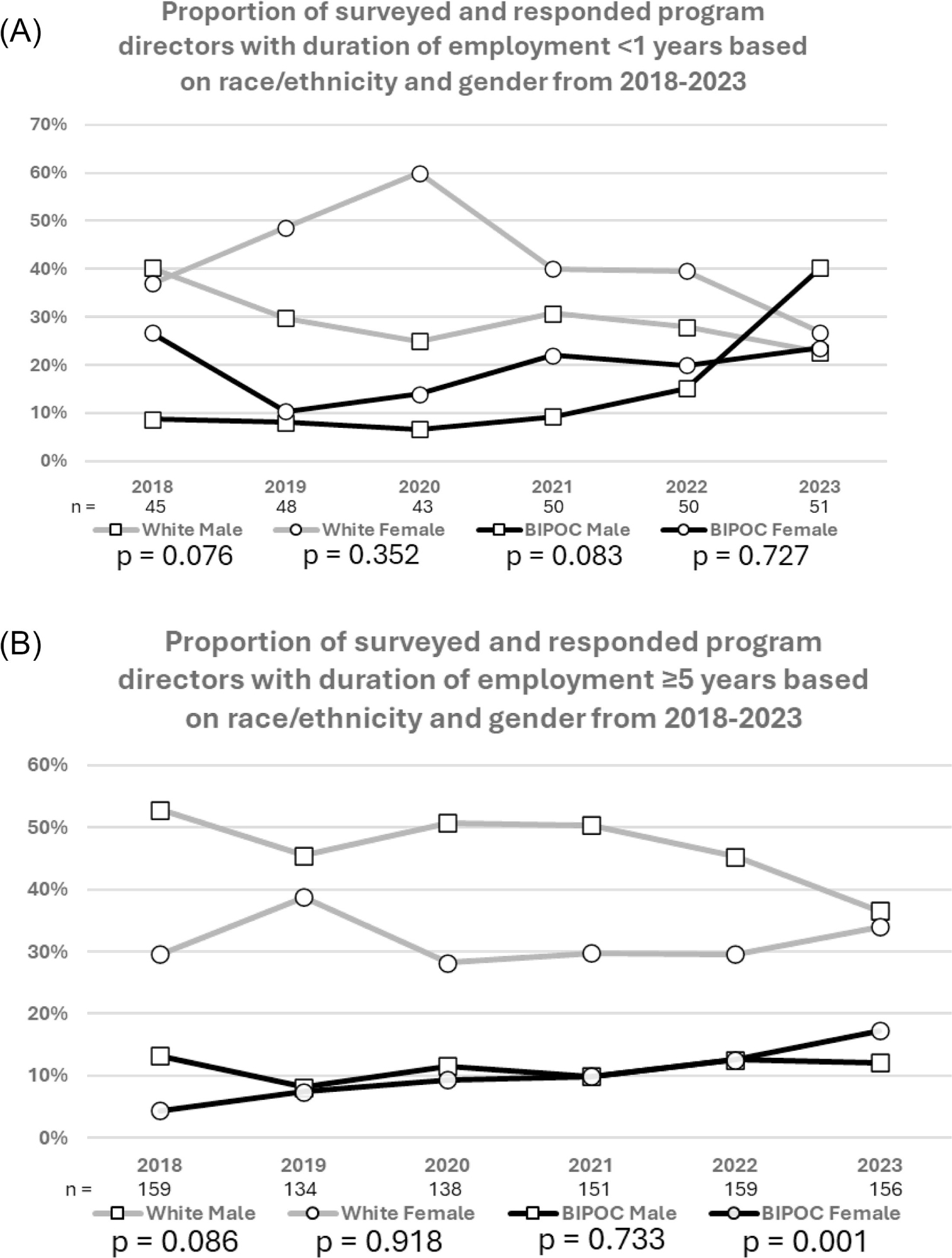
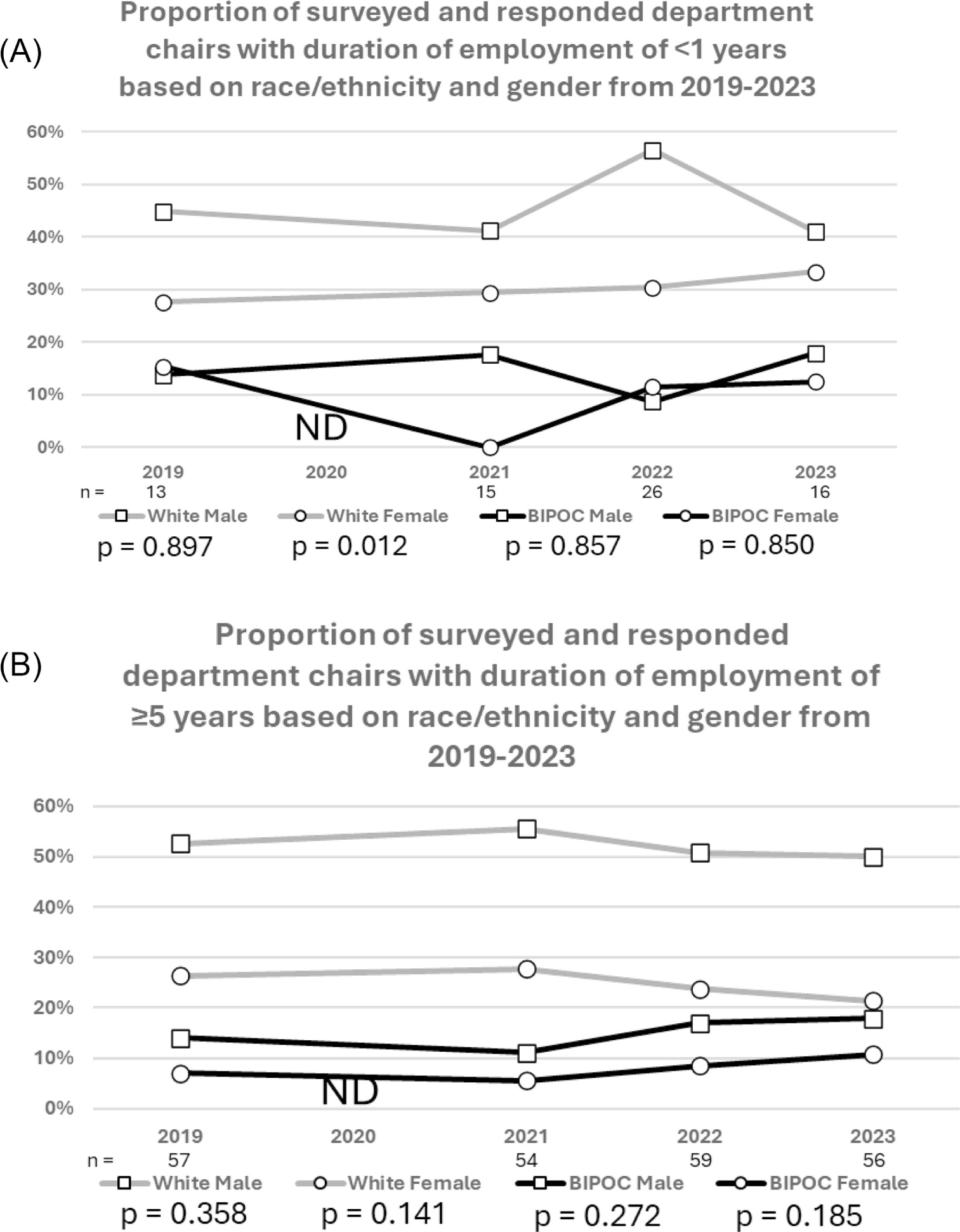
Results: Increases in BIPOC representation were observed only among leaders with ≥5 years of duration. Increases in the proportion of BIPOC male and female clerkship directors with ≥5 years rose from 4.8% each in 2012 to 19.3% and 14.0% in 2023 (P=0.005, P=0.009). BIPOC female program directors with ≥5 years of duration increased from 4.4% in 2018 to 17.3% in 2023 (P=0.001). No significant trends were identified among department chairs or among leaders with <1 year of duration.
Conclusions: In family medicine academic leadership, observed increases in BIPOC men and women clerkship directors and BIPOC women program directors are driven by retention rather than recruitment into leadership roles. Departments should therefore sustain and scale retention practices while implementing formal mentorship and sponsorship programs, transparent promotion pathways, and targeted outreach to ensure equitable growth in leadership diversity.
A diverse physician workforce improves health outcomes by reducing disparities, advancing equity, and strengthening population health.1,2 Academic medicine leadership plays a pivotal role in shaping workforce diversity; however, Black, Indigenous, and People of Color (BIPOC) and females remain underrepresented in these positions due to persistent systemic barriers.3-6 Although prior initiatives have advanced gender and racial/ethnic representation, sustaining and expanding these gains remains an ongoing challenge.
In family medicine, notable increases in academic leadership diversity have been documented.7-10 Studies report significant upward trends in the number of female clerkship directors (CDs), program directors (PDs), and department chairs (DCs).7-10 Similarly, research shows increased representation of BIPOC faculty in these roles over the past decade.7-10 We sought to determine whether gains in family medicine academic leadership diversity are a result of recruitment or retention.
We performed a longitudinal secondary analysis of publicly available cross-sectional Council of Academic Family Medicine Educational Research Alliance (CERA) survey studies from the online CERA Data Clearinghouse.11 CERA conducts cross-sectional surveys of family medicine CDs, PDs, and DCs which begin with standardized questions regarding the demographic data of the respondents. Methodology papers have validated the representativeness of CERA survey respondents.12-14 Surveys were approved by the American Academy of Family Physicians’ Institutional Review Board prior to their administration.
We abstracted demographic data (gender, race/ethnicity, and duration) from all CERA CD, PD, and DC surveys in which all three variables were collected from 2011 to 2023. Respondents with missing demographic data were excluded. We defined duration as duration of employment. We looked for significant change in the percent of leaders who are female, BIPOC, and intersected female and BIPOC and who had a duration of <1 year or ≥5 years. We chose a threshold value of five years in the position to define retainment after not finding a standard validated threshold in the literature. This threshold of ≥5 years represented the common average median duration amongst all three academic leaders in our dataset (CD- 5 years; PD- 4.79 years; DC- 4.83 years). Increases in the percent with a duration of <1 year suggests strong recruitment, while increases in the percent with a duration of ≥5 years suggests strong retention. We used R (R-4.2.2 - Vienna, Austria) to analyze data. Simple linear regression created a linear relationship that was analyzed using Pearson’s correlation test to detect longitudinal linear trends among the proportion of survey respondents based on combinations of gender, race/ethnicity, and duration across time.
Clerkship Director Recruitment and Retainment
We analyzed 12 CERA FM clerkship director surveys with response rates ranging from 49%–86%. Our analysis did not identify significant gender-based trends among CDs with duration <1 year (Supplemental Figure 1A) nor duration ≥5 years (Supplemental Figure 1B). We also did not observe significant trends based on BIPOC representation among CDs with duration <1 year (Supplemental Figure 2A). We identified a significant increase in BIPOC representation among CDs with duration ≥5 years, increasing from 9.5% (4/42) in 2012 to 33.3% (19/57) in 2023 (Supplemental Figure 2B; R2 = 0.682, P<0.001).
We examined intersectional trends by race/ethnicity and gender. Our analysis did not reveal significant changes among white male or white female CDs with duration <1 year (Figure 1A) nor duration ≥5 years (Figure 1B). Among BIPOC male and female CDs with duration <1 year, we did not find significant trends. In contrast, we observed significant increases among BIPOC CDs with duration ≥5 years: BIPOC male representation rose from 4.8% (2/42) in 2012 to 19.3% (11/57) in 2023 (R2 = 0.558, P=0.005), and BIPOC female representation increased from 4.8% (2/42) in 2012 to 14.0% (8/57) in 2023 (R2 = 0.511, P=0.009).
Program Director Recruitment and Retainment
We analyzed 22 CERA FM program director surveys, with response rates ranging from 41%–61%. We did not identify significant gender-based trends among PDs with duration <1 year (Supplemental Figure 3A) nor duration ≥5 years (Supplemental Figure 3B). We also did not observe significant trends based on BIPOC representation among PDs with duration <1 year (Supplemental Figure 4A). We found a significant increase in BIPOC representation among PDs with duration ≥5 years, rising from 17.6% (28/159) in 2018 to 29.5% (46/156) in 2023 (Supplemental Figure 4B; R2 = 0.831, P=0.011).
We did not detect significant trends among white male and white female PDs with duration <1 year (Figure 2A) nor duration ≥5 years (Figure 2B). We did not observe significant trends among BIPOC male and female PDs with duration <1 year. We found no significant trends for BIPOC male PDs with duration ≥5 years, however, BIPOC female PDs with duration ≥5 years showed a significant increase in representation, rising from 4.4% (7/159) in 2018 to 17.3% (27/156) in 2023 (R2 = 0.942, P=0.001).
Department Chair Recruitment and Retainment
We analyzed four CERA FM department chair surveys, with response rates ranging from 48%–54%. Our analysis did not identify significant gender-based or BIPOC-related trends among DCs with duration <1 year (Supplemental Figure 5A and 6A) nor duration ≥5 years (SupplementalFigure 5B and 6B).
We did not observe significant changes among white male DCs with duration <1 year (Figure 3A). White female DCs with duration <1 year showed a significant decrease in representation, declining from 26.3% (15/57) in 201921.4% (12/46) in 2023 (R2 = 0.953, P=0.012). We did not identify significant trends among white male or female DCs with duration ≥5 years (Figure 3B), nor among BIPOC male or female DCs with duration <1 year and duration ≥5 years.
Previous research has showed shifts in gender and racial/ethnic representation among family medicine CDs, PDs, and DCs.7-10 Our analysis shows increases in BIPOC representation among BIPOC men and women CDs with duration ≥5 years and BIPOC women PD with duration ≥5 years. These trends indicate stronger retainment of BIPOC leaders, especially BIPOC women, over the past decade without parallel increases in recruitment into leadership positions based on the lack of trends in representation of CDs, PDs, and DCs with duration <1 year. The results reveal temporal patterns but cannot identify which departmental actions caused these retention gains. Departments may have improved retention through formal mentorship and sponsorship,15-18 leadership development,15,17,19 protected administrative time20, compensation adjustments19,20, service equity19,and greater visibility of BIPOC leaders.15,18
Faculty turnover remains substantial and disproportionately affects BIPOC clinicians, which magnifies the importance of retention strategies.4,5,21 BIPOC faculty face barriers such as lower promotion rates, limited access to grant funding, and disproportionate non-clinical responsibilities.6,15,16,17,21 Retaining BIPOC and female academic leaders requires significant departmental effort. Departments could create and promote official pathway programs for academic leaders.16 Departments with BIPOC leaders have greater opportunity for mentorship of individuals from similar backgrounds, which can strengthen the pathway to leadership and improve retention across all career fields.16
One limitation of this study is reliance on CERA survey data. These surveys had variable response rates which have previously been disclosed.7 Additionally, we cannot infer specific causal mechanisms from the CERA data. Other limitations include inconsistencies in demographic data collection across survey years, with variations in race/ethnicity and gender reporting. Most recruitment studies focus on filling down-stream positions (medical students, residents, and clinical faculty) which may indicate a lag in our data focused instead on up-stream leadership positions.15
Retention gains are encouraging but incomplete; departments must maintain effective retention practices while implementing standardized, data-driven recruitment pathways to sustain and expand leadership diversity.
The authors of this manuscript have no conflicts to disclose.
These data were collected as part of multiple surveys conducted by the CAFM Educational Research Alliance (CERA). These projects were approved by the American Academy of Family Physician’s Institutional Review Board.
References
-
Stanford FC. The importance of diversity and inclusion in the healthcare workforce.
J Natl Med Assoc. 2020;112(3):247–249. doi:10.1016/j.jnma.2020.03.014
-
Swartz TH, Palermo A-GS, Masur SK, Aberg JA. The science and value of diversity: closing the gaps in our understanding of inclusion and diversity.
J Infect Dis. 2019;220(220 Suppl 2):S33–S41. doi:10.1093/infdis/jiz174
-
Soklaridis S, Lin E, Black G, et al. Moving beyond “think leadership, think white male”: the contents and contexts of equity, diversity and inclusion in physician leadership programmes.
BMJ Lead. 2022;6(2):146–157. doi:10.1136/leader-2021-000542
-
-
Clark L, Shergina E, Machado N, et al. Race and ethnicity, gender, and promotion of physicians in academic medicine.
JAMA Netw Open. 2024;7(11). doi:10.1001/jamanetworkopen.2024.46018
-
-
Ringwald BA, Edwards Y, Vengal S, Montemayor J, Ringwald C. the changing faces of academic family medicine leadership: a CERA secondary analysis.
Fam Med. 2025;57(3):201–207. doi:10.22454/FamMed.2025.804452
-
Xierali IM, Nivet MA, Rayburn WF. Diversity of department chairs in family medicine at US Medical Schools.
J Am Board Fam Med. 2022;35(1):152–157. doi:10.3122/jabfm.2022.01.210298
-
Adetoye M, Gold K. Race and gender disparities among leadership in academic family medicine.
J Am Board Fam Med. 2022. doi:10.3122/jabfm.2022.AP.220122
-
Weidner A, Clements DS. Cafm leadership demographics.
Ann Fam Med. 2021;19(2):181–185. doi:10.1370/afm.2678
-
Seehusen DA, Mainous AG III, Chessman AW. Creating a Centralized Infrastructure to Facilitate Medical Education Research.
Ann Fam Med. 2018;16(3):257–260. doi:10.1370/afm.2228
-
Kost A, Moore MA, Ho T, Biggs R. Protocol for the 2023 CERA Clerkship Director Survey.
PRiMER. 2023;7(30). doi:10.22454/PRiMER.2023.238868
-
Mainous AG 3rd, Seehusen D, Shokar N. CAFM Educational Research Alliance (CERA) 2011 Residency Director survey: background, methods, and respondent characteristics. Fam Med. 2012;44(10):691–693.
-
-
Rodriguez JE, Campbell KM, Fogarty JP, Williams RL. Underrepresented minority faculty in academic medicine: a systematic review of URM faculty development. Fam Med. 2014;46(2):100–104.
-
Beech BM, Calles-Escandon J, Hairston KG, Langdon SE, Latham-Sadler BA, Bell RA. Mentoring programs for underrepresented minority faculty in academic medical centers: a systematic review of the literature.
Acad Med. 2013;88(4):541–549. doi:10.1097/ACM.0b013e31828589e3
-
Ries A, Wingard D, Morgan C, Farrell E, Letter S, Reznik V. Retention of junior faculty in academic medicine at the University of California, San Diego.
Acad Med. 2009;84(1):37–41. doi:10.1097/ACM.0b013e3181901174
-
Childs E, Yoloye K, Bhasin RM, Benjamin EJ, Assoumou SA. Retaining faculty from underrepresented groups in academic medicine: results from a needs assessment.
South Med J. 2023;116(2):157–161. doi:10.14423/SMJ.0000000000001510
-
Settles IH, Linderman JJ, Rivas-Drake D, Saville J, Conner S. Three strategies for engaging campus leaders in transformative initiatives to retain faculty of color.
Journal of Diversity in Higher Education. 2025;18(3):363–368. doi:10.1037/dhe0000511
-
Rodríguez JE, Campbell KM, Mouratidis RW. Where are the rest of us? Improving representation of minority faculty in academic medicine.
South Med J. 2014;107(12):739–744. doi:10.14423/SMJ.0000000000000204
-
Price EG, Gozu A, Kern DE, et al. The role of cultural diversity climate in recruitment, promotion, and retention of faculty in academic medicine.
J Gen Intern Med. 2005;20(7):565–571. doi:10.1111/j.1525-1497.2005.0127.x



There are no comments for this article.