Background and Objectives: The Accreditation Council of Graduate Medical Education endorses inclusion of patient feedback in performance evaluations during residency training.
Methods: A Council of Academic Family Medicine Educational Research Alliance survey was distributed in spring 2025 to program directors (PDs) at family medicine (FM) residencies, with 321/726 (44.2%) responding. PDs were asked about perceptions and implementation of patient feedback in residency training.
Results: The majority of PDs agree incorporating patient feedback into residency training prepares residents for independent practice (92.5%), improves residents’ morale (64.4%), quality of care (61.7%), and communication skills (69.5%), with 68.8% of programs providing written patient feedback to residents twice yearly or greater, and 65.4% of programs providing verbal coaching on patient feedback twice yearly or greater. However, 37.4% of programs implement residency curricula and 33.0% of programs provide faculty development on patient feedback. PDs from programs providing patient feedback curricula are more likely to view this feedback as improving resident morale, quality of care, and communication with patients (P=0.005, P=0.002, P=0.003), with a similar pattern seen among PDs from programs with faculty development on coaching residents about patient feedback. Increased frequency of coaching residents was positively correlated with PD agreement that patient feedback is valuable for improving residents’ morale, quality of care, patient communication, and preparation for independent practice.
Conclusions: Although PDs value patient feedback, there are gaps with implementing patient feedback into residency training, and an opportunity exists to better prepare family medicine residents for future independent practice.
Patient feedback and patient satisfaction surveys are a widespread performance metric of physician practices, regularly used to evaluate quality in healthcare settings.1 Family medicine residency programs are required to provide residents with objective performance evaluations and progress along formative milestones, incorporating feedback from patients.2,3 The 2025 Accreditation Council of Graduate Medical Education (ACGME) Program Requirements for Graduate Medical Education in Family Medicine stipulate that “the program must provide an objective performance evaluation” for each resident, and that to accomplish this, the program must “use multiple evaluators (eg, faculty members, peers, patients, self, and other professional staff members).”3 The ACGME requirements further outline that this information must inform a twice-yearly meeting with each resident of their performance and progress.
Residency training presents a timely opportunity to coach residents in receiving and applying patient feedback, and the mechanism of providing patient feedback impacts acceptability and utility. Faculty physicians report that patient feedback is viewed most favorably when delivered through direct discussion.4 In training settings, pediatric residents were more likely to reflect on and learn from patient feedback when accompanied by faculty coaching; key facets included helping residents address emotional responses to feedback, view feedback credibly, frame feedback into a lifelong learning perspective, and develop actionable goals for behavior change.5 Additionally, residents who review patient feedback with a faculty coach are more likely to seek further patient feedback than residents who reviewed patient feedback on their own.6 When patient feedback was incorporated into resident advising sessions, there was greater concordance of resident self-assessment with external evaluations of resident performance, suggesting that feedback from multiple sources, including from patients, can better inform resident self-assessment of competency.7 Residency programs have implemented a variety of strategies to elicit patient feedback and use it to promote reflection and practice change among learners, ranging from direct patient questioning by the provider, to timely written feedback with incentives and recognition.8-10 However, standard and best practices have not been well described across graduate medical education programs, with little guidance in family medicine residency education.
The primary aim of this study was to evaluate the current state of integrating patient feedback into family medicine residency training, examining (1) the frequency and methods used by family medicine residency programs to provide patient feedback to residents, (2) the percentage of programs with resident curricula and/or faculty development in coaching residents on patient feedback, and (3) program directors’ (PDs) perceived barriers to and value of providing patient feedback in resident education.
We hypothesized that PDs at programs providing structured resident curriculum, faculty development on coaching, and more frequent delivery of patient feedback would report greater perceived value of patient feedback on improving resident morale, improving quality of care, improving patient communication, and preparing residents for independent practice than programs without such training. We also sought to examine associations between program size and affiliations with academic medical centers regarding feedback frequency, formal curricula, and faculty development.
Survey
The survey questions were included in the Spring 2025 Council of Academic Family Medicine Educational Research Alliance (CERA) Program Director Survey. The CERA survey is distributed annually to program directors at ACGME-accredited family medicine residency programs. The Spring 2025 CERA survey was approved by the Institutional Review Board of the American Academy of Family Physicians, and was distributed to 726 program directors at eligible programs (those with a graduated resident class), with 321 (44.2%) responding, and the demographics of the sample surveyed represented the pool of potential respondents.11 Survey questions on demographics were developed by the CERA survey administrators. The survey questions on patient feedback were developed by the authors of this paper using an iterative process, resulting in 10 single-response multiple choice or 4-point Likert-scale questions. The outcomes of particular interest were the frequency and methods by which programs provided patient feedback to residents, barriers to providing patient feedback, whether programs provided resident training on receiving and/or faculty development on coaching in regards to patient feedback, and the perceptions of PDs regarding patient feedback in relation to patient care.
Statistical Analyses
We used frequencies (counts and percentages) to describe survey respondent demographics (Table 1) and responses (Table 2). Given that most variables of interest were measured on an ordinal scale with only a small number of response levels, we used rank-based tests for hypothesis testing. We used a two-tailed Mann-Whitney U test to compare independent samples of ordinal variables (Figure 1) and Spearman’s rank correlation to evaluate relationships between ordinal variables (Figure 2). For categorical variables with only two levels (ie, binary variables), we used Pearson’s χ2 test to compare proportions between independent samples. P values were rounded to three decimal places, with values less than 0.001 reported as P<0.001. For exploratory analyses involving a family of hypothesis tests, we used the Holm correction to adjust P values for multiple comparisons and control the family-wise error rate. We selected the Holm method because it provides stronger control of type I error than unadjusted testing while being less conservative than the Bonferroni correction. Statistical significance was defined as α = 0.05. All statistical analyses were performed with R version 4.5.1 (R Foundation).
|
(N = 321)
n (%) |
Program director’s race |
American Indian/Alaska Native/Indigenous |
1 (0.3) |
Asian |
26 (8.1) |
Black/African American |
14 (4.4) |
Hispanic/Latino/of Spanish Origin |
15 (4.7) |
Middle Eastern/North African |
2 (0.6) |
Native Hawaiian/other Pacific Islander |
0 |
White |
233 (72.6) |
Choose not to disclose |
14 (4.4) |
Multiraciala |
15 (4.7) |
Unknown |
1 (0.3) |
Program director’s gender |
Female/woman |
183 (57.0) |
Male/man |
135 (42.1) |
Genderqueer/gender nonconforming |
0 |
Nonbinary |
0 |
Choose not to disclose |
2 (0.6) |
Self-described |
0 |
Unknown |
1 (0.3) |
Program type |
University-based |
51 (15.9) |
Community-based (university-affiliated) |
184 (57.3) |
Community-based (nonaffiliated) |
75 (23.4) |
Military |
6 (1.9) |
Other |
5 (1.6) |
Program size (# of residents) |
Small (less than 19) |
137 (42.7) |
Medium (19 to 31) |
136 (42.4) |
Large (greater than 31) |
48 (15.0) |
Unknown |
0 |
Program location |
New England (NH, MA, ME, VT, RI, or CT) |
9 (2.8) |
Middle Atlantic (NY, PA, or NJ) |
45 (14.0) |
South Atlantic (PR, FL, GA, SC, NC, VA, DC, WV, DE, or MD) |
56 (17.4) |
East South Central (KY, TN, MS, or AL) |
15 (4.7) |
East North Central (WI, MI, OH, IN, or IL) |
60 (18.7) |
West South Central (OK, AR, LA, or TX) |
34 (10.6) |
West North Central (ND, MN, SD, IA, NE, KS, or MO) |
26 (8.1) |
Mountain (MT, ID, WY, NV, UT, AZ, CO, or NM) |
26 (8.1) |
Pacific (WA, OR, CA, AK, or HI) |
50 (15.6) |
Community size (# of people in the community associated with the program’s location) |
Less than 30,000 |
39 (12.1) |
30,000 to 75,000 |
53 (16.5) |
75,000 to 150,000 |
62 (19.3) |
150,000 to 500,000 |
74 (23.1) |
500,000 to 1,000,000 |
44 (13.7) |
Greater than 1,000,000 |
46 (14.3) |
Unknown |
3 (0.9) |
|
(N = 321)
n (%) |
1. How often does your residency program typically provide each resident with a written summary of their patient feedback evaluations? |
Weekly |
5 (1.6) |
Monthly |
43 (13.4) |
Quarterly |
91 (28.3) |
Twice a year |
82 (25.5) |
Yearly |
32 (10.0) |
We do not routinely provide residents with this information. |
63 (19.6) |
No response |
5 (1.6) |
2. In what setting are patient feedback evaluations primarily discussed with residents? (choose the most applicable) |
As part of regular advisor meetings with the resident |
113 (35.2) |
As part of the regular milestones assessment process |
82 (25.5) |
Following the receipt of exceptional feedback (either concerning/negative or positive) |
60 (18.7) |
As part of an annual review meeting |
21 (6.5) |
We do not routinely discuss patient feedback evaluations with residents. |
41 (12.8) |
No response |
4 (1.2) |
3. What is the primary curricular method used to teach residents about reviewing, analyzing, and integrating patient feedback evaluations? (choose the most applicable) |
Lecture/didactic |
46 (14.3) |
Group discussion |
60 (18.7) |
Seminar or workshop |
7 (2.2) |
Provision of self-study reading material (inclusive of online modules) |
7 (2.2) |
No formal curriculum |
197 (61.4) |
No response |
4 (1.2) |
4. How often do residents typically receive individual discussion and coaching from any faculty member (inclusive of the program director) regarding patient feedback evaluations? |
Weekly |
9 (2.8) |
Monthly |
12 (3.7) |
Quarterly |
88 (27.4) |
Twice a year |
101 (31.5) |
Yearly |
28 (8.7) |
We do not routinely discuss patient feedback evaluations with residents. |
78 (24.3) |
No response |
5 (1.6) |
5. Does your program provide formal faculty development (eg, lectures, group discussions, seminars or workshops, online modules, or other continuing education) to prepare faculty to coach residents on patient feedback evaluations? |
No |
208 (64.8) |
Yes |
106 (33.0) |
No response |
7 (2.2) |
6. What is your program’s main challenge to discussing patient feedback evaluations with residents? (choose the most applicable) |
Data issues (inclusive of difficulty obtaining patient feedback, collating, organizing, or distributing data) |
160 (49.8) |
Lack of faculty time |
44 (13.7) |
Insufficient faculty training on discussing patient feedback with residents |
14 (4.4) |
Difficulty coordinating a meeting time between faculty and resident |
36 (11.2) |
Resident objection or pushback to receiving patient feedback |
5 (1.6) |
There are no challenges. |
37 (11.5) |
We do not routinely discuss patient feedback evaluations with residents. |
21 (6.5) |
No response |
4 (1.2) |
7. Patient feedback evaluations have helped improve our residents’ morale when providing care to patients. |
Strongly agree |
21 (6.5) |
Agree |
186 (57.9) |
Disagree |
91 (28.3) |
Strongly disagree |
10 (3.1) |
No response |
13 (4.0) |
8. Patient feedback evaluations have helped our residents improve the quality of care that they provide to patients. |
Strongly agree |
18 (5.6) |
Agree |
180 (56.1) |
Disagree |
103 (32.1) |
Strongly disagree |
7 (2.2) |
No response |
13 (4.0) |
9. Patient feedback evaluations have helped our residents improve their interactions and communication skills with patients. |
Strongly agree |
17 (5.3) |
Agree |
206 (64.2) |
Disagree |
79 (24.6) |
Strongly disagree |
6 (1.9) |
No response |
13 (4.0) |
10. It is valuable for our residents to receive patient feedback evaluations in preparation for independent practice. |
Strongly agree |
107 (33.3) |
Agree |
190 (59.2) |
Disagree |
12 (3.7) |
Strongly disagree |
3 (0.9) |
No response |
9 (2.8) |
Demographics
The majority of PDs responding to the Spring 2025 CERA Program Director Survey were community-based with university affiliation (57.3%), followed by community-based (23.4%), then university-based (15.9%), military (1.9%), and other (1.6%). Program sizes were categorized as either small (42.7%, less than 19 residents), medium (42.4%, 19 to 31 residents), or large (15%, greater than 31 residents). Programs were varied in terms of geographic location and community size (Table 1).
Survey Results
The majority (92.5%) of responding PDs agree/strongly agree that incorporating patient feedback into residency training is important preparation for independent practice, and the majority of responding PDs agree/strongly agree that patient feedback improves residents’ morale (64.4%), quality of care provided by residents (61.7%), and residents’ communication skills (69.5%, Table 2).
We found that 37.4% of programs have a formal curriculum to teach residents about receiving and applying patient feedback. Of programs providing this education, group discussion or lecture/didactic were the most common teaching modalities. Additionally, 33.0% of programs have formal faculty development on coaching residents on receiving and integrating patient feedback (Table 2).
Written Patient Feedback Frequency
It was determined that 68.8% of programs provide a written summary of patient feedback to residents twice yearly or greater, with most programs providing this information either quarterly (28.3%) or biannually (25.5%). Notably, 19.6% of programs do not routinely provide written patient feedback to residents (Table 2).
Resident Coaching/discussion Frequency
We identified that 65.4% of programs provide discussion/coaching on patient feedback to residents with twice yearly or greater frequency, most often during an advisor meeting (35.2%) or as part of the milestones assessment process (25.5%). In 18.7% of programs, patient feedback discussions primarily occur following receiving either markedly positive or concerning feedback, and in 12.8% of programs, patient feedback is not routinely discussed with residents (Table 2).
Barriers to Resident Coaching/discussion
The main challenges to providing coaching or discussion of patient feedback with residents were: difficulty with obtaining/distributing patient feedback data (49.8%), lack of faculty time (13.7%), difficulty coordinating meeting times between a faculty and resident (11.2%), insufficient faculty training (4.4%), and resident objection or “push-back” to receiving patient feedback (1.6%). A minority of PDs do not report challenges (11.5%) with discussing patient feedback (Table 2).
Resident Curriculum or Faculty Development in Relation to Perceived Value of Patient Feedback
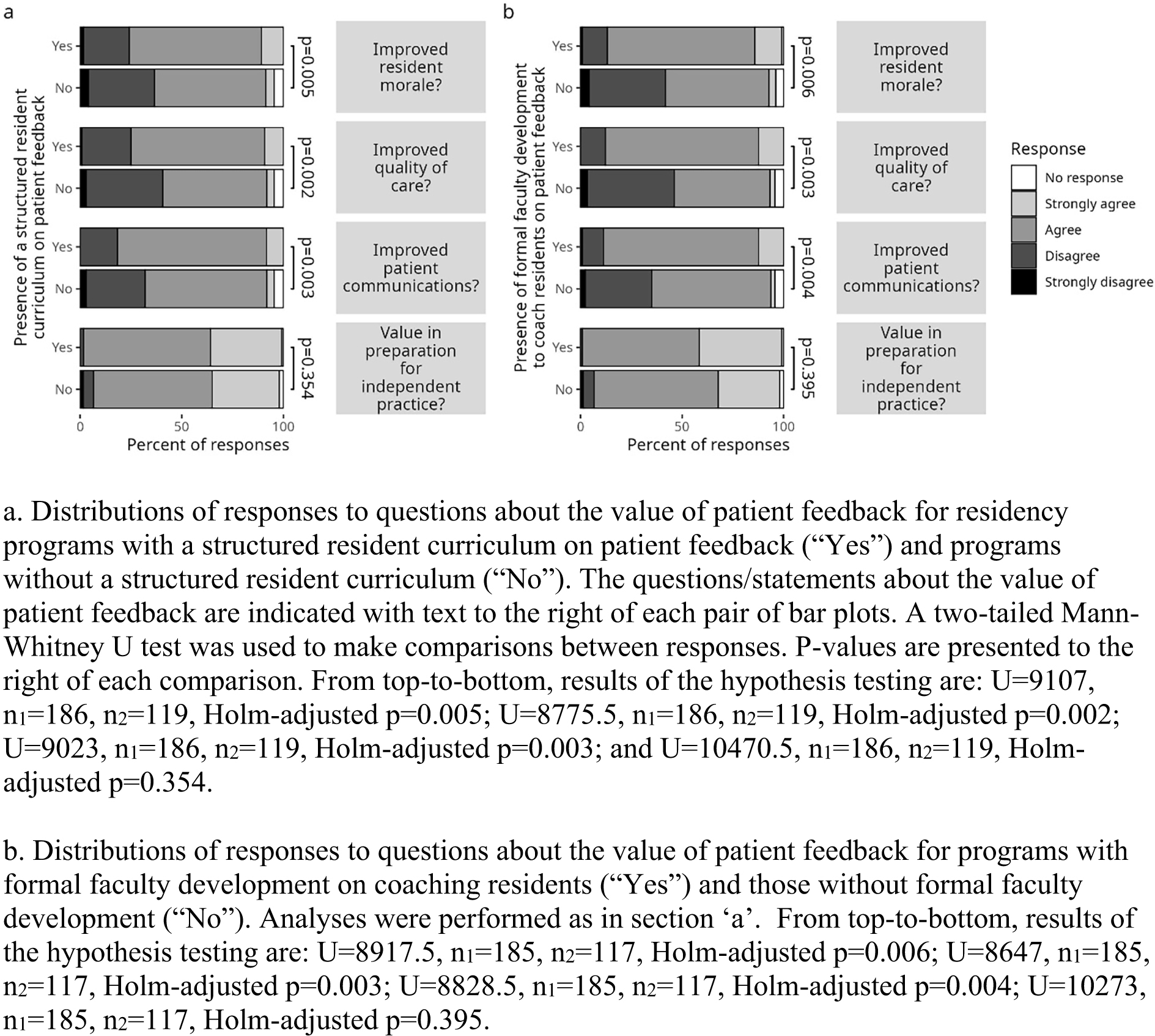
PDs from programs with patient feedback curricula for residents expressed significantly stronger agreement that patient feedback improves resident morale (Figure 1a, two-tailed Mann-Whitney U test, U = 9,107, n1 = 186, n2 = 119, Holm-adjusted P=0.005), quality of care (Figure 1a, two-tailed Mann-Whitney U test, U = 8,775.5, n1 = 186, n2 = 119, Holm-adjusted P=0.002), and communication/interactions with patients (Figure 1a, two-tailed Mann-Whitney U test, U = 9,023, n1 = 186, n2 = 119, Holm-adjusted P=0.003). The majority of PDs agreed that patient feedback is important for preparing residents for independent practice, with no significant difference between PDs with or without resident curricula (Figure 1a, two-tailed Mann-Whitney U test, U = 10,470.5, n1 = 186, n2 = 119, Holm-adjusted P=0.354).
Similarly, PDs from programs with faculty development on coaching residents on patient feedback expressed significantly stronger agreement that patient feedback was valuable for improving resident morale (Figure 1b, two-tailed Mann-Whitney U test, U = 8,917.5, n1 = 185, n2 = 117, Holm-adjusted P=0.006), quality of care (Figure 1b, two-tailed Mann-Whitney U test, U = 8,647, n1 = 185, n2 = 117, Holm-adjusted P=0.003), and communications/interactions with patients (Figure 1b, two-tailed Mann-Whitney U test, U = 8,828.5, n1 = 185, n2 = 117, Holm-adjusted P=0.004). The majority of PDs viewed patient feedback as important for independent practice, regardless of the presence of faculty development or not (Figure 1b, two-tailed Mann-Whitney U test, U = 10,273, n1 = 185, n2 = 117, Holm-adjusted P=0.395).
Frequency of Discussion/coaching in Relation to Perceived Value of Patient Feedback
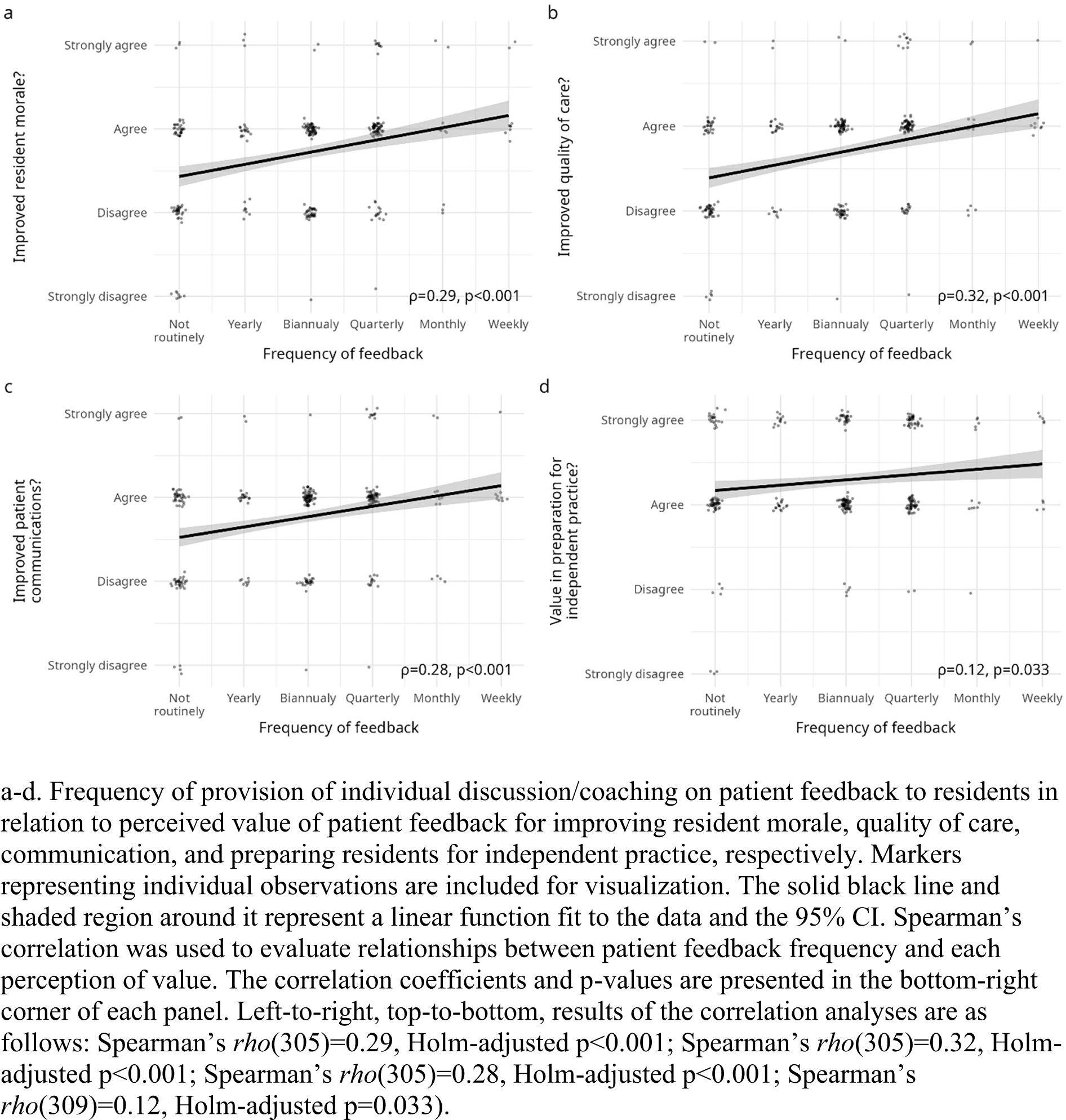
Frequency of discussion/coaching residents on patient feedback was weakly positively correlated with PD agreement that patient feedback is valuable for improving residents’ morale, quality of care, and patient interactions/communication (Figure 2a-c, Spearman’s ρ(305)=0.29, Holm-adjusted P<0.001, Spearman’s ρ(305)=0.32, Holm-adjusted P<0.001, Spearman’s ρ(305)=0.28, Holm-adjusted P<0.001, respectively), and very weakly positively correlated with value in preparation for independent practice (Figure 2d, Spearman’s ρ(309)=0.12, Holm-adjusted P=0.033).
Patient Feedback Frequency, Curricula, and Faculty Development in Relation to Program Size and Type
We refactored the three levels of program size (small, medium, and large) from CERA into two levels: small (<19 residents) and large (≥19 residents) programs, for comparison and analysis. We also sorted programs into types based on affiliation: university-affiliated vs non-university-affiliated. Using these dichotomies to describe residency programs, we found that there was no association between program size and frequency of provision of written patient feedback to residents (data not shown, two-tailed Mann-Whitney U test, U = 11,517, n1 = 137, n2 = 184, Holm-adjusted P=1.0). There was also no association between program size and frequency of faculty coaching to residents about patient feedback (data not shown, two-tailed Mann-Whitney U test, U = 10,577.5, n1 = 137, n2 = 184, Holm-adjusted P=0.137).
Additionally, program size was unrelated to the provision of a formal resident curriculum (data not shown, χ2 [1, n = 317] = 0.315, Holm-adjusted P=1.0) as well as faculty development on patient feedback (data not shown, χ2 [1, n = 317] = 0.0, Holm-adjusted P=1.0).
Neither the frequency of provision of written patient feedback, frequency of faculty coaching, presence of a formal resident curriculum, nor presence of faculty development depended on the type of program (university-based/affiliated vs non-university-based/affiliated, data not shown, all Holm-adjusted P values>0.05).
Principal Findings
In this descriptive cross-sectional quantitative survey study, we found that the majority of responding PDs had favorable views on incorporating patient feedback in residency education, with perceptions that sharing patient feedback with residents led to better resident morale, higher quality of care, and improved patient communication. Specifically, we found that PDs who agree that sharing patient feedback is beneficial were more likely to provide formal resident training on receiving patient feedback, faculty development on coaching residents about patient feedback, and more frequent discussion with residents on patient feedback.
The vast majority of PDs (93%) agreed that patient feedback is important in preparing family medicine residents for independent practice, yet many programs are falling short in educating their residents on patient feedback. Relatively few programs provide residency curricula or faculty development on coaching residents regarding patient feedback, and some do not routinely provide patient feedback at all.
Although we had hypothesized that the larger or university-based/affiliated programs would have more resources to support patient feedback implementation, there was no difference in delivering resident curriculum or faculty development on patient feedback, or providing residents with written patient feedback or coaching/discussion on patient feedback. Barriers to providing coaching/discussion were mainly systemic, with nearly half of programs identifying difficulty with obtaining and distributing patient feedback as the key issue. Time barriers (faculty time, coordination of meeting time) were another notable, although less frequent, challenge.
There is a marked discrepancy between PD recognition of the importance of patient feedback in provision of patient care and preparing residents for independent practice, and the actions of residency programs to educate residents in this area.
Relevance of Findings
Medicine is increasingly focused on patient experience. Online reviews are highly prevalent, including healthcare systems reporting individual physician results online.12 Eighty-four percent of patients read online reviews before choosing a new health care provider.13 Patient satisfaction surveys14,15 are widely utilized in healthcare systems to increase transparency, improve patient care, and inform hospital reimbursements. Physician employers may utilize patient satisfaction surveys to measure physician performance and impact financial compensation.16 Unsatisfactory patient reviews can lead to negative job satisfaction, physician burnout, and the decision to leave their job or medicine altogether.16,17 The pressure to attain higher patient satisfaction scores may influence physician medical decision-making, including the prescribing of antibiotics, prescribing opioid medications, performing procedures, and ordering imaging and tests.17
Residency is an optimal time to teach physicians to thoughtfully incorporate patient feedback and cultivate skills to improve patient experience.18 Interestingly, clinical knowledge and years of experience may not translate into positive patient feedback,19-22 whereas empathy and effective communication improve patient satisfaction scores.19,23
Though most PDs agree that preparation for future practice should include patient feedback, underscored by ACGME guidance, many programs are not meeting this goal. Given that effective data collection/distribution, faculty time availability, and coordination of meeting time were top barriers to providing patient feedback, interventions that focus on these areas may be of benefit. Additionally, there is the potential to add in both residency curricula and faculty development on patient feedback in many residency programs.
Limitations
Limitations of this study include only evaluating family medicine residency programs through PD report. Additionally, the results were based on PD perceptions and do not include resident, faculty or alumni perceptions. The study is also limited by a low response rate, which may introduce bias, however, the rate is in line with response rates from prior CERA studies, and comparing potential to actual respondents supports sample representativeness.11
Conclusions and Next Steps
Although PDs value patient feedback, there is a gap in implementing patient feedback in residency education, with some programs not providing this feedback routinely, and the majority of programs lacking resident curricula or faculty development around patient feedback. Family medicine residency programs have an opportunity to prepare family medicine residents for future independent practice by incorporating intentional and structured patient feedback into residency training.
Coaching Residents Following Patient Feedback Evaluations: Implications From a CERA Study. Presented at the 2026 Society of Teachers of Family Medicine Annual Spring Conference, May 2–6, 2026, New Orleans, Louisianna
References
-
Wong E, Mavondo F, Fisher J. Patient feedback to improve quality of patient-centred care in public hospitals: a systematic review of the evidence.
BMC Health Serv Res. 2020;20(1):530. doi:10.1186/s12913-020-05383-3
-
-
-
Vilendrer SM, Kling SMR, Wang H, et al. How feedback is given matters: a cross-sectional survey of patient satisfaction feedback delivery and physician well-being.
Mayo Clin Proc. 2021;96(10):2615–2627. doi:10.1016/j.mayocp.2021.03.039
-
Bogetz AL, Orlov N, Blankenburg R, Bhavaraju V, McQueen A, Rassbach C. How residents learn from patient feedback: a multi-institutional qualitative study of pediatrics residents’ perspectives.
J Grad Med Educ. 2018;10(2):176–184. doi:10.4300/JGME-D-17-00447.1
-
Rassbach CE, Bogetz AL, Orlov N, et al. The effect of faculty coaching on resident attitudes, confidence, and patient-rated communication: a multi-institutional randomized controlled trial.
Acad Pediatr. 2019;19(2):186–194. doi:10.1016/j.acap.2018.10.004
-
Keister DM, Hansen SE, Dostal J. Teaching resident self-assessment through triangulation of faculty and patient feedback.
Teach Learn Med. 2017;29(1):25–30. doi:10.1080/10401334.2016.1246249
-
David D, McAfee SG, Eth S. The impact of patient feedback on psychotherapy and supervision outcomes in psychiatry residency.
Acad Psychiatry. 2023;47(5):546–549. doi:10.1007/s40596-022-01638-9
-
Banka G, Edgington S, Kyulo N, et al. Improving patient satisfaction through physician education, feedback, and incentives.
J Hosp Med. 2015;10(8):497–502. doi:10.1002/jhm.2373
-
O’Leary KJ, Cyrus RM. Improving patient satisfaction: timely feedback to specific physicians is essential for success.
J Hosp Med. 2015;10(8):555–556. doi:10.1002/jhm.2403
-
Reedy-Cooper A, Ho T, Moore MA. Protocol for the spring 2025 CERA program director survey.
PRiMER. 2025;9:45. doi:10.22454/PRiMER.2025.639725
-
Wickner PG, Dankers C, Green M, Salmasian H, Kachalia A. Early performance trends after the public posting of ambulatory patient satisfaction reviews.
J Patient Exp. 2019;6(4):329–332. doi:10.1177/2374373519833649
-
-
Giordano LA, Elliott MN, Goldstein E, Lehrman WG, Spencer PA. Development, implementation, and public reporting of the HCAHPS survey.
Med Care Res Rev. 2010;67(1):27–37. doi:10.1177/1077558709341065
-
-
Schneider BJ, Ehsanian R, Schmidt A, et al. The effect of patient satisfaction scores on physician job satisfaction and burnout.
Future Sci OA. 2020;7(1):FSO657. doi:10.2144/fsoa-2020-0136
-
Zgierska A, Rabago D, Miller MM. Impact of patient satisfaction ratings on physicians and clinical care.
Patient Prefer Adherence. 2014;8:437–446. doi:10.2147/PPA.S59077
-
-
Ali K, Shayne P, Ross M, Franks N. Evaluation of the patient satisfaction performance of emergency medicine resident physicians in a large urban academic emergency department.
Annals of Emergency Medicine. 2013;62(4):S139. doi:10.1016/j.annemergmed.2013.07.215
-
Walker LE, Colletti JE, Bellolio MF, Nestler DM. Progression of emergency medicine resident patient experience scores by level of training.
J Patient Exp. 2019;6(3):210–215. doi:10.1177/2374373518798098
-
Lang SC, Weygandt PL, Darling T, et al. Measuring the correlation between emergency medicine resident and attending physician patient satisfaction scores using Press Ganey.
AEM Educ Train. 2017;1(3):179–184. doi:10.1002/aet2.10039
-
Allenbaugh J, Corbelli J, Rack L, Rubio D, Spagnoletti C. A brief communication curriculum improves resident and nurse communication skills and patient satisfaction.
J Gen Intern Med. 2019;34(7):1167–1173. doi:10.1007/s11606-019-04951-6
-
Aqeel A, Haider T, Sanaullah O, Pamula J. Improving patient satisfaction scores of resident-run services in inpatient settings.
Chest. 2021;160(4):A1415. doi:10.1016/j.chest.2021.07.1294



There are no comments for this article.