Background and Objectives: Despite highly effective therapies for the hepatitis C virus (HCV), treatment rates remain low. Management of HCV is shifting to primary care, and family physicians are positioned to provide this care. Our objective was to determine the extent of early-career family physicians’ provision of HCV treatment.
Methods: We merged 2016–2023 data from the American Board of Family Medicine National Graduate Survey, which is administered 3 years after completing residency, with state-level HCV mortality data from the Centers for Disease Control and Prevention (2017–2021). We conducted bivariate analyses to examine differences in HCV treatment by physician characteristics, practice type, and practice location. We created maps to visually explore HCV treatment and mortality by state.
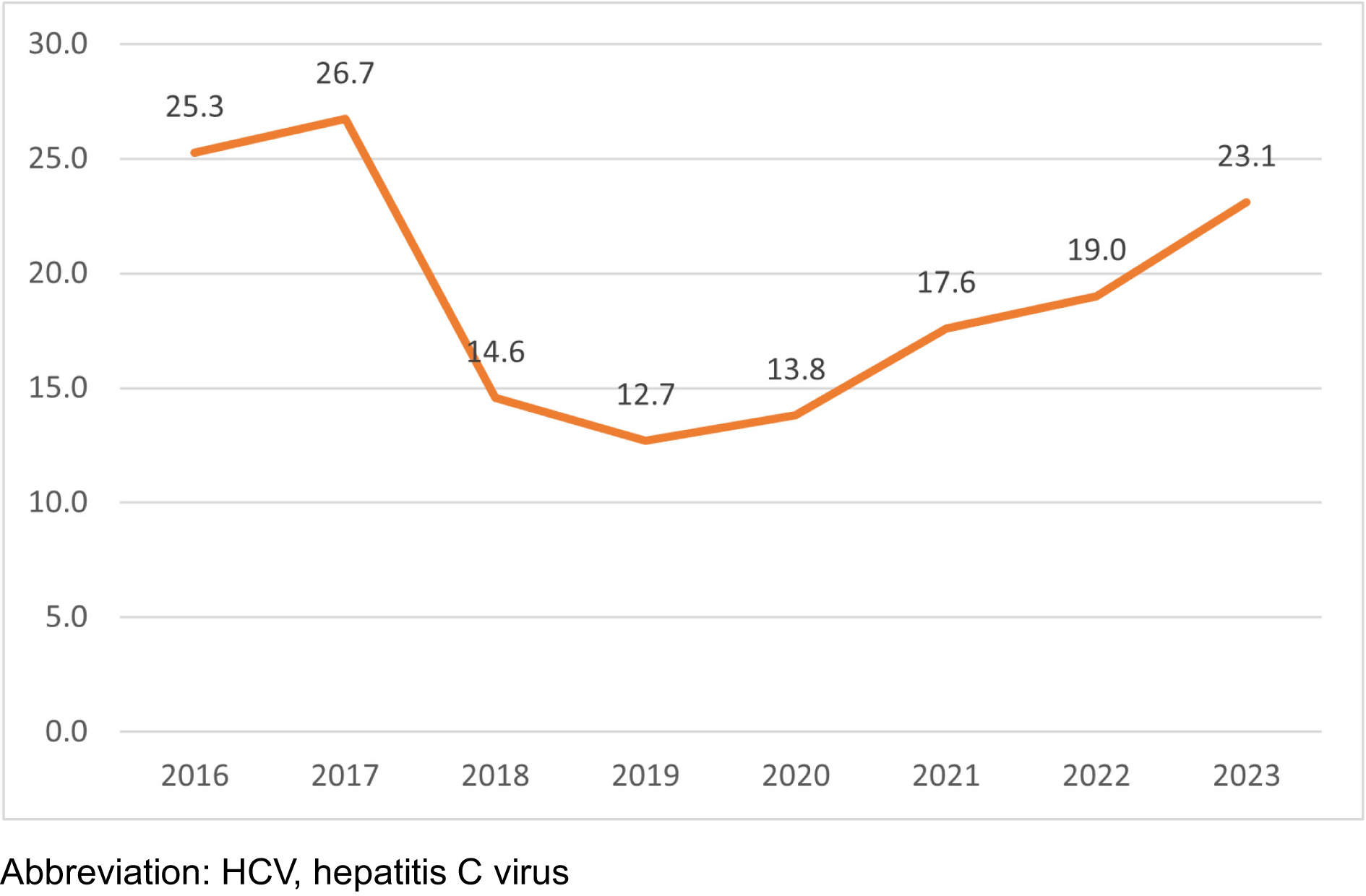
Results: Overall, less than 20% of early-career family physicians reported treating HCV patients. Early-career family physicians HCV treatment rates exceeded 25% in 2016 and 2017, with rates falling to below 15% from 2018 to 2020, before rebounding to 23% in 2023. Early-career family physicians who were males, had MDs (compared to DOs), were international medical graduates, and were in nonmetropolitan areas and in medically underserved area practice types had significantly higher HCV treatment rates. State-level variation was observed, with higher early-career HCV treatment rates in states with higher HCV mortality.
Conclusions: While HCV treatment has been simplified over the past decade, HCV treatment by early-career family physicians has declined. Despite this decline, early-career family physicians have higher rates of HCV treatment in higher-need areas and in medically underserved practice settings. Supporting family physicians through education, clinical exposure, and incentives may increase provision of HCV care to address unmet needs.
More than 2 million people in the United States have chronic hepatitis C (HCV).1 New annual cases of HCV doubled from 2013 to 2022, particularly among younger populations (ages 18–39), attributed largely to injection drug use.2,3 Populations at the highest risk for HCV include incarcerated populations, which have HCV rates more than 10 times the general population; American Indian/Alaskan Natives, which have the highest incidence rates of HCV; and non-Hispanic Black populations, which have experienced the largest increase in cases over the past few years.2,4 Improving access to treatment is critical, because chronic HCV leads to long-term liver failure, liver cancer, cirrhosis, and eventually premature death.5
Over the last decade, the development of direct-acting antiviral therapies has greatly improved HCV treatment, with cure rates up to 95%.6 However, large numbers of HCV patients are not being treated.7-9 Focusing on privately and publicly insured adults, Thompson et al reported that only about one-third initiated treatment within a year of diagnosis,8 and some recent reports have suggested postpandemic reversals of gains in testing and treatment.9 Tsang et al reported similar findings using 10 years of data from a commercial laboratory, finding that about 35% of patients with initial infection were cured, with cure rates ranging widely across US states.7 These low HCV treatment rates can be attributed to several factors, including high costs, stigma, and state-level Medicaid policies, which have changed dramatically over the past decade and vary significantly across states.10-12
The Infectious Diseases Society of America explicitly called for increasing the number of primary care clinicians providing HCV treatment as critical to improving access to care.13 Several studies have demonstrated the effectiveness of HCV treatment delivered by primary care physicians.14,15 In a study of a high-risk population in a federally qualified health center, Kattakuzhy et al found that HCV treatment by nurse practitioners and primary care physicians was as safe and effective as care provided by HCV specialists.14 In a primary care setting, Stewart et al implemented a population-based improvement intervention that increased HCV treatment rates from 66%–76%.15 Despite these studies and increasing calls for expansion of nonspecialist HCV care to improve access to treatment, research has suggested that many primary care physicians have limited experience with HCV patients and lack the confidence to initiate treatment.11,16,17
Though family physicians are the largest group of primary care physicians, research on family physicians treating HCV patients is limited. A recent study using 2017 to 2021 data found that only 4% of final year resident family physicians intended to treat HCV,18 but no studies have explored family physician engagement in HCV treatment at a national level. The overall objective of our research was to determine temporal and geographic trends in HCV treatment rates for early-career family physicians, while also exploring differences by physician characteristics, practice type, and practice location. We also examined the relationship between HCV treatment rates and HCV mortality at the state level.
In our research, we used self-reported HCV treatment data from the American Board of Family Medicine (ABFM) National Graduate Survey (2016–2023), which is administered to ABFM-certified physicians 3 years after residency graduation (defined as early-career), and state-level HCV mortality data from the Centers for Disease Control and Prevention (CDC, 2017–2021).19,20 We excluded early-career family physicians who did not practice in the United States, who were missing their practice address, or who reported not doing patient care. Also excluded were early-career family physicians who had missing HCV treatment data.
Our primary outcome measure was HCV treatment rates, defined as the percentage of early-career family physicians self-reporting providing the pharmacologic management of HCV.19 Medically underserved area (MUA) practices were defined as early-career family physicians practicing in federally qualified health centers, rural health clinics, Indian Health Service, or correctional facilities. Any other practice type was defined as a non-MUA practice. Metropolitan status was defined based on the US Department of Agriculture rural-urban commuting area codes, which breaks down areas by zip codes according to the following classifications: metro (1–3); micro (4–6); small town (7–9); and rural (10). We defined all areas outside of metro (1–3) as nonmetropolitan (4–10).20
After creating trend lines to explore early-career family physician HCV treatment by year, we conducted t tests to determine differences in HCV treatment by physician characteristics (age, gender, medical degree, graduate location), practice type (MUA vs non-MUA), and practice location (metropolitan vs nonmetropolitan). Because our primary aim was descriptive, we did not use multivariable regression, though future analyses may examine independent associations. Next, data were aggregated to the state level, and we mapped early-career family physician HCV treatment rates for US states by tercile: The top 33rd percentile of states were defined as high-treatment states, while the bottom 33rd percentile were defined as low-treatment states. Finally, we merged state-level HCV mortality data, defined high and low HCV mortality states by tercile, and created a conditional map to explore the relationship between early-career family physician HCV treatment and HCV mortality.
We used Microsoft Excel and GeoDa version 1.22.0.4 (GeoDa Center) to create maps and conduct the analyses. This research was considered exempt by the Institutional Review Board of the American Academy of Family Physicians.
After applying exclusion criteria, our analytic sample included 14,837 early-career family physicians. From 2016 to 2023, about one-fifth of early-career family physicians reported providing HCV treatment, though the percentages varied by year (Figure 1). More than one-fourth of early-career family physicians reported treating HCV patients in 2016 and 2017; this declined to below 15% from 2018 to 2020, then increased back to 23% in 2023.21
Table 1 displays the characteristics of early-career family physicians providing HCV treatment. While females and US medical graduates made up the majority of our sample, males and international medical graduates had significantly higher HCV treatment rates. Also, early-career family physicians with medical degrees (MDs) had significantly higher HCV treatment rates than those with osteopathic degrees (DOs).
|
Early-career family physicians providing HCV treatment n (%) |
All early-career family physicians n (%) |
P value |
Total |
2,817 (19.0) |
14,837 |
|
Degree |
<0.001 |
MD |
2,335 (19.7) |
11,872 (80.0) |
|
DO |
482 (16.3) |
2,965 (20.0) |
|
Gender |
<0.001 |
Female |
1,352 (16.3) |
8,280 (55.9) |
|
Male |
1,456 (22.3) |
6,532 (44.1) |
|
Graduate location |
<0.001 |
International medical graduates |
979 (21.3) |
4,586 (31.0) |
|
US medical graduates |
1,838 (17.9) |
10,251 (69.0) |
|
Practice location |
<0.001 |
Nonmetropolitan |
564 (21.6) |
2,608 (17.6) |
|
Rural |
91 (26.3) |
346 (2.3) |
|
Small town |
191 (21.2) |
900 (6.1) |
|
Micropolitan |
282 (20.7) |
1,362 (9.2) |
|
Metropolitan |
2,253 (18.4) |
12,229 (82.4) |
|
Practice type |
<0.001 |
All MUA practices |
777 (31.8) |
2,443 (16.4) |
|
Indian Health Service |
61 (52.1) |
117 (0.8) |
|
Rural health clinic |
139 (23.6) |
589 (4.0) |
|
Federally qualified health center |
498 (32.1) |
1,553 (10.5) |
|
Government clinic (nonfederal) |
75 (42.1) |
178 (1.2) |
|
All Non-MUA practices |
2,040 (16.5) |
12,394 (83.6) |
|
Academic health center |
333 (21.9) |
1,523 (10.2) |
|
Emergency medicine |
67 (16.5) |
406 (2.7) |
|
Federal |
69 (11.6) |
596 (4.0) |
|
Hospital/health system owned |
641 (13.0) |
4,922 (33.2) |
|
Hospitalist |
393 (29.3) |
1,343 (9.1) |
|
Independently owned medical practice |
270 (16.0) |
1,684 (11.4) |
|
Managed care/HMO practice |
148 (17.2) |
859 (5.8) |
|
Urgent care |
33 (5.5) |
595 (4.0) |
|
Work-site clinic |
36 (20.0) |
178 (1.2) |
|
Early-career family physicians in nonmetropolitan areas have HCV treatment rates significantly higher than early-career family physicians in metropolitan areas. Early-career family physician HCV treatment rates increase as locations get more rural, with those located in rural and small towns having the highest HCV treatment rates. Early-career family physicians in MUA practices have significantly higher HCV treatment rates (31.8%) than those in non-MUA practices (16.5%).
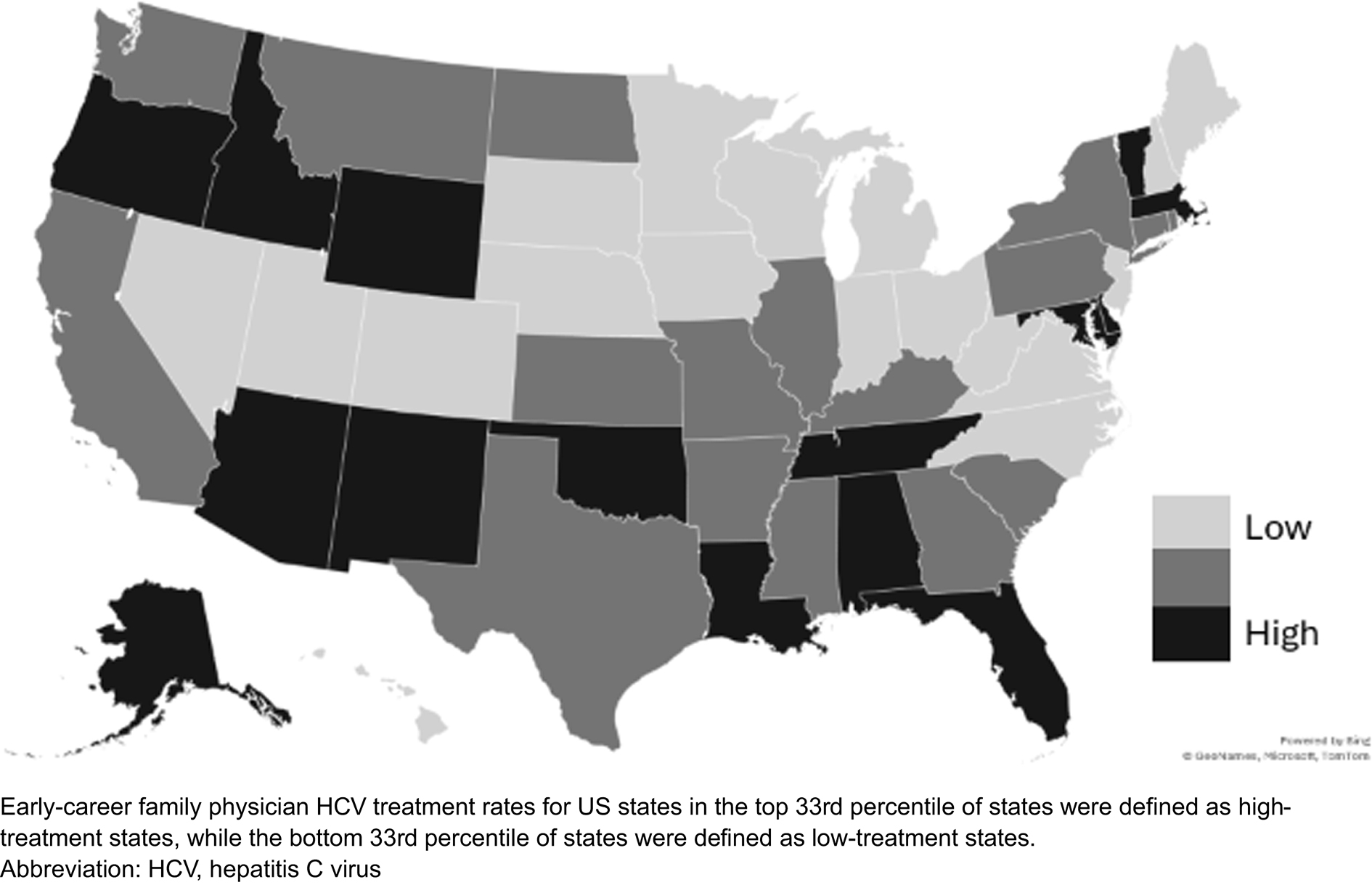
Figure 2 displays state-level geographic variation for early-career family physicians providing HCV treatment. The geographic patterns were clear; more than a dozen states had early-career family physician HCV treatment rates below 17%; these included several states in the Midwest, the Great Plains, Mid-Atlantic, and Mountain West. States with the highest early-career family physician HCV treatment rates (>25%) can be found throughout the United States—including Alaska, Idaho, Oregon, and New Mexico in the west; Alabama, Louisiana, and Florida in the southeast; and Vermont, Delaware, Massachusetts, and District of Columbia in the northeast.
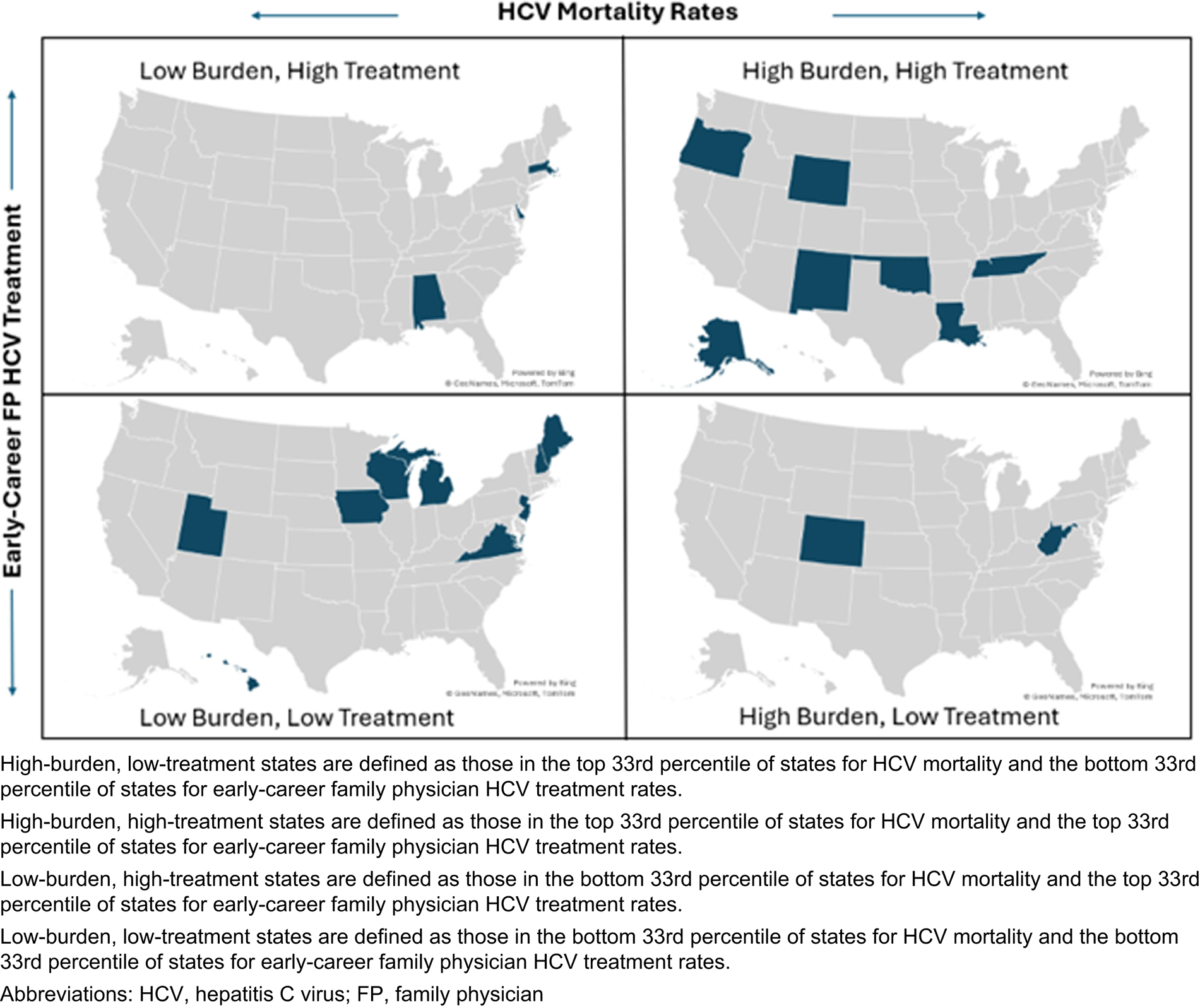
Mapping HCV mortality by the percentage of early-career family physicians providing HCV treatment at the state level revealed geographic patterns (Figure 3). Many states with high HCV mortality also had high rates of early-career family physician HCV treatment, though a few exceptions were identified. Both Colorado and West Virginia had among the highest HCV mortality rates, but relatively low rates of early-career family physician HCV treatment.
These findings highlight significant gaps in both early-career family physician HCV treatment provision and the availability of highly effective direct-acting antiviral therapies. We found a low percentage of early-career family physicians treating HCV patients, and the percentage has decreased over the past decade. This finding is consistent with previous research; estimates from the CDC identified a steady decline in HCV treatment from 2015 to 2020.22,23 However, the data also showed that early-career family physicians in high-HCV mortality states, rural areas, and MUA practice had higher rates of HCV treatment provision.
To achieve national goals of eliminating HCV by 2030, recently reinforced in Senate bill 1941, policymakers and educators must seize opportunities for family physicians to expand care in this area and help improve access to HCV treatment for the most vulnerable populations.24,25 This necessity is particularly true in several high-need states, including Colorado and West Virginia, which have low rates of early-career family physicians providing HCV treatment and high rates of HCV mortality. Further, a recent study from the CDC found that fewer than 10% of patients diagnosed with HCV had been cured in West Virginia, compared to 34% for the United States. Colorado also was one of more than a dozen states with HCV cure rates below 26%.7 Interestingly, our analysis suggests that state-level Medicaid barriers to treatment did not have an impact on early-career family physician HCV treatment rates; several states with few or no barriers to treatment (including Colorado) had relatively low early-career family physician HCV treatment rates. While this finding may be explained partly by the fact that state-level Medicaid laws changed dramatically during the study period (2016–2023), Medicaid restrictions may play a role in West Virginia’s low early-career family physician HCV treatment rates because the state has several barriers for accessing treatment.12
Access to HCV treatment can be improved by increasing the number of primary care physicians who have the training, experience, and organizational support to initiate treatment.26,27 Wang et al described how primary care physicians are ideally suited to guide patients through the HCV cascade of care—from screening, providing linkages to care, and initiating treatment—and the importance of exposure to HCV treatment in residency training.27 Improving HCV treatment rates through increased training in residency is logical given that research has found that behaviors in residency training carry over to practice, defined as “imprinting.”28 However, previous research has found that low percentages of family physicians in their final year of residency training intend to treat HCV patients; this finding warrants more in-depth research on the impact of residency training on HCV treatment patterns.18 Future research will look at links between residency preparation in HCV treatment and HCV treatment rates of family physicians over time as they move from early- to midcareer.
This study had a few limitations. First, we used self-reported survey responses to assess current early-career family physician HCV treatment behavior. These responses were subject to recall bias and social desirability bias, and the data did not include any details on the HCV treatment or whether the early-career family physicians were referring to specialists or using a Project ECHO-like telehealth model.29 Further, pharmacy data were not available to verify that early-career family physicians were treating HCV patients. A related limitation was that practice type also was self-reported, meaning that some safety-net clinic types may not have been included as MUA practices. A second limitation involved our cross-sectional approach, which did not allow for identifying causal factors contributing to higher rates of early-career family physician HCV treatment provision. Future research topics include using qualitative approaches for gaining a more in-depth understanding of the factors that contribute to higher HCV treatment rates and better HCV clearance outcomes. A third limitation was related to our state-level analyses, which were subject to the ecological fallacy and were proxies for population demand at the practice level. Future research will explore the relationship between HCV prevalence, mortality, and treatment for smaller geographies, including counties.
This study was the first to explore the role of early-career family physicians in treating HCV at a national level in the United States. We found that while early-career family physician HCV treatment rates remain relatively low and have decreased over the past decade, early-career family physicians in the highest need areas (rural, MUA practice, high-burden states) are providing HCV treatment at higher rates. Reaching HCV elimination goals will require that family physicians take a larger role in providing HCV treatment, particularly among the most vulnerable populations.
This research was presented at the North American Primary Care Research Group Annual Meeting, November 21–25, 2025, Atlanta, GA.
Dr Bazemore and Dr Peterson are employees of the American Board of Family Medicine.
References
-
Hofmeister MG, Rosenthal EM, Barker LK, et al. Estimating prevalence of hepatitis C virus infection in the united states, 2013-2016.
Hepatology. 2019;69(3):1020–1031. doi:10.1002/hep.30297
-
-
-
Spaulding AC, Kennedy SS, Osei J, et al. Estimates of Hepatitis C Seroprevalence and Viremia in State Prison Populations in the United States.
J Infect Dis. 2023;228(Suppl 3):S160–S167. doi:10.1093/infdis/jiad227
-
US Preventive Services Task Force, Owens DK, Davidson KW, et al. Screening for Hepatitis C virus infection in adolescents and adults: US preventive services task force recommendation statement.
JAMA. 2020;323(10):970–975. doi:10.1001/jama.2020.1123
-
Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis C virus infection: a systematic review.
Ann Intern Med. 2017;166(9):637–648. doi:10.7326/M16-2575
-
Tsang CA, Tonzel J, Symum H, et al. State-specific hepatitis C virus clearance cascades - United States, 2013-2022.
MMWR Morb Mortal Wkly Rep. 2024;73(21):495–500. doi:10.15585/mmwr.mm7321a4
-
Thompson WW, Symum H, Sandul A, et al. Vital signs: hepatitis C treatment among insured adults - United States, 2019-2020.
MMWR Morb Mortal Wkly Rep. 2022;71(32):1011–1017. doi:10.15585/mmwr.mm7132e1
-
Scobie HM, Allison J, Masters N, et al. Newly reported chronic hepatitis C among adults - Alaska, 2016-2023.
MMWR Morb Mortal Wkly Rep. 2025;74(10):161–166. doi:10.15585/mmwr.mm7410a1
-
Gordon SC, Kaushik A, Chastek B, Anderson A, Yehoshua A. Characteristics associated with receipt of treatment among patients diagnosed with chronic hepatitis C virus.
J Viral Hepat. 2023;30(9):756–764. doi:10.1111/jvh.13860
-
Doshi RK, Ruben M, Drezner K, et al. Knowledge, attitudes, and behaviors related to hepatitis C screening and treatment among health care providers in Washington, DC.
J Community Health. 2020;45(4):785–794. doi:10.1007/s10900-020-00794-z
-
-
Bhattacharya D, Aronsohn A, Price J, et al. Hepatitis C guidance 2023 update: American association for the study of liver diseases– infectious diseases society of America recommendations for testing, managing, and treating hepatitis C virus infection.
Clin Infect Dis. 2023.
doi:10.1093/cid/ciad319
-
Kattakuzhy S, Gross C, Emmanuel B, et al. expansion of treatment for hepatitis C virus infection by task shifting to community-based nonspecialist providers: a nonrandomized clinical trial.
Ann Intern Med. 2017;167(5):311–318. doi:10.7326/M17-0118
-
Stewart A, Craig-Neil A, Hodwitz K, et al. increasing treatment rates for hepatitis C in primary care.
J Am Board Fam Med. 2023;36(4):591–602. doi:10.3122/jabfm.2022.220427R1
-
Jones AT, Briones C, Tran T, Moreno-Walton L, Kissinger PJ. Closing the hepatitis C treatment gap: United States strategies to improve retention in care.
J Viral Hepat. 2022;29(8):588–595. doi:10.1111/jvh.13685
-
Gonzalez CJ, Kapadia SN, Niederdeppe J, et al. The state of hepatitis C elimination from the front lines: a qualitative study of provider-perceived gaps to treatment initiation.
J Gen Intern Med. 2024;39(12):2268–2276. doi:10.1007/s11606-024-08807-6
-
Sonoda K, Morgan ZJ, Peterson LE. scope of practice intentions among family medicine residents for integrated care of HIV and hepatitis C infection in people with opioid use disorder.
Fam Med. 2025;57(1):41–47. doi:10.22454/FamMed.2024.703890
-
American Board of Family Medicine. National Graduate Survey reports, 2016–2023.
-
-
-
Centers for Disease Control and Prevention. New estimates reveal declines in hepatitis C treatment in the U.S. between 2015 and 2020. CDC; 2021.
-
Scialli A, Saab S, Salimian A, Bhattacharya D, Goodman-Meza D. Hepatitis C treatment among primary care and specialty providers: a single center study, 2015 to 2022.
J Prim Care Community Health. 2024;15. doi:10.1177/21501319241253521
-
-
-
Tran L, Feldman R, Riley T III, Jung J. Association of the extension for community healthcare outcomes project with use of direct-acting antiviral treatment among us adults with hepatitis C.
JAMA Netw Open. 2021;4(7). doi:10.1001/jamanetworkopen.2021.15523
-
Wang AE, Hsieh E, Turner BJ, Terrault N. Integrating management of hepatitis C infection into primary care: the key to hepatitis C elimination efforts.
J Gen Intern Med. 2022;37(13):3435–3443. doi:10.1007/s11606-022-07628-9
-
Phillips RL Jr, Holmboe ES, Bazemore AW, George BC. Purposeful imprinting in graduate medical education: opportunities for partnership.
Fam Med. 2021;53(7):574–577. doi:10.22454/FamMed.2021.264013
-
Komaromy M, Duhigg D, Metcalf A, et al. Project ECHO (Extension for community healthcare outcomes): a new model for educating primary care providers about treatment of substance use disorders.
Subst Abus. 2016;37(1):20–24. doi:10.1080/08897077.2015.1129388



There are no comments for this article.