Background and Objectives: Evaluating resident physicians is essential for resident development and patient safety. Fear of retaliation from residents may be a barrier to faculty completing resident physician evaluations. This study examined family medicine program directors’ perceptions on fear of retaliation from resident physicians as a barrier to faculty completing honest, high-quality evaluations.
Methods: The study was conducted as part of the 2024 Council of Academic Family Medicine Educational Research Alliance study of family medicine residency program directors. The 10-item survey assessed program directors’ perceptions of faculty fear of retaliation, the impact of this fear, and rates of retaliation occurring in their programs in the last 3 years.
Results: The response rate was 45.39% (320/705). More than half (56.4%, 172/305) perceived that faculty in their programs are reluctant to give critical feedback on evaluations; nearly half (48.9%, 150/305) believed that fear of retaliation is a barrier. Fear of a reciprocal negative evaluation (34.5%, 106/305) and fear of formal complaints (38.9%, 119/305) were prevalent. Lack of adequate documentation was attributed to a failure to remediate and dismiss a resident in 19.8% (61/307) and 11.7% (36/306) of programs, respectively. Formal complaints against an evaluator or program occurred in 18.6% (57/307) of programs, and civil lawsuits were filed in 5.2% (16/306) in the preceding 3 years.
Conclusions: Family medicine program directors perceive fear of retaliation from residents as a barrier to faculty completing honest, high-quality evaluations. Formal complaints and even civil lawsuits against evaluators or programs are not uncommon.
Many medical educators across disciplines report challenges in the provision of high-quality, effective feedback and evaluations, particularly with regard to negative performance evaluations for trainees.1 An analysis of more than 77,000 numeric scores on end-of-rotation evaluations in three residency programs (internal medicine and anesthesia) revealed fewer than 1% indicated below average performance.2 Time constraints, fear of damaging the relationship between the resident and evaluator, anticipated resident resistance to negative feedback, and lack of comfort with delivery of negative feedback are well-described in the literature, though often with small studies and not specific to family medicine residencies.3,4 Only a limited amount of literature is dedicated to fear of negative repercussions as barriers to the completion of high-quality, honest feedback.3-7
A previous Council of Academic Family Medicine Educational Research Alliance (CERA) study of family medicine program directors identified a high incidence of residents undergoing remediation, and one of the top two barriers to the remediation process was the lack of documented evaluations. However, the reasons for this lack of documentation were not investigated.8 A study that included 156 anesthesia residents concluded that faculty overestimate the risk of retaliation from residents; however that was based on residents self-reporting their hypothetical likelihood of retaliation.9 Evidence also exists of a reciprocity effect among surgical residents and faculty (ie, trainees modify their evaluation of faculty members based on the evaluations the faculty members produce for the trainee) as well as fear of reciprocity from radiology educators at a single site.7,10 A survey of 22 Canadian medical educators (represented mostly by surgical specialties) indicated fear of retaliation, including that of appeals and legal action, as a barrier to accurately reporting poor performance. This concern appears to be particularly high among faculty of lower academic rank; assistant professors were significantly less likely to give low performance ratings to clerkship students than full professors, suggesting perceived vulnerability to feedback.11 More than half of those respondents reported passing a resident who would have benefited from additional training.8 Another small Canadian survey of 21 clinical educators (mix of surgery and internal medicine) indicated a fear of the appeals process or potential legal action as one of four major barriers to providing a failing evaluation.7
The prevalence of fear of retaliation as a barrier has not been examined among family medicine programs and has not yet been examined as part of a large-scale, multiprogram study. Given the frequency in which family medicine residency programs have residents in remediation and the identified challenge of having adequate documentation to make the process successful, identification of the fear of retaliation as a barrier is important.8 We hypothesized that fear of retaliation is perceived as a barrier in most family medicine residency programs and that recent experience with retaliation makes this perception more likely.
Participants
Between April 30, 2024, and June 7, 2024, family medicine program directors of US family medicine residency programs that had at least three graduating classes and an active email address (N = 705) were invited to participate in an online survey. The project was part of a larger CERA omnibus study. Email invitations to participate were delivered using the platform SurveyMonkey (SurveyMonkey Inc). Nonresponders received five weekly follow-up emails encouraging participation, with a sixth reminder sent 1 day before the survey closed. For additional description of the CERA survey, see Seehusen et al.12
Survey Development
The 10-question survey was developed by the first four authors, who are interdisciplinary clinician educators, and revised with input from the senior author and two medical librarians. The survey was developed to assess program directors’ perception of the fear of retaliation from residents through formal institutional or legal channels as a barrier to faculty completion of high-quality and honest evaluations in their programs, as well as actual incidence of negative outcomes (ie, as graduating a resident who needed additional training, appeals, formal complaints, and legal action). Program directors were chosen as the survey participants because they have the most comprehensive viewpoint of their residents’ performance and their faculty members’ habits returning assigned evaluations. Given that resident remediation typically requires a high degree of confidentiality, program directors were considered best suited to assess whether they believe residents graduated from their programs who should have had additional training or dismissal but lacked necessary documentation; they also were considered most likely to be aware of actions such as formal complaints, appeals, or lawsuits. The CERA steering committee evaluated the questions for consistency with the overall subproject aim, readability, and existing evidence of reliability and validity. Pretesting was performed on flow, timing, and readability by family medicine educators who were not part of the target population.
Analysis
We created three scales based on the content of the survey items.
Perceived fear of retaliation as a barrier: consisted of four items with a Likert-scale (eg, “A barrier to high-quality, honest evaluation completion is fear of retaliation from the resident in any form;” 1–strongly disagree to 5–strongly agree); scores could range from 4 to 20, with higher scores indicating fear of retaliation having a stronger negative impact on faculty ratings.
Failure to remediate and/or dismiss residents: consisted of three items with a 3-point scale (eg, “In the last 3 years, has the program graduated a resident you felt should have undergone remediation or a reportable action that did not due to lack of necessary documentation?”; 1–no, 2–once, 3–multiple times); scores could range from 3 to 9, with higher scores indicating a greater incidence of failing to remediate or dismiss residents when warranted.
Resident action after adverse decision: consisted of three items with a 3-point scale (eg, “In the last 3 years, has a resident appealed a remediation process, dismissal, or other reportable action?”; 1–no, 2–once, 3–multiple times); scores could range from 3 to 9, with higher scores indicating a greater incidence of residents taking action after an adverse decision, such as appealing a decision, filing a formal complaint, or filing a civil lawsuit.
To determine relationships among the three scales, we used the Pearson product-moment correlation coefficient and set the α at P<0.05. To determine the relationship among program characteristics (ie, program type and program size) and the three scales, we used a 3×3 analysis of variance for each scale and set the α at P<0.05. To determine the relationship among program director characteristics (ie, number of years in current role, gender identity, underrepresented minority [URM] identity) and the three scales, we used multiple linear regression for each scale and set the α at P<0.05.
The American Academy of Family Physicians Institutional Review Board approved the project in April 2024.
The overall response rate was 45.39% (320/705). Program director demographics and characteristics are detailed in Table 1, and program characteristics are detailed in Table 2.
Characteristic |
Frequency |
Percentage |
Type of degree |
MD |
250/316 |
79.1 |
DO |
66/316 |
20.9 |
Years in current role
(M = 5.3, SD = 5.01) |
<1 year |
22/320 |
6.9 |
1 to<3 years |
91/320 |
28.4 |
3 to<6 years |
93/320 |
29.1 |
6 to<10 years |
63/320 |
19.7 |
10 or more years |
51/320 |
15.9 |
Years as program director
(M = 6.03, SD = 5.54) |
<1 year |
21/315 |
6.7 |
1 to<3 years |
79/315 |
25.1 |
3 to<6 years |
88/315 |
27.9 |
6 to<10 years |
57/315 |
18.1 |
10 or more years |
70/315 |
22.2 |
Gender |
Female/woman |
177/320 |
55.3 |
Male/man |
138/320 |
43.1 |
Not reported |
5/320 |
1.6 |
Identified as URM |
No |
276/320 |
86.3 |
Yes |
43/320 |
13.4 |
Not reported |
1/320 |
0.3 |
Race and ethnicity |
American Indian/Alaska Native/Indigenous |
1/320 |
0.3 |
Asian |
27/320 |
8.4 |
Black/African American |
14/320 |
4.4 |
Hispanic/Latino/of Spanish origin |
17/320 |
5.3 |
Middle Eastern/North African |
2/320 |
0.6 |
White |
238/320 |
74.4 |
Not reported |
8/320 |
2.5 |
Multiple selections |
13/320 |
4.1 |
Characteristic |
Frequency |
Percentage |
Program type |
Community-based, affiliated with a university |
188/320 |
58.5 |
Community-based, not affiliated with a university |
77/320 |
24.1 |
University-based |
47/320 |
14.7 |
Military |
4/320 |
1.3 |
Other |
4/320 |
1.3 |
Program region |
New England |
11/320 |
3.4 |
Middle atlantic |
50/320 |
15.6 |
South atlantic |
49/320 |
15.3 |
East south central |
12/320 |
3.8 |
East north central |
59/320 |
18.4 |
West south central |
37/320 |
11.6 |
West north central |
28/320 |
8.8 |
Mountain |
26/320 |
8.1 |
Pacific |
48/320 |
15.0 |
Program community size |
<30,000 |
41/319 |
12.9 |
30,000 to 74,999 |
59/319 |
18.5 |
75,000 to 149,000 |
64/319 |
20.1 |
150,000 to 499,999 |
73/319 |
22.9 |
500,000 to 1 million |
33/319 |
10.3 |
>1 million |
49/319 |
15.4 |
Program size |
<19 residents |
121/319 |
37.9 |
19 to 31 |
148/319 |
46.4 |
>31 residents |
50/319 |
15.7 |
Program Director-Perceived Fear of Retaliation as a Barrier
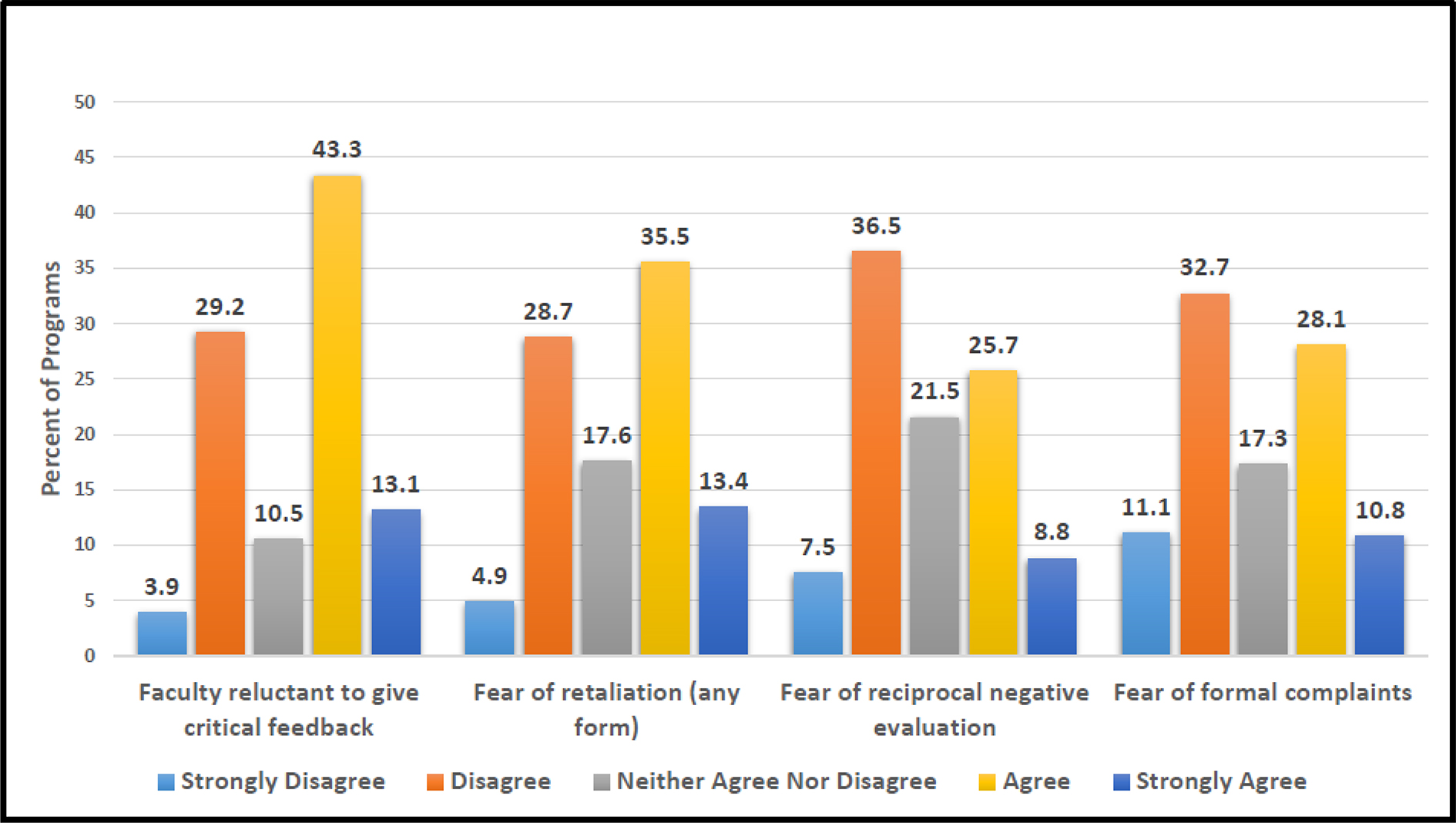
More than half (56.4%, 172/305) of program directors strongly agreed/agreed that faculty are reluctant to give feedback on evaluations that may be perceived as critical, and nearly half (48.9%, 150/305) perceived that fear of retaliation from an evaluated resident is a barrier (Figure 1). Specifically, 34.5% (106/305) perceived fear of a reciprocal negative evaluation, and 38.9% (119/305) perceived fear of formal complaints against the evaluator or program through the institution or legal system.
Failure to Remediate and/or Dismiss Residents
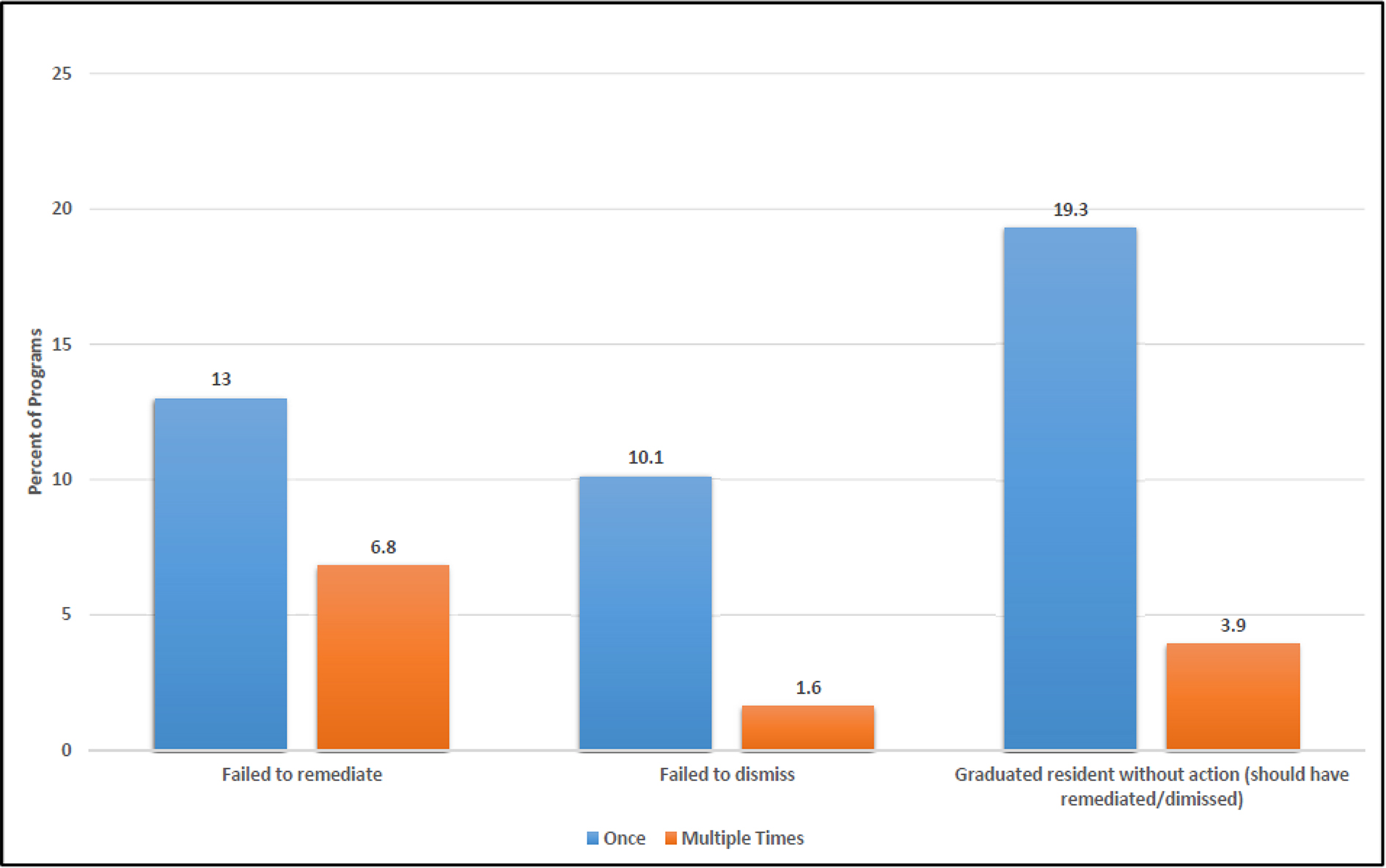
In the past 3 years, 19.8% (61/307) of program directors reported that insufficient documentation led to at least one failure to remediate a resident, and 11.7% (36/306) said that it led to at least one failure to dismiss a resident (Figure 2). Nearly a quarter (23.2%, 71/306) of program directors have graduated a resident in the last 3 years they believed should have undergone remediation or other reportable action but did not, with 3.9% (12/306) doing so multiple times.
Resident Action After an Adverse Action
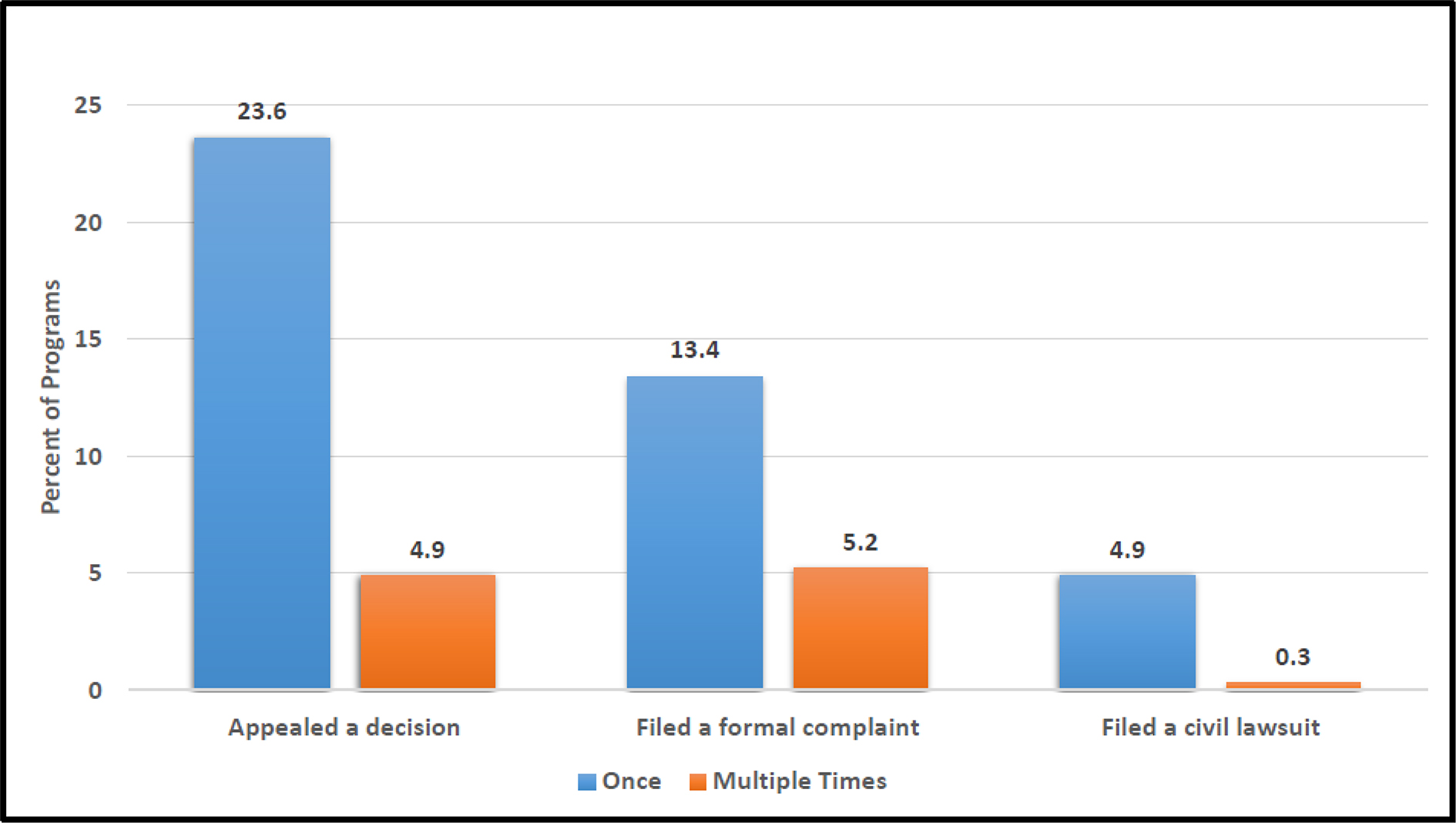
In the last 3 years, 28.5% (87/305) of programs had a resident appeal a remediation process, dismissal, or other reportable action at least once (Figure 3). Formal complaints of any kind against faculty evaluators or the program regarding an evaluation, remediation, dismissal, or other reportable action occurred in 18.6% (57/307) of programs, and civil lawsuits were filed in 5.2% (16/306).
Relationships Among Variables
We identified a statistically significant correlation between perceived fear of retaliation as a barrier scale and failure to remediate and/or dismiss residents scale (r = 0.303, P<0.001), and between the failure to remediate and/or dismiss residents scale and resident action after adverse decision scale (r = 0.233, P<0.001). We found no relationship between the perceived fear of retaliation scale and resident action after adverse decision scale (r = 0.106, P=0.066).
Regarding program size and type, only the relationship between program size and resident action after adverse decision were significant, with post hoc analysis (LSD) indicating that larger programs had significantly more resident actions after adverse decisions than small (P=0.030, 95% CI = 0.038, 0.751) and medium programs (P=0.008, 95% CI = 0.124, 0.819).
No significant relationship existed between program director characteristics (ie, number of years in current role, gender identity, URM identity) and measured outcomes.
Most family medicine program directors perceived fear of retaliation from residents as a barrier to their faculty providing high-quality, honest evaluations. Formal complaints against faculty or the program regarding an evaluation or other program action was common, and more than 5% of programs or their faculty had been sued in the 3 year study period, indicating the perceived fear from faculty has some merit. Nearly one-third of programs had experienced challenges with remediating due to insufficient documentation, and more than one in 10 programs had failed to dismiss a resident due to insufficient documentation over the preceding 3 years. Although this study did not directly link faculty-reported fear of retaliation to these outcomes, it likely accounted for at least some of the lack of documentation, given the high prevalence of the perceived barrier.
This is the largest study in graduate medical education to assess the prevalence of this barrier to faculty evaluation completion. The lack of significant relationships among these findings and program characteristics suggests that this is a resident-driven rather than institutionally driven phenomenon. This finding may reflect differences between resident and faculty expectations regarding feedback, remediation, and rights within training programs. Increased awareness of formal complaint avenues and legal protections could drive residents to be more vigilant about challenging negative feedback or decisions perceived as adverse, particularly given the significant impact that disciplinary actions may have on a resident’s career. Emphasis on resident well-being, due process, and transparency may have unintentionally contributed to faculty reluctance to provide critical feedback, fearing institutional or legal consequences. Due to a lack of previous data, whether these findings represent a long-standing norm or change in perceived attitudes and behaviors is unclear.
Limitations of this study included reliance on self-reported data from program directors, which introduces the possibility of bias, because their perceptions will not fully reflect the experiences of faculty or residents. The 45.39% response rate, while similar to survey rates for physician specialists and consistent with prior CERA surveys, may limit its generalizability.13 In particular, program directors with higher levels of program-related stress possibly may not have responded, leading to an underreporting of relevant factors. Another possible limitation is the potential for unmeasured confounding factors, such as institutional culture or local policies, which could influence both the prevalence of retaliation fears and the decisions to remediate or dismiss residents. The cross-sectional nature of the study further limited our ability to draw conclusions about causality, and other unexamined factors, such as variations in faculty training or support, could possibly contribute to the observed trends.
Future research should explore interventions aimed at mitigating fear of retaliation and improving the remediation and evaluation processes. An important first step may be to ensure that residency faculty are adequately trained in providing feedback and partnering effectively with struggling learners. For example, recent research on best practice among struggling family medicine resident learners has emphasize the importance of conducting early assessment and identification, ensuring resident engagement, and providing consistent feedback; this research suggests that supporting learners early may prevent the need for formal remediation later in residency.14 Junior faculty in particular may struggle with giving feedback, despite evidence that residents have reported wanting constructive feedback to enhance their learning; and training faculty in best practice for providing feedback is an ongoing need.9,15 Similar results in studies across other specialties could elucidate whether these findings are generalized across graduate medical education or specialty-specific. Also important may be to replicate questions regarding fear of retaliation among program faculty to examine whether program directors’ perspective of fear of retaliation is consistent with that reported by faculty themselves. Additionally, research into resident perspectives on the evaluation process could provide valuable insights and lead to more balanced solutions for both faculty and residents.
According to program directors, fear of retaliation from residents is a widespread barrier to honest faculty evaluations across family medicine programs of varying characteristics. This may contribute to alarming rates of insufficient documentation needed when remediation or program dismissal is warranted. Formal complaints and civil lawsuits against evaluators and programs are not uncommon.
The authors thank Gwen Sprague, medical librarian, University Health Lakewood Medical Center, and Jennifer Livingston, MD, who reviewed the survey questions.
References
-
Yepes-Rios M, Dudek N, Duboyce R, Curtis J, Allard RJ, Varpio L. The failure to fail underperforming trainees in health professions education: A BEME systematic review: BEME Guide No. 42.
Med Teach. 2016;38(11):1092–1099. doi:10.1080/0142159X.2016.1215414
-
Anderson LM, Rowland K, Edberg D, Wright KM, Park YS, Tekian A. An analysis of written and numeric scores in end-of-rotation forms from three residency programs.
Perspect Med Educ. 2023;12(1):497–506. doi:10.5334/pme.41
-
Watling CJ, Kenyon CF, Schulz V, Goldszmidt MA, Zibrowski E, Lingard L. An exploration of faculty perspectives on the in-training evaluation of residents.
Acad Med. 2010;85(7):1157–1162. doi:10.1097/ACM.0b013e3181e19722
-
McCutcheon S, Duchemin AM. Overcoming barriers to effective feedback: a solution-focused faculty development approach.
Int J Med Educ. 2020;11:230–232. doi:10.5116/ijme.5f7c.3157
-
Chelliah P, Srivastava D, Nijhawan RI. What makes giving feedback challenging? A survey of the Association Of Professors Of Dermatology (APD).
Arch Dermatol Res. 2023;315(2):291–294. doi:10.1007/s00403-022-02370-y
-
Dudek NL, Marks MB, Regehr G. Failure to fail: the perspectives of clinical supervisors.
Acad Med. 2005;80(10 Suppl):S84–7. doi:10.1097/00001888-200510001-00023
-
McQueen SA, Petrisor B, Bhandari M, Fahim C, McKinnon V, Sonnadara RR. Examining the barriers to meaningful assessment and feedback in medical training.
Am J Surg. 2016;211(2):464–475. doi:10.1016/j.amjsurg.2015.10.002
-
Frazier W, Wilson SA, D’Amico F, Bergus GR. Resident remediation in family medicine residency programs: a CERA survey of program directors.
Fam Med. 2021;53(9):773–778. doi:10.22454/FamMed.2021.546572
-
Wolpaw J, Saddawi-Konefka D, Dwivedi P, Toy S. Faculty underestimate resident desire for constructive feedback and overestimate retaliation. J Educ Perioper Med. 2019;21(4).
-
Cousar M, Huang J, Sebro R, Levin D, Prabhakar H. Too scared to teach? The unintended impact of 360-degree feedback on resident education.
Curr Probl Diagn Radiol. 2020;49(4):239–242. doi:10.1067/j.cpradiol.2019.04.006
-
Swails JL, Gadgil MA, Goodrum H, Gupta R, Rahbar MH, Bernstam EV. Role of faculty characteristics in failing to fail in clinical clerkships.
Med Educ. 2022;56(6):634–640. doi:10.1111/medu.14725
-
Seehusen DA, Mainous AG III, Chessman AW. Creating a centralized infrastructure to facilitate medical education research.
Ann Fam Med. 2018;16(3):257–260. doi:10.1370/afm.2228
-
Cunningham CT, Quan H, Hemmelgarn B, et al. Exploring physician specialist response rates to web-based surveys.
BMC Med Res Methodol. 2015;15(1). doi:10.1186/s12874-015-0016-z
-
Haymaker CM, Schilling J, Fraser K, et al. Best practices for early intervention and remediation of residents in family medicine: insights from an interdisciplinary delphi study.
Fam Med. 2025;57(2):98–106. doi:10.22454/FamMed.2025.820384
-
Natesan S, Jordan J, Sheng A, et al. Feedback in medical education: an evidence-based guide to best practices from the Council of Residency Directors in Emergency Medicine.
West J Emerg Med. 2023;24(3):479–494. doi:10.5811/westjem.56544



There are no comments for this article.