Background and Objectives: Tensions between clinical and hospital training, along with dysfunctional family medicine training clinics, have resulted in continuity clinic being the least favorite part of training for some residents. These factors are all contributors to burnout. We hypothesized that following Clinic First action steps to prioritize and enhance outpatient clinic would positively affect resident wellness and clinic engagement. This study describes our interventions and their effects within the Oregon Health & Science University (OHSU) Family Medicine 4-year Portland residency program.
Methods: In July 2017 the Oregon Health & Science University Family Medicine Portland residency program implemented scheduling and curricular interventions inspired by the Clinic First model. We conducted a mixed-methods cross-sectional study using focus groups and surveys to understand the effects of these interventions on resident wellness and engagement.
Results: Clinic First-inspired interventions, particularly a 2+2 scheduling model, decreased transitions within the day, and a clinic immersion month were associated with improved residents’ perception of wellness. These interventions had variable effects on clinic engagement. Eighty-eight percent of interns surveyed about the month-long clinic orientation in the beginning of residency reported that they felt prepared managing continuity patients in the clinic setting and their upcoming rotations.
Conclusions: This study demonstrates that Clinic First-inspired structural changes can be associated with improvement in resident perceptions of wellness and aspects of clinic engagement. This can give educators a sense of hope as well as tangible steps to take to improve these difficult and important issues.
The majority of family medicine clinicians provide care primarily in outpatient settings,1 yet most family medicine residencies use rotation-based models favoring inpatient care. This comes at the expense of outpatient training, which often occurs in underfunded, dysfunctional clinics.2-4 Furthermore, most programs lack structured outpatient curricula and fail to deliver skills necessary to thrive in evolving primary care models.5 These tensions between inpatient and outpatient training result in clinic being the least favorite part of training for some residents.4
Inadequate training and dysfunctional practices are risk factors for burnout, which disproportionally affects family physicians.6 Cumbersome geographic and mental transitions from inpatient to outpatient settings can further add to learner stress.4 Models prioritizing quality resident outpatient training are needed to improve wellness.7
Bodenheimer, et al describe a Clinic First model that provides steps programs can take regarding resident scheduling, engagement, and work-life balance to emphasize quality ambulatory training in high-functioning clinics.4,8,9 While studies have examined alternative scheduling models, few have evaluated comprehensive Clinic First educational interventions.3, 10-16 Most studies focus on clinic metrics, leaving the effects on resident wellness and engagement largely unstudied.
We hypothesized that adopting a Clinic First model to make outpatient clinic training a cornerstone would positively affect resident wellness and clinic engagement.9 This study describes our interventions and their effects within the Oregon Health & Science University (OHSU) Family Medicine 4-year Portland residency program.
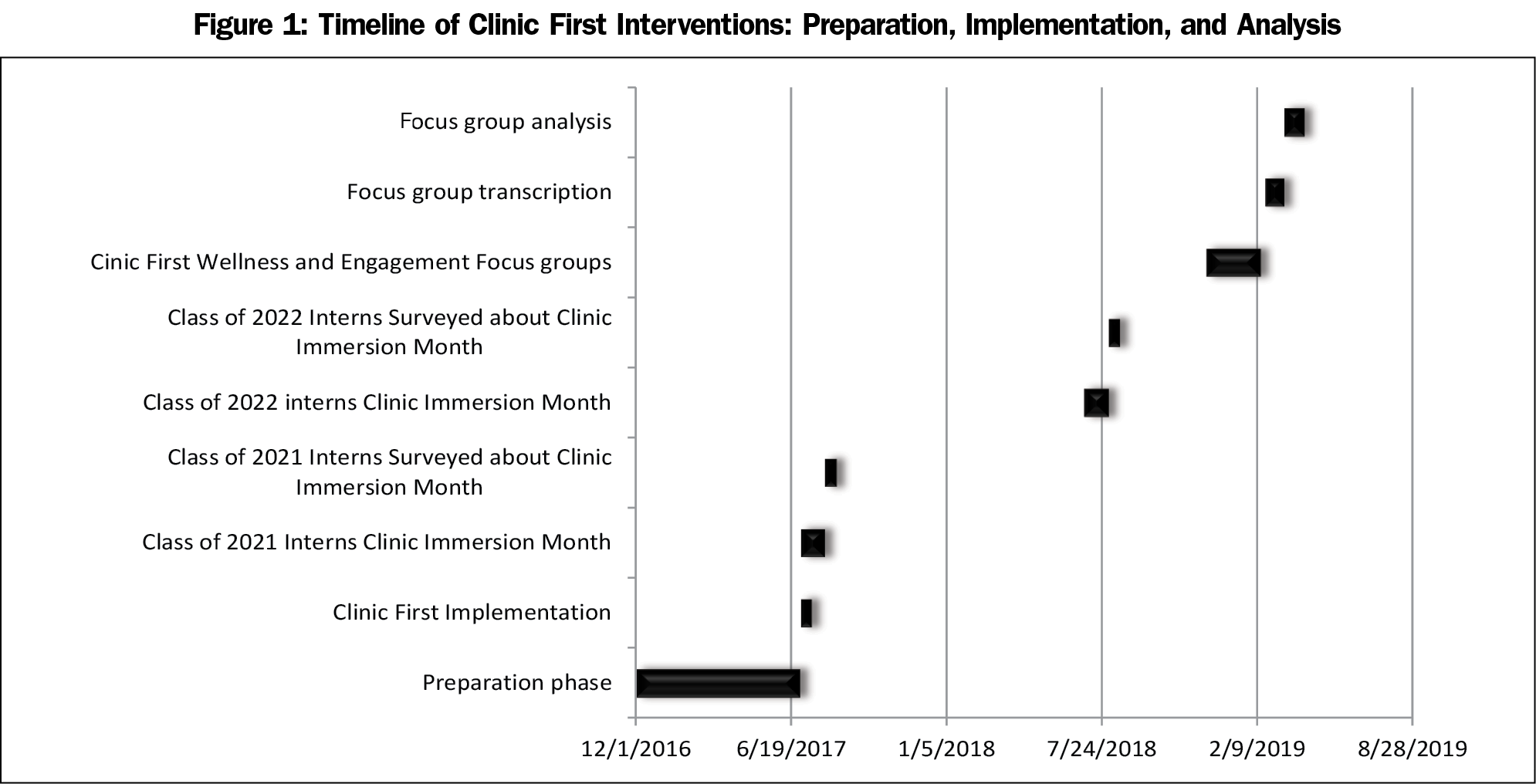
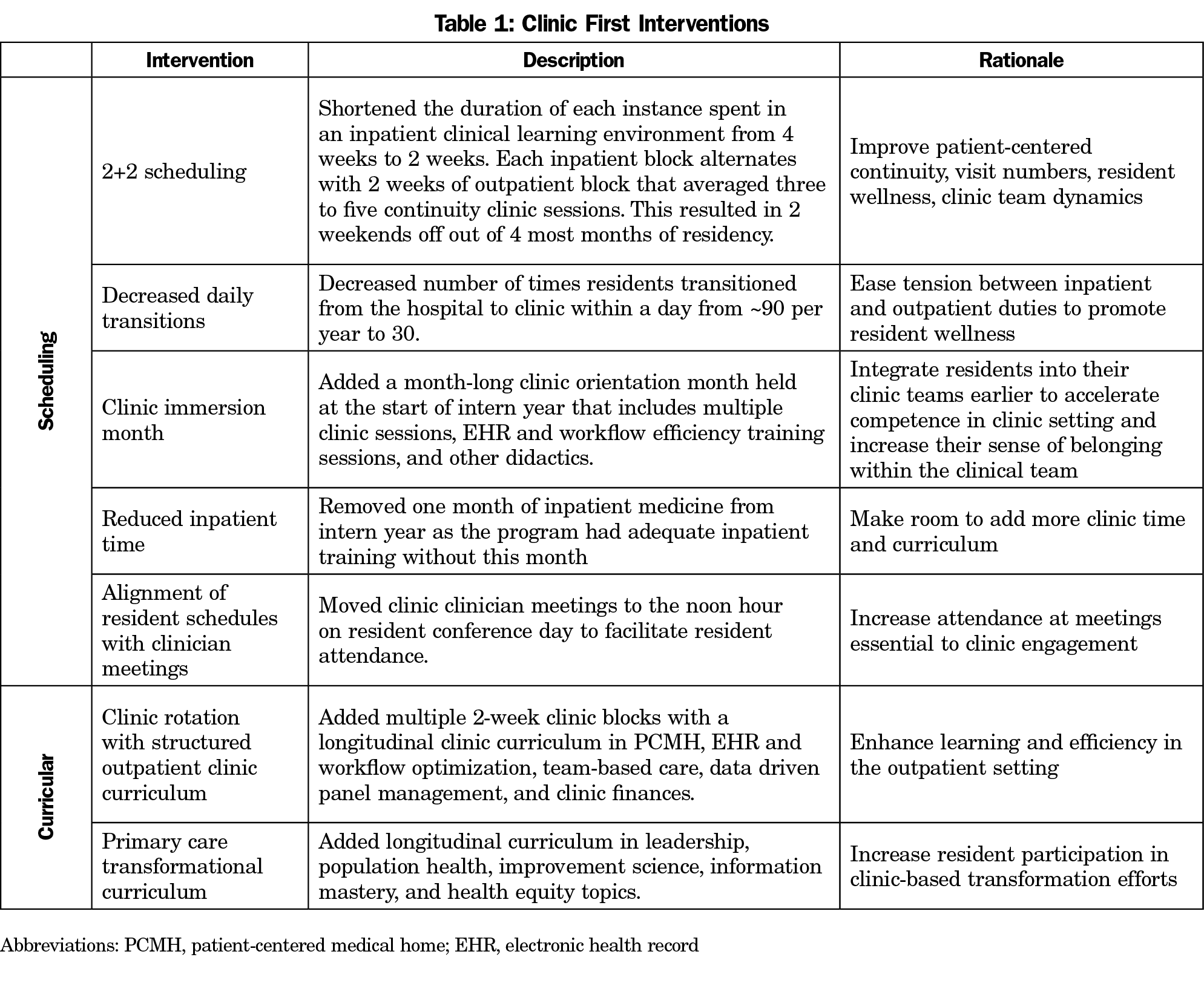
We conducted a mixed-methods cross-sectional study of 47 residents enrolled in our residency program from July 2017 to February 2019 (Figure 1). Seven scheduling and curricular interventions were made (Table 1) in July 2017.
Focus Groups
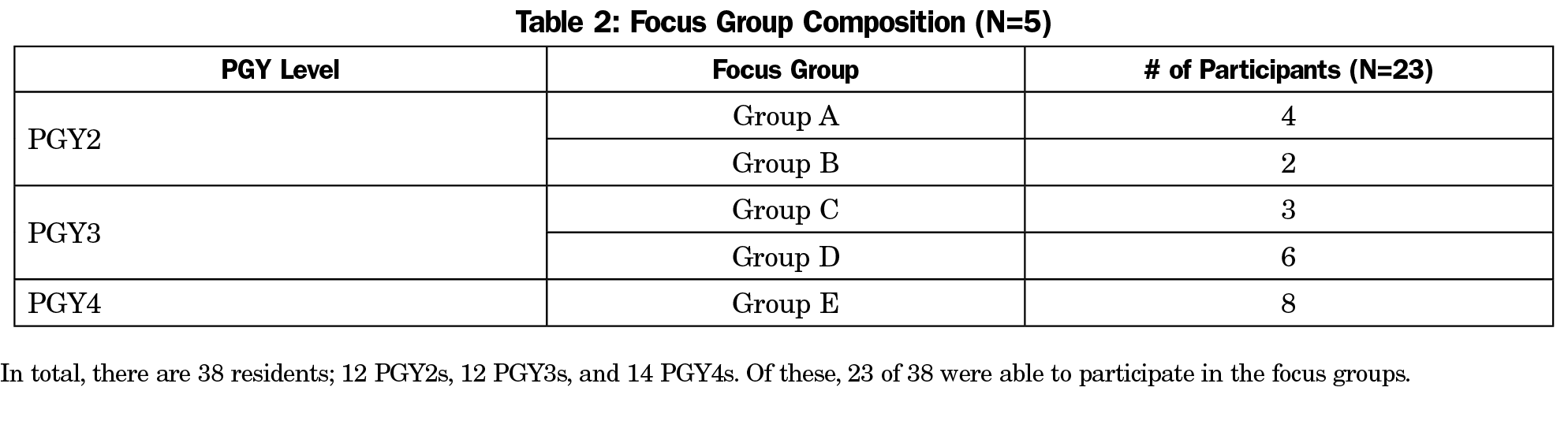
Eighteen months after intervention implementation, family medicine department research associates conducted focus groups without evaluative roles within the residency (Table 2). Primary outcomes were resident wellness and clinic engagement. To encourage a wide range of responses, outcomes were not predefined.
The study team developed a series of open-ended questions that asked residents to reflect on how the curricular interventions affected their wellness and engagement (See Appendix). Third- and fourth-year residents (PGY-3s and PGY-4s) were asked to compare their experiences before and after the interventions. Second-year residents (PGY-2s) had no preintervention reference point so were not asked to compare. First-year residents (PGY-1s) were not included, given their limited time in the program at the time of study. A third party transcribed the interviews.
We used grounded theory and immersion-crystallization approaches to transcript analysis. For the purpose of analysis, we defined wellness as performing well at work and gleaning meaning or enjoyment from work while maintaining physical and mental health. We defined clinic engagement as residents’ enjoying clinic, being present for a patient panel, and being involved in clinic operations. Independent analysis and coding by each member of the research team was followed by in-person meetings to develop themes by consensus.17
Survey
We administered an online survey to two classes of PGY-1s (n=24 total) in August 2017 and August 2018 at the end of the clinic immersion month(s). We used open- and close-ended questions to understand residents’ perceived preparedness for work in their continuity clinics and rotations after the intervention. Close-ended questions used a 5-point Likert scale.
The OHSU Institutional Review Board approved this study.
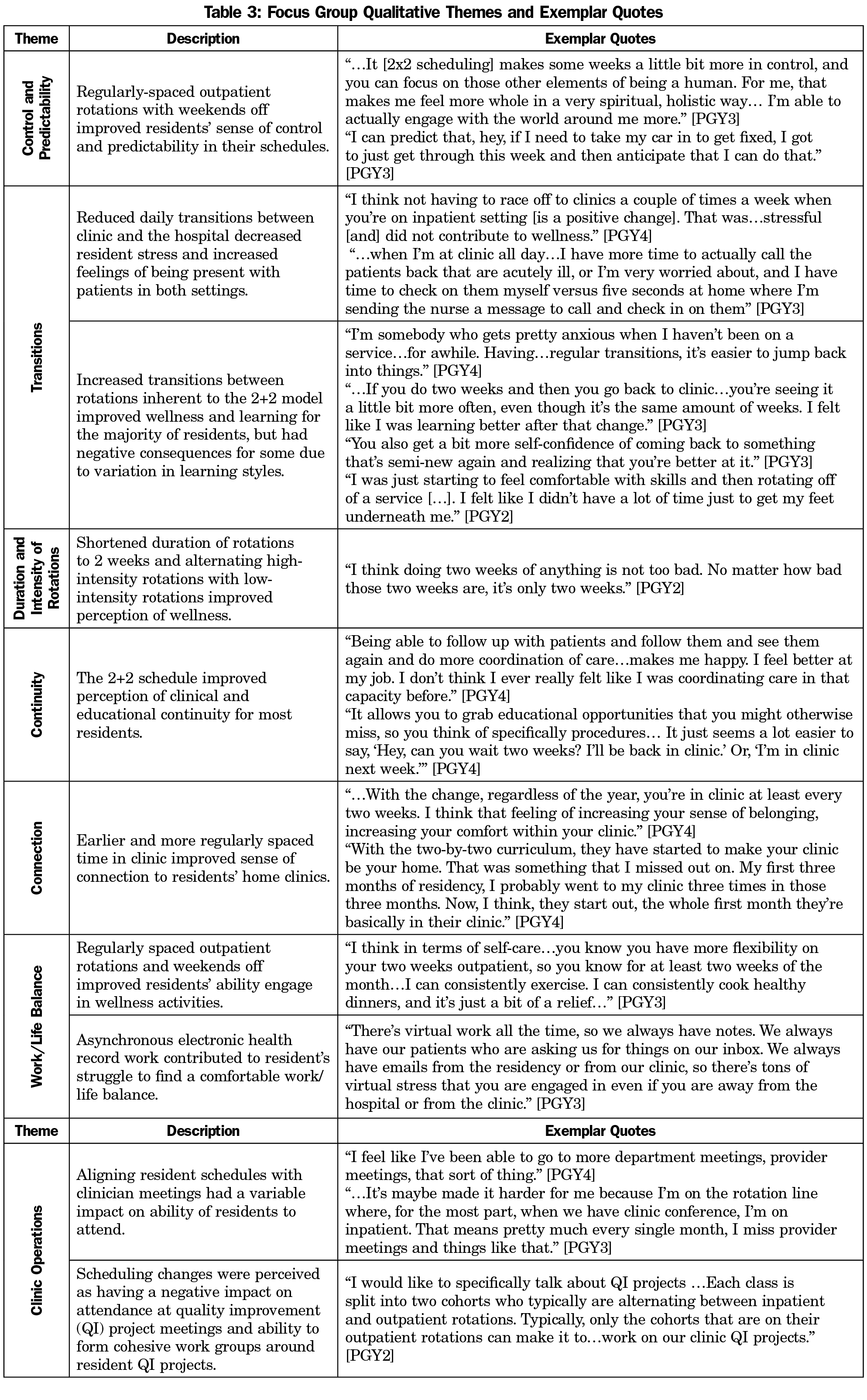
We convened five focus groups December 2018 through February 2019. Participants included 6 of 12 PGY-2s (50%), 9 of 12 PGY-3s (75%), and 8 of 14 PGY-4s (57%). Emergent themes around wellness and clinic engagement included control and predictability in one’s schedule, transitions within the day and between rotations, duration and intensity of rotations, continuity, connection, work/life balance, and clinic operations (Table 3).
Completion rate for the survey was 70% (17/24); 88% of residents reported feeling prepared for rotations and managing continuity patients. Residents reported they would feel more prepared with increased clinical sessions, electronic health record inbox training, and community activities. They also recommended fewer didactic lectures.
This study provides early data on the potential effects of Clinic First interventions on resident wellness and clinic engagement. Themes suggest the 2+2 model, decreased daily transitions, reduced inpatient time, and the clinic immersion month are associated with improved perceptions of multiple factors known to contribute to wellness.4,6,7,11 Increased transitions between rotations inherent to 2+2 scheduling are perceived as mostly positive with some caveats that appear to be based on learning style differences.
Clinic engagement themes suggest residents may feel more comfortable and present with their patients while in clinic, but continue to struggle with asynchronous patient care tasks and being involved in clinic operations. Specifically, clinician meeting attendance has not improved, likely due to the need to physically transition to clinic at noon without adequate travel time. Additionally, resident engagement in QI project meetings has not improved. While the ability and expectations of residents to attend these meetings has not changed, residents perceive that the 2+2 scheduling creates barriers to attendance and meaningful group work because it creates two separate cohorts of residents. These findings highlight the importance of evaluation and continual process improvement when undertaking curricular changes.
This study has a number of limitations. As a single training site testing one approach to Clinic First implementation, our results may not be generalizable to other programs. Further, lack of a comparison group inhibits us from attributing causality to interventions. Bias among the analysis group is a possibility, as they created the study interventions. Measurement bias is also possible as our clinic immersion month survey measured resident preparedness, which we viewed as a surrogate for wellness and engagement.
This study focused on the scheduling aspects of our Clinic First transition. It will be important to further study optimal Clinic First scheduling models and curricular interventions and methods for blending inpatient and outpatient care responsibilities.
Nationally, many programs have interest in moving towards a Clinic First model.18 The implication that this model could improve resident perception of wellness and clinic engagement can give educators a sense of hope when tackling these difficult and important issues.
Acknowledgments
Presentations: This study was presented at the 2019 Society of Teachers of Family Medicine Annual Spring Conference, April 30, 2019, Toronto, ON, Canada.
References
- American Academy of Family Physicians. Selected Practice Characteristics of Active AAFP Members (Dec 2018). Leawood, KS: AAFP; 2018. https://www.aafp.org/about/the-aafp/family-medicine-specialty/facts/table-4.html. Accessed July 26, 2019.
- Keirns CC, Bosk CL. Perspective: the unintended consequences of training residents in dysfunctional outpatient settings. Acad Med. 2008;83(5):498-502. https://doi.org/10.1097/ACM.0b013e31816be3ab
- Wieland ML, Halvorsen AJ, Chaudhry R, Reed DA, McDonald FS, Thomas KG. An evaluation of internal medicine residency continuity clinic redesign to a 50/50 outpatient-inpatient model. J Gen Intern Med. 2013;28(8):1014-1019. https://doi.org/10.1007/s11606-012-2312-1
- Gupta R, Dubé K, Bodenheimer T. The road to excellence for primary care resident teaching clinics. Acad Med. 2016;91(4):458-461. https://doi.org/10.1097/ACM.0000000000001100
- Anderson A, Simpson D, Kelly C, Brill JR, Stearns JA. The 2020 physician job description: how our GME graduates will meet expectations. J Grad Med Educ. 2017;9(4):418-420. https://doi.org/10.4300/JGME-D-16-00624.1
- Kumar S. Burnout and doctors: prevalence, prevention and intervention. Healthcare (Basel). 2016;4(3):E37. https://doi.org/10.3390/healthcare4030037
- Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-576. https://doi.org/10.1370/afm.1713
- Bodenheimer T, Ghorob A, Willard-Grace R, Grumbach K. The 10 building blocks of high-performing primary care. Ann Fam Med. 2014;12(2):166-171. https://doi.org/10.1370/afm.1616
- Gupta R, Barnes K, Bodenheimer T. Clinic first: 6 actions to transform ambulatory residency training. J Grad Med Educ. 2016;8(4):500-503. https://doi.org/10.4300/JGME-D-15-00398.1
- Bates CK, Yang J, Huang G, et al. Separating residents’ inpatient and outpatient responsibilities: improving patient safety, learning environments, and relationships with continuity patients. Acad Med. 2016;91(1):60-64. https://doi.org/10.1097/ACM.0000000000000849
- Bordley J, Agustin AG, Ahmed MA, et al. Restoration of resident sleep and wellness with block scheduling. Med Educ. 2017;51(12):1241-1249. https://doi.org/10.1111/medu.13392
- Buckhold FR III, Sanley MJ, Paniagua MA. An evaluation of continuity clinic redesign. J Gen Intern Med. 2013;28(12):1556. https://doi.org/10.1007/s11606-013-2612-0
- Chaudhry SI, Balwan S, Friedman KA, et al. Moving forward in GME reform: a 4 + 1 model of resident ambulatory training. J Gen Intern Med. 2013;28(8):1100-1104. https://doi.org/10.1007/s11606-013-2387-3
- Francis MD, Wieland ML, Drake S, et al. Clinic design and continuity in internal medicine resident clinics: findings of the educational innovations project ambulatory collaborative. J Grad Med Educ. 2015;7(1):36-41. https://doi.org/10.4300/JGME-D-14-00358.1
- Hussain AJ. Alternative Scheduling Models: Improving Continuity of Care, Medical Outcomes, and Graduate Medical Education in Resident Ambulatory Training. J Am Osteopath Assoc. 2016;116(12):794-800. https://doi.org/10.7556/jaoa.2016.155
- Heist K, Guese M, Nikels M, Swigris R, Chacko K. Impact of 4 + 1 block scheduling on patient care continuity in resident clinic. J Gen Intern Med. 2014;29(8):1195-1199. https://doi.org/10.1007/s11606-013-2750-4
- Crabtree BF, Miller WL, eds. Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999.
- Zeller TA, Ewing JA, Asif IM. Prevalence of clinic first curricula: a survey of AFMRD members. Fam Med. 2019;51(4):338-343. https://doi.org/10.22454/FamMed.2019.666943



There are no comments for this article.