Over the past 50 years, Residency Program Solutions (RPS) has been a key participant in supporting family medicine residency training programs and program leadership development. RPS is a peer consultation service offered by the American Academy of Family Physicians to help both new and established family medicine residency programs fulfill related Accreditation Council for Graduate Medical Education program requirements for residency training. Shepherded by an RPS Criteria for Excellence manual, which is constantly evolving and updated regularly, RPS consultants utilize various in-person and virtual consultation formats in response to the needs of their clients. This article summarizes the contributions of RPS over the last five decades and highlights the continued evolution of consultation and other educational offerings that help family medicine residency programs strive for excellence.
Family medicine was the first medical discipline to establish a peer consultation service.1 The Residency Assistance Program (RAP) was created with the collaborative vision of the American Academy of Family Physicians (AAFP), the Society of Teachers of Family Medicine, the American Board of Family Practice—now the American Board of Family Medicine (ABFM), and the Family Health Foundation of America (which evolved into the AAFP Foundation) via grant funding from the W.K. Kellogg Foundation. RAP was established in 1975 under the direction of Dr Thomas Stern to help residency programs meet the training requirements of the newly established discipline of family medicine.2
The reasons for consultation have evolved in parallel with changes in the discipline. In the 1970s and 1980s, most consultations requested were focused on helping new programs develop and meet accreditation requirements. In the 1990s, focus shifted to assisting programs in difficulty as well as programs that strived to achieve excellence. Unfavorable notification letters from the Accreditation Council for Graduate Medical Education (ACGME) Review Committee for Family Medicine often triggered consultations. Research from that period showed that family medicine residency programs that utilized RPS consultations reported improved ACGME outcomes with decreases in the total number of citations and increases in the length of their accreditation cycles,3 while programs that were forced to close in the early 2000s were less likely to have utilized RAP consultations,2 suggesting benefits of timely RPS consults.
In the late 2000s, RAP was rebranded as Residency Program Solutions (RPS), though its purpose and mission remained the same. Requests shifted again with heightened focus on value-based care and financial issues. By the late 2010s, more consultations were requested to assist a surge of new programs with financial pro formas, accreditation, and program development. Historically, most consult requests come from program directors,2 but others have come at the request of department chairs, medical school deans, or chief executive officers; the latter requests often are financial in nature. Demand for RPS consultations has remained steady over the past 50 years. Between 1975 and 2025, RAP and RPS conducted nearly 1,600 confidential consultations (email communication with RPS staff, October 28, 2025).
All RPS consultants have been seasoned practicing family physicians with experience as family medicine program directors or other institutional graduate medical education (GME) leaders. RPS consultants meet for training sessions four times a year to keep abreast of evolving issues in residency training and share best practices to ensure the most up-to-date recommendations during consultations. Over the years, consultants have paused their consultant roles if accepted to serve in a role with a potential conflict of interest, for example, serving on the ACGME Review Committee for Family Medicine.
The RPS consultant panel has expanded in recent years in both number of consultants and breadth of experience to help programs address issues in real time. New consultants are trained by participating in a site visit with a seasoned consultant colleague. All consultants share their perspectives as educators and program and/or departmental leaders with their consulting clients, providing pertinent knowledge of educational requirements and best practices in family medicine to help programs and administration navigate the complicated environment of GME. Since inception of the RAP/RPS program in 1975, 158 consultants have been appointed to serve their colleagues, with 19 currently serving in active consultant roles (Appendix A, list of consultants and directors). Over the years, many consultants have served for more than 10 years.
RPS CRITERIA FOR EXCELLENCE
Beginning in 1978, the RPS consultant team has developed a set of programmatic benchmarks known as the RPS Criteria for Excellence (CfE), designed to be a standard for programs desiring to go beyond meeting minimum ACGME requirements. Whereas the ACGME program requirements may be viewed as the floor that all programs must meet, the RPS CfE is intended to outline aspirational goals for programs. The RPS CfE are developed as a consensus product of the consultants’ experience from their own programs and conversations with other GME thought leaders, and informed by program consultations. Program directors have used the RPS CfE as a vital tool to advocate for additional support and resources to improve their programs.
To stay ahead of changing health care and educational environments, the RPS CfE manual has been regularly updated over 12 editions. Evidence suggests that early editions of the RPS CfE had some influence on updates to the ACGME family medicine requirements, regarding faculty research, pregnancy care/obstetrics, and duty hours.2 Changes to the RPS CfE can therefore be a harbinger for future ACGME requirement changes. To promote family medicine on the global stage, the RPS CfE was first translated into Spanish in 1982 and later into Russian (email communication with Center for the History of Family Medicine manager, February 10, 2026). As a result, the RPS CfE has made critical contributions to the development of the discipline.2
An artificial intelligence (AI) review (email communication with RPS staff, July 28, 2025) of revisions and additions to the RPS CfE from 2005 to 2025 reflects the evolution of changing program requirements, practice environments, and learning opportunities, highlighting the significant challenges that residency programs face (Table 1). Most recent updates to the RPS CfE in the 12th edition centered on structural barriers to care and recommendations for promoting health equity goals for populations served by programs. In addition, a section on understanding the role of AI in GME will likely be expanded in the 13th edition of RPS CfE, given the rapid development of this technology.
Year(s) |
Major themes |
2006–2011 |
Competency evaluation: Introduction of ACGME milestones, with emphasis on formative/summative evaluations, mapping competencies, and milestones |
2014 |
Shift in educational model: Redefining the locus of education from family medicine centers to family medicine practices using patient-centered medical home concepts and allowing broader continuity experiences beyond clinic walls |
2015–2017 |
Quality and safety: Emphasis on clinical learning environment review domains: patient safety, transitions of care, and well-being, and embedding continuous quality improvement processes |
2018–2019 |
Competency-based education: Expansion of entrustable professional activities and individualized education plans with suggestions for implementing direct observation and multirater feedback |
2020 |
Milestones 2.0: Recommendations on how to assess residents semiannually and align evaluations with updated subcompetencies |
2023 |
Clinic first model: Adoption of University of California–San Francisco clinic first model emphasizing ambulatory care as the core curriculum, with guidance about how to integrate resident scheduling, engagement, and work-life balance into teaching practices |
2023–2024 |
Advanced primary care models: Description of medicare access and CHIP reauthorization act and quality payment program frameworks with recommendations on how to teach value-based care, population health, and team-based models |
2025 |
Addressing bias, structural barriers to care, and health equity: Stronger emphasis on reducing inherent bias in resident and faculty recruitment, selection, and evaluation, and recommendations for promoting health equity goals for populations served by programs. Understanding the role of artificial intelligence |
The online RPS CfE was launched in March 2025 and has incorporated an AI chatbot, which allows programs to pose unique questions and includes information from the supporting documents referenced in many of the modules. Each of the 20 modules comes with a short self-assessment tool that allows programs to rate their own progress compared with the RPS CfE in that area and highlights opportunities for growth and improvement. The database includes contributions from other vetted family medicine resources, adding more timely best-practice solutions for emerging program challenges. Since inception of this residency assessment tool in 2025, 256 modules have been completed with the largest percentages being accessed for workforce mission (12%), competency-based medical education or CBME (11%), and resident and faculty well-being (9%; email communication with RPS staff, February 10, 2026). The tool can be accessed at https://www.aafp.org/residency-program-directors/residency-program-solutions/assessment-tool.
All family medicine residency programs need to meet the minimum program requirements set by ACGME and ABFM/AOBFP (American Osteopathic Board of Family Physicians). Both newly developed programs and established residency programs want to go beyond the minimum requirements to develop strong programs, determine program feasibility, and pursue excellence; these three goals have been the basis for all RPS consultations. When programs identify a concern and contact the RPS team in search of a consult, an intake is conducted and a call for consultants is shared with the consult team. Sometimes a specific consultant is requested for their particular expertise. Once a consultant agrees to take a consult, they communicate with the client to plan next steps.
Prior to scheduling an on-site or virtual visit, a previsit questionnaire is completed. Frequently, the focus of consultations has pivoted when viewed through the eyes of an experienced consultant, uncovering other issues simmering beneath the surface of the original consult request. The on-site consultation remains particularly high value for in- depth analysis of more complicated and extensive needs, and consultant recommendations can be used politically and strategically by the program director to achieve goals or obtain resources for their program.
In the mid-2000s, an increasing number of requests were for virtual consultation, a trend that accelerated during the COVID-19 pandemic and has persisted. Since 2021, 83% of consultations have been delivered virtually (email communication with RPS staff, September 8, 2025). The cost savings, easier scheduling, and lack of travel time are significant advantages of virtual consultations. Regardless of the total length of the consultation (eg, several hours or longitudinal over years), all clients receive timely written emails or reports until their consultation contract is complete.
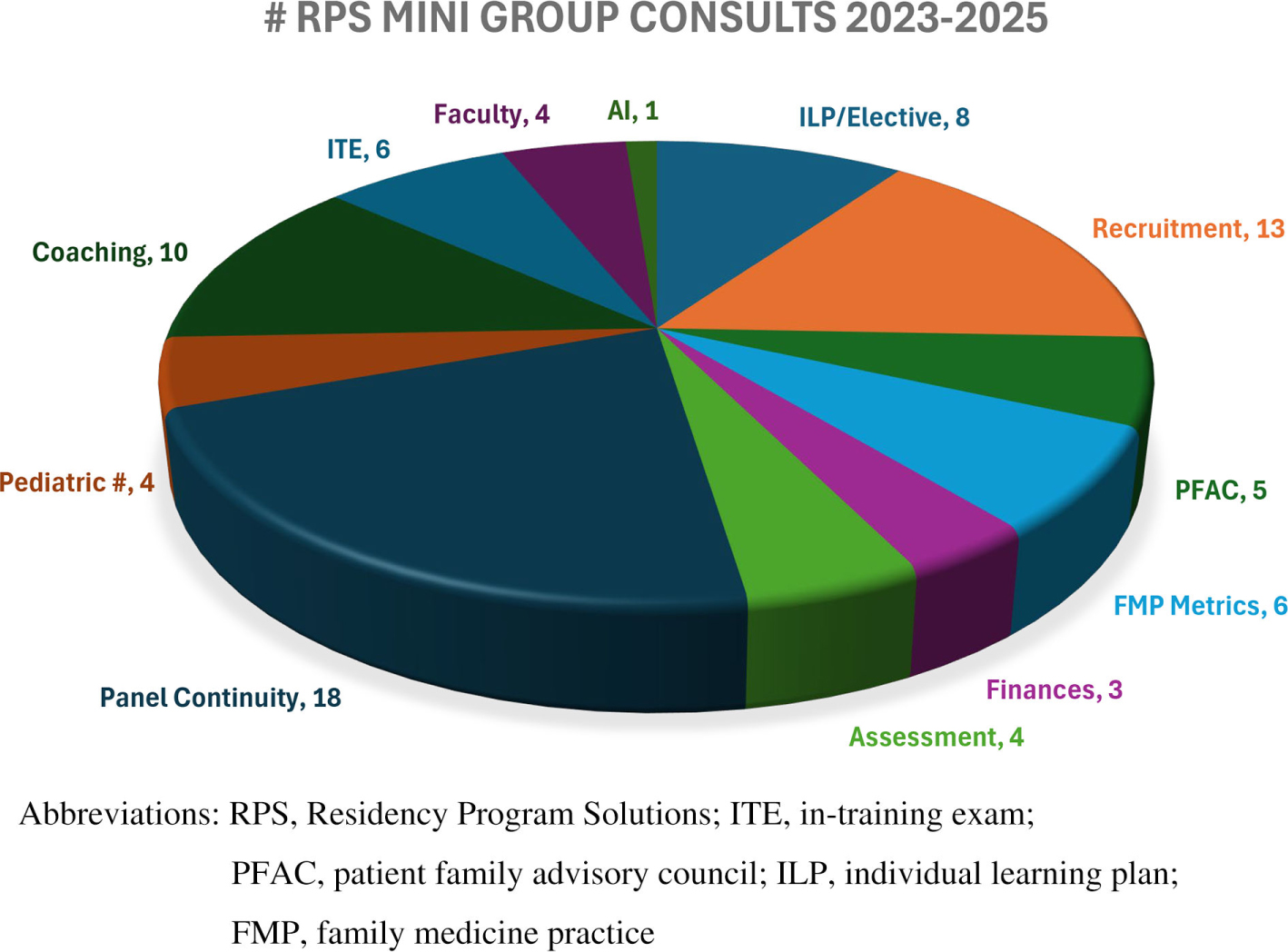
In recent years, newer consultation types (Table 2) have been developed. Express virtual consultations are problem-focused and are 90 or 180 minutes in length, allowing one consultant to address one focused problem for one program. Mini-group consultations (60 minutes) are also available, center around a particular topic, and are intended for multiple programs. Since they were first offered in 2022, RPS consultants have hosted 82 mini-group consultations on 26 different topics (Figure 1). These focused topics align with broader topics that are often the impetus for traditional single program consultations (Table 3). In-person 20 minute consults are available at the annual Residency Leadership Summit (RLS) conference. RPS now also provides a professional coaching service, designed as a longitudinal relationship with a new program director and experienced consultant to support the success of these emerging leaders.
Type of consult |
Focus |
Time |
Meeting style |
Traditional |
Varied (Table 1) |
20 hrs+ |
Virtual; on-site |
Express consult |
One topic; one program |
90 or 180 minutes |
Virtual |
RLS 20 minute consult |
One topic; one program |
20 minutes |
In person at RLS |
Mini group |
One topic; multiple programs |
60 minutes |
Virtual |
Longitudinal coaching |
Leader development |
Varies |
Virtual |
Traditional consult topics |
Mini-group consult topics (2023–2025) |
Strategy development |
|
Accreditation |
|
Mock site visits |
|
Culture and morale |
|
Curriculum innovation |
|
Faculty development and management |
Implementation of new faculty time requirement Faculty recruitment: finding, onboarding, and creating development plans Coaching with the end in mind—faculty development |
New program development |
|
Osteopathic recognition and added qualifications |
|
Overall program health and sustainability |
Engaging residents in learning: self-reflection and ILP development Engaging residents in feedback and growth Using available resources for ILP development |
Rural training |
|
Program management |
|
Teaching health centers |
|
Finance and financial issues |
|
Institutional and program application review |
|
Recruitment and retention |
Recruitment/match changes Program signaling and geographic preference Holistic review Anticipating 2024–2025 Match |
Family medicine practice management |
Residency practice metrics Team-based care integration Building resident volume in the family medicine practice Improving continuity rates Panel management Using AI for resident note documentation How to increase pediatrics in the FMP |
Site transitions |
|
ACGME requirements |
Patient advisory councils Measuring and reporting patient and provider continuity Options to meet ACGME requirements for care of sick children |
The partnership between RPS and the Technical Assistance Center Consortium (TAC) funded by Health Resources and Services Administration (HRSA) has been a major source of recent RPS consultations. In the past 5 years, RPS has conducted 48 new program consultations; all but one were new program consultations from the HRSA TAC (email with RPS staff, February 9, 2026). Many of these new programs were supported by RPS consultations during their application, accreditation, and recruitment processes or had collaborated with HRSA-assigned consultants via Teaching Health Center Program Development grants.
MEETING THE CONSULTATION NEEDS FOR RESIDENCY PROGRAMS
Achieving clarity about local GME finance options is often the primary question that clients bring to RPS consults, and requests for a pro forma budget are frequent. However, finance discussions always involve more than just finances and often include other issues: stakeholder commitment, leadership, the detailed structure of the residency curriculum, the operations of the clinical practice in the clinic and the hospitals, and the potential for successful recruitment and retention of faculty, program leaders, and residents. The integration of all these factors has made RPS consultations most valuable because most RPS peer consultants have encountered these issues to some degree in their own programs.
Programs that ask for advice on fixing nonfinancial problems often involve careful consideration of finance issues. While RPS consultants are neither accountants nor attorneys, RPS clients have found this consultative approach extremely helpful in negotiating the stakeholder relationships needed for the healthy operational and financial partnerships that are key to long-term GME viability. Recognition of this expertise by other medical specialties even has led to requests for RPS consultations outside of family medicine. On rare occasions, RPS has responded to requests from different specialties (rural internal medicine, rural psychiatry), fellowships (sports medicine), and those from the institutional and state GME level (email correspondence with Dr Lou Sanner, February 12, 2026).
The annual RLS offers educational content, meetings, and networking for residency leadership, faculty, and coordinators involved in the day-to-day workings of family medicine residency programs. Each year at RLS, multiple sessions are presented by RPS consultants on GME topics ranging from the struggling learner to the nuances of GME funding. For RLS 2026, nine RPS consultants copresented five workshops.4 Recent preconference workshops led by RPS consultants included the implementation of new ACGME family medicine program requirements (2022–2024), and RPS consultants attended the ABFM and Association of Family Medicine Residency Directors (AFMRD) Strengthening Outcomes and Assessment in Residency (SOAR) initiative (2023–2026). SOAR provides a way for programs to implement curricular improvement based on residency graduate outcomes.5
Over the years, some RPS consultants have served in a dual role as faculty at the National Institute for Program Director Development (NIPDD) fellowship, though NIPDD is an entirely separate program managed by AFMRD. Launched in 1994, NIPDD is a 9 month fellowship for new and aspiring program directors to hone their skills to become effective residency program directors.6 A study published in 2015 on the effectiveness of NIPDD graduates as program directors showed a positive relationship between completion of an NIPDD fellowship by the program director and higher board examination pass rates.7 For these reasons, RPS consultants often recommend that new program directors participate in NIPDD. To date, more than 1426 fellows have graduated from NIPDD, and capacity was expanded from 60 to 70 fellows per year starting in 2024 to address the growing number of new programs (email communication with AFMRD staff, February 9, 2026).
Most consultants are serving as program directors or academic leaders themselves and are fully engaged in meeting the needs of their own organizations. Growing demand for consultations creates additional strains on a finite personnel pool, which limits the number, scope of work, and available time that consultants have for RPS consultations. Like the discipline as a whole, where a substantial portion of family physicians are now at or past retirement age, the panel itself experiences retirement of consultants with unique funds of knowledge.
Programs in crisis may need immediate assistance, which further complicates scheduling. Persistent issues of funding instability for programs may prohibit hiring a consultant or pose challenges such as incurring added costs for needed faculty or experiences such as point-of-care ultrasound training to meet new requirements. The rapid expansion of programs also has created many new first-time program directors, who may need more support and faculty development for this complicated role. Family medicine has experienced a significant increase in both the number of programs (817 in 2025) and positions offered in the match (5,370 in 2025, which is 148 more positions than in 2024).8
RPS is responding to each of these challenges by expanding the consultant panel, diversifying both the type and manner of available consultations, and intensifying training in new areas of program support. Written feedback from recent consultations in the past few years has been sparse (N = 10), albeit positive. On a scale of 1 to 5, with one being the highest, the scores for ease in overall process (1), extent and quality (1), consultant recommendations (1.1), and value of presentation materials (1.1) were gathered (email communication RPS staff, February 12, 2026). Certainly, further efforts to fully assess and improve newer RPS consultation offerings are warranted and may be another opportunity to utilize AI.
RPS will need to further evolve to help the discipline of family medicine maintain its growth and momentum going forward in the face of significant headwinds. Programs will continue to experience financial pressures from multiple sources, threats to family medicine’s broad-scope training needs from consolidated health systems that traditionally have undervalued primary care, and ongoing challenges in recruiting medical students in the match. With the renewed ACGME focus on CBME and the core outcomes expected by ABFM for procedural sign-off in June 2027,9 RPS is preparing to respond with recommendations in the RPS CfE and anticipates further shared collaborations among the various stakeholder groups in family medicine.
Although AI tools such as ambient scribing may help today’s clinicians become more efficient, many are concerned that AI may jeopardize residents developing core decision-making skills and add yet more complexity to the practice and learning environment.10 Some programs are anticipated to consult RPS to help residency programs appropriately utilize AI as recommendations become clearer on how to best optimize AI from an educational perspective. Future graduates will care for patients in environments focused on population health registries, value-based programs, and AI-integrated practices—all areas that RPS will need to devise training and best practices in and update the RPS CfE accordingly.
A shortcoming of this paper was the difficulty in summarizing the specific details of more than 1,600 consultations conducted to date, largely because of documentation differences over the years, new consultation types, and the confidential nature that underlies all of them. A future recommendation to the RPS executive committee might be to define an ideal means of tracking consultations moving forward with an emphasis on consultation type, date, duration, who requested, cost, and other critical measures and outcomes. While a 50-year look back to see which of these metrics were documented historically is beyond the scope of this paper, that would no doubt provide a more complete assessment of the RPS program and allow for ongoing programmatic improvement.
In March 2025, the RPS program celebrated its 50th anniversary by welcoming past RPS and RAP directors to Kansas City to share their stories with current consultants during the RLS. The stories started with memories of the early developmental days of the program from early RAP leaders like Dr Dan Ostergaard and progressed to the challenges of present-day RPS consultations. Past directors raised the question, Can you tell the story of family medicine without RPS?
Over the past 50 years, residency programs have asked for help on a broad set of GME topics, and RPS consultations have evolved to meet these needs. RPS has provided wise guidance with each iteration of the CfE and consulting assistance for hundreds2 of individual programs—whether starting, struggling, or simply looking to improve. Unique in the health care consulting landscape, the perspective of having a peer-to-peer consultation from an experienced program director is a distinguishing factor of RPS and has allowed longitudinal relationship building with individual residency programs and leaders. Just as the discipline of family medicine is centered on the relationship with individual patients, RPS is focused on the needs of individual programs. As such, RPS has been an essential contributor to the story of family medicine over the last five decades and has made a substantial impact on the development of hundreds of family medicine programs and program directors, as well as the thousands of family physician graduates they have trained to date.
Authors are all Residency Program Solutions consultants or leaders.
References
-
-
-
-
American Academy of Family Physicians. Residency Leadership Summit 2026. Dallas, Texas. March 5-6, 2026.
-
Cole S, Fetter J, Oliver MG. Soaring to new heights: strengthening outcomes and assessment in residency..
Ann Fam Med. 2023;21(2):197–198. doi:10.1370/afm.2974
-
Pugno PA, Dornfest FD, Kahn NB Jr, Avant R. The National Institute for Program Director Development: a school for program directors.
J Am Board Fam Pract. 2002;15(3):209–213. https://www.jabfm.org/content/15/3/209
-
-
Mitchell D. AAFP News. Match day 2025: family medicine sets another milestone.
Ann Fam Med. 2025;23(3):275–276. doi:10.1370/afm.250230
-
-



There are no comments for this article.