
Family medicine leads in ethnic and racial diversity among specialties in the United States1,2 and can lead in addressing social needs to optimize health.3 In this special article, we describe the concept of an identity-driven career and its potential advantages. We also discuss how institutions and individuals can weaponize identity. For this article, we define underrepresented in medicine (URiM) individuals as those who identify as American Indian or Alaska Native, Black or African American, Latino, Hispanic or of Spanish Origin, Native Hawaiian or Pacific Islander, or Southeast Asian. While sexual and gender minorities do face some of the same challenges as those who identify as URiM, the cited literature does not include sexual and gender minorities in the URiM definition, which is a limitation of this piece. That is, however, an issue worthy of review in subsequent articles.
SPECIAL ARTICLES
Who Am I to Who I Am: The Identity-Driven Career
N. Ogechi Abara, MD | Yulsi L. Fernandez Montero, MD | Menerva Yole–Lobe, MPAS, PA-C | Brandis Belt, MD | Donna Baluchi, MLIS | Judy C. Washington, MD | José E. Rodríguez, MD
Fam Med. 2026;58(6):401-403.
DOI: 10.22454/FamMed.2026.805373
Underrepresented minorities in medicine often have experiences shaped by external perceptions of their identity. This article introduces the concept of an identity-driven career, where individuals intentionally integrate personal identity into professional roles, leveraging lived experiences to advance scholarship and service. We explore how identity enriches family medicine by fostering trust, addressing health inequities, and creating inclusive learning environments. However, leaders can weaponize identity and assign roles based on perceived identity. Individuals who experience this frequently may feel trapped in an identity-defined career. We propose strategies to mitigate these inequities, including institutional support for faculty autonomy, equitable distribution of diversity efforts, and incentives to encourage participation by faculty who are not underrepresented in medicine. Family medicine, with its undisputed leadership diversity, is uniquely positioned to lead this transformation. Identity-informed approaches can enhance research, education, and patient care while promoting equity across specialties.
What Is an Identity-Driven Career?
In the current political climate, where diversity, equity, and inclusion (DEI) work has been vilified and made illegal,4 creating language that accentuates the positive and negative uses of race/ethnic identities is necessary. For many of the authors, we have difficulty separating our identities from our professional work. To describe this phenomenon, we introduce the term identity-driven career. An identity-driven career is one in which the individual holds the reins, meaning that they are the principal architects of their own careers, using their identities to drive their careers in the direction they choose. They use their identity to imbue their work with their life experience. Their commitment to their identified community stems from a dedication to self. Their identity can lead individual faculty members to projects and academic products. In this case, URiM faculty can leverage their identity for advancement by using information and tools that are inherently familiar and readily available to them. Their identity drives their work and, as such, they are in control of how they use their race/ethnicity and other identities.
For many individuals in family medicine, and perhaps more so for URiM faculty, professional identity may be closely intertwined with personal or phenotypic identity. When approached mindfully, with appropriate boundaries, this intersection may offer unique opportunities in academic medicine. When driven by identity, physicians explore research questions from the inside, creating worthy scholarship from unique perspectives.
As family medicine educators teaching through an identity-driven lens, we can recognize blind spots in the medical curriculum, use our experiences to cultivate inclusive learning environments, and advocate for changes in admission processes to promote diversity and enhance learner outcomes. However, occasionally, those in identity-driven careers can find themselves in situations where identity is weaponized, leading to an identity-defined career.
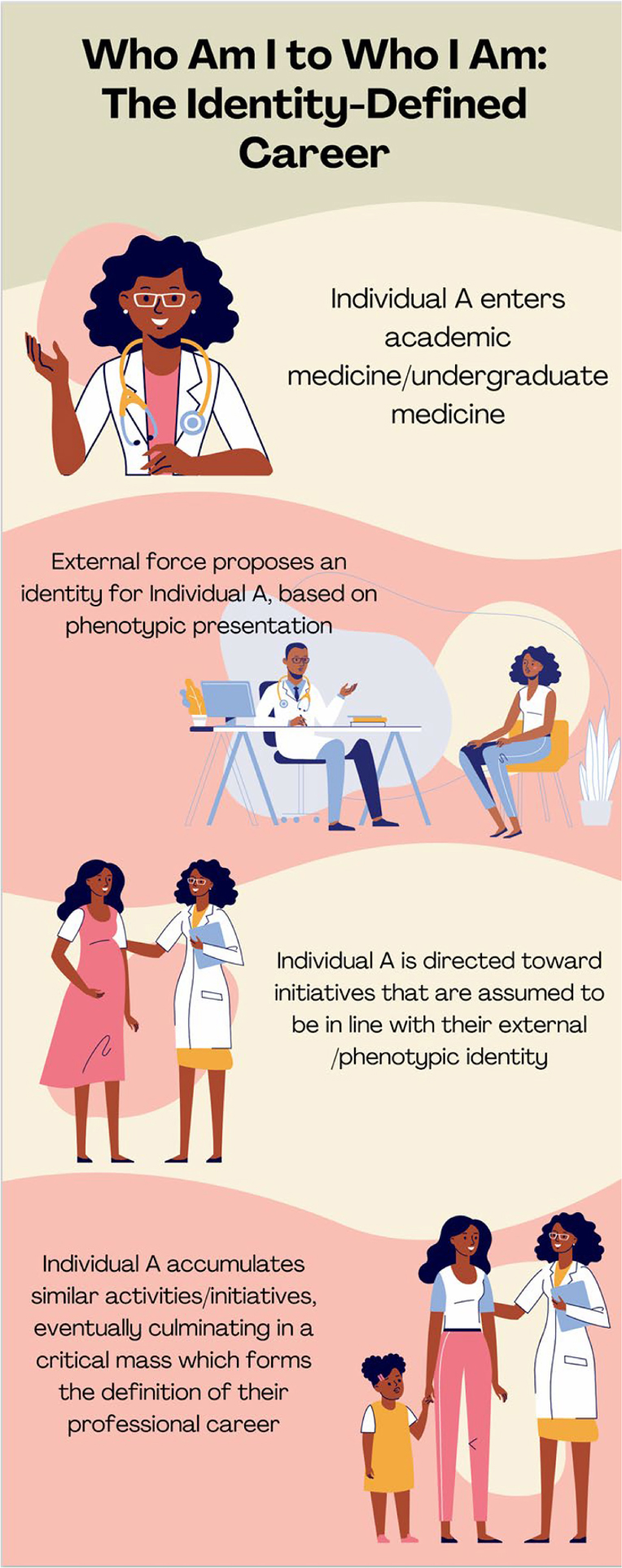
The Identity-Defined Career
Weaponization of identity occurs when faculty members are marginalized or isolated because of their external identity—typically described externally by an assumed cultural background, ethnicity, or social group based on their phenotypic characteristics.
For example, a new academic family physician perceived as female and Black may be assigned to lead diversity efforts or to head a free clinic in an underserved area. This situation can lead to pseudo-leadership, tokenism, and gate-blocking.5,6 Over time, she may be assigned similar duties, as her prior work reflects that this is within her skill set. She accumulates a body of work that is ultimately defined by her identity, as determined by someone else. She may feel compelled to espouse personally discordant values, which can lead to low satisfaction with her work in medicine and a departure from academic medicine (Figure 1).
A White man may be promoted early and placed in positions of power without proper qualifications, leading in turn to frustration and a mismatch between skills and product. In time, both of these physicians’ careers are impacted by external definitions of their identity. In both cases, we lose valuable perspectives in medicine. This outcome is reflective of a system rather than the inherent limitations of identity itself. Reframing identity as a source of agency rather than one of limitation can offer a different career trajectory.
From Identity-Defined to Identity-Driven
When identity is weaponized, URiM faculty can positively leverage their external identity by aligning with their own values and interests. Opportunities can arise when identity-driven expertise leads to significant contributions, such as publications, thereby enhancing academic portfolios. Recognizing how identity can beneficially shape careers is crucial.
To mitigate weaponization, URiM faculty should explore their interests freely rather than being assigned roles based on identity, such as serving on diversity committees or participating in community service. Leaders can encourage and incentivize non-URiM faculty to engage in diversity efforts, promoting inclusivity and reducing the burden on URiM faculty. In addition, leaders also can increase opportunities for URiM faculty to participate in research, promoting further exploration of their interests. To this end, family medicine can address some of the research challenges arising from identity-defined careers. Although not intended to be an exhaustive list, Table 1 describes how identity-driven actions can benefit medical specialties.
Challenges |
Strategies and solutions |
|---|---|
Lack of diversity in medical specialties limits the research questions. |
Retain and recruit more diverse residents and hire them as faculty. Institute a residency-based research curriculum with an emphasis on health equity. |
Committee service obligations are associated with diminished time for research opportunities. |
Ensure that committee assignments are distributed and provide opportunities for faculty serving on those committees to produce scholarly products from their work. |
Minority women tax increases community work and diminishes time for research.13 |
Be attentive to the needs of minority women, recognizing that the intersection of race and gender exponentially increases taxation. Ensure that citizenship assignments are equally distributed between women and nonwomen faculty.7 |
Minoritized faculty have less protected time for research and more clinical assignments than their non-URiM counterparts.8 |
Be mindful of clinical assignments and minoritized identity. Ensure that URiM faculty are promoted on time, ensuring that their clinical efforts remain consistent with those of their non-URiM peers. Equity audits are a helpful tool in this effort. |
Family medicine diversity may lead to a persistent racist perception of inferiority for URiM faculty and an inability to produce meaningful scholarship.8,9 |
Define diversity as a driver of excellence. Correct misperceptions and conflations of the family medicine specialty being inferior because it has the most diversity. Provide opportunities for research and distribute them equitably throughout the department. |
Abbreviation: URiM, underrepresented in medicine
Identity-defined actions can lead to increased clinical or committee work,10 often focused on diversity committees and mentorship, and leaving less time for the research work that leads to promotion.11 These activities, while valuable, are not as effective at advancing knowledge as research, given the evidence that quality research is central to academic medicine.12 These identity-defined activities have been described as the minority tax, the minority woman tax, or cultural taxation, which hinder career growth.13,14
Identity is a crucial construct in academic medicine. We have illustrated how it can be weaponized to limit opportunities, but we also have explored how leaning in to individual identity can be a career advantage and provide direction. Leaders and faculty can use these ideas as an impetus for research and scholarship, as well as an opportunity to improve equity across various identities within their institutions.
References
-
Analyzing physician workforce racial and ethnic composition physician specialties (part 1). Association of American Medical Colleges. Analysis in Brief. 2014;14(8).
-
Increasing family medicine faculty diversity still lags population trends. J Am Board Fam Med. 2017;30(1):100–103. doi:10.3122/jabfm.2017.01.160211
-
Addressing family medicine’s capacity to improve health equity through collaboration, accountability and coalition-building. Fam Med. 2019;51(2):198–203. doi:10.22454/FamMed.2019.921819
-
Goodbye DEI: Confessions of a Displaced Diversity Doctor. Rodríguez. 2025. https://doctorsonsocialmedia.com/book-goodbye-dei
-
Pseudoleadership as a contributor to the URM faculty experience. J Natl Med Assoc. 2023;115(1):S0027-9684(22)00181-X):73–76:. doi:10.1016/j.jnma.2022.11.003
-
Addressing the gate blocking of minority faculty. J Natl Med Assoc. 2021;113(5):S0027-9684(21)00070-5):517–521:. doi:10.1016/j.jnma.2021.04.002
-
Citizenship tasks and women physicians: additional woman tax in academic medicine? J Womens Health (Larchmt). 2021;30(7):935–943. doi:10.1089/jwh.2020.8482
-
Overcoming Mission Competition in Departments of Family Medicine. Fam Med. 2024;56(1):5–8. doi:10.22454/FamMed.2023.564792
-
Comments heard by US medical students about family practice. Fam Med. 2003;35(8):573–578. https://www.stfm.org/familymedicine/vol35issue8/Campos-Outcalt573
-
Are committee experiences of minoritized family medicine faculty part of the minority tax? a qualitative study. BMC Med Educ. 2023;23(1):862. doi:10.1186/s12909-023-04848-3
-
The diversity efforts disparity in academic medicine. Int J Environ Res Public Health. 2021;18(9):4529. doi:10.3390/ijerph18094529
-
More service or more advancement: Institutional barriers to academic success for women and women of color faculty at a large public comprehensive minority-serving state university. Journal of Diversity in Higher Education. 2022;15(3):365–379. doi:10.1037/dhe0000292
-
Abolish the minority woman tax! J Womens Health (Larchmt). 2021;30(7):914–915. doi:10.1089/jwh.2020.8884
-
Ethnic minority scholars, research, and mentoring: current and future issues. Educational Researcher. 1994;23(4):24–27. https://www.jstor.org/stable/1176259. doi:10.3102/0013189X023004024
Lead Author
N. Ogechi Abara, MD
Affiliations: Department of Family Medicine, Yuma Regional Medical Center, Yuma, AZ
Co-Authors
Yulsi L. Fernandez Montero, MD - David Geffen School of Medicine, University of California, Los Angeles
Menerva Yole–Lobe, MPAS, PA-C - Spencer Fox Eccles School of Medicine, University of Utah Health, Salt Lake City, UT
Brandis Belt, MD - Robert Wood Johnson Medical School, Rutgers University, Somerset, NJ
Donna Baluchi, MLIS - Spencer S. Eccles Health Sciences Library, University of Utah Health, Salt Lake City, UT
Judy C. Washington, MD - Atlantic Health, Morristown, NJ
José E. Rodríguez, MD - Meharry Medical College School of Medicine, Nashville, TN
Corresponding Author
José E. Rodríguez, MD
Correspondence: Department of Family and Community Medicine, Meharry Medical College, Nashville, TN
Email: jose.rodriguez@mmc.edu
Fetching other articles... 
Loading the comment form...
Submitting your comment...

There are no comments for this article.