Background and Objectives: Primary care continues to face pressure to improve clinical outcomes with limited resources. Point-of-care ultrasound (POCUS) offers potential value by improving diagnostic efficiency and procedural safety; yet early adoption in family medicine has been limited by faculty expertise, time constraints, and infrastructure barriers. In 2014, we developed a structured POCUS curriculum to address resident demand and programmatic gaps in family medicine training.
Methods: We implemented a 4-week required postgraduate year (PGY) one ultrasound rotation designed to function with limited faculty availability. The curriculum integrates asynchronous learning, simulation, supervised scanning with standardized patients and sonographers, structured image review, and competency assessment. Residents complete a defined number of scans in high-yield applications including cardiac, lung, abdominal aorta, venous thrombosis, musculoskeletal/soft tissue, and obstetric ultrasound. Longitudinal reinforcement was later added through quarterly hands-on sessions and a PGY-3 advanced ultrasound rotation emphasizing competency reassessment and near-peer teaching.
Results: Over 10 years, faculty capacity expanded primarily through training program graduates. An alumni survey (2015–2022 graduates; 58% response rate) demonstrated continued POCUS use in 44% of respondents, with higher utilization among rural physicians and billing rates exceeding national primary care averages. Common barriers included time constraints and equipment access, while skin/soft tissue, musculoskeletal, and procedural applications were most frequently used.
Conclusions: A scalable, longitudinal POCUS curriculum in family medicine is feasible despite limited protected faculty time. Tailoring training to anticipated practice settings, emphasizing ambulatory-relevant applications, and addressing workflow and billing education may improve long-term adoption and sustainability.
Primary care has for many years faced pressure to improve outcomes with fewer resources. Evidence from other specialties, such as emergency medicine, has shown that bedside imaging could reduce the need for costly diagnostic tests and improve procedural outcomes. When we initially considered implementing a curriculum in 2014, point-of-care ultrasound (POCUS) seemed well-suited to meet the challenge in primary care as well. Residents wanted training, but programs lacked experience in delivering POCUS training. These converging factors motivated us to develop a structured POCUS curriculum.
To meet these needs, we designed a 4-week ultrasound rotation for first-year residents that could run with limited faculty time and expertise. The curriculum blended asynchronous video modules, simulation, and supervised scanning with standardized patients, sonographers, and faculty preceptors, followed by structured image review. Residents completed a set number of examinations in high-yield applications, including cardiac, lung, aortic, venous thrombosis, soft tissue or musculoskeletal, and obstetric ultrasound. Tools were developed to assess knowledge, scanning skills, and attitudes, creating a model for family medicine residencies, with lessons learned over 10 years informing curriculum development and modification (Table 1).1
PGY level |
Curricular component |
Requirements/content |
Original or added |
PGY-1 |
Introductory module (start of residency) |
Intro to POCUS principles, image acquisition basics |
Original |
|
Ultrasound orientation (start of PGY-1 POCUS rotation) |
Individual hands-on orientation to required scans, equipment, logging system, and resources |
Original |
|
4-week required POCUS rotation |
POCUS applications
Limited echo (PLAX, PSAX, IVC) AAA screening Lung ultrasound (consolidation, pneumothorax, effusion, pulmonary edema) Limited 2-point DVT assessment Limited knee exam for effusion (added later) |
Original, except:
Knee exam—added Renal exam—removed |
POCUS experiences
Use of simulator for GYN and pregnancy scans (IUP confirmation, early dating, limited anatomy, fetal HR) Work with hospital sonographers (medical and obstetrical) and echo techs Regular gel rounds with ultrasound curricular lead Required online self-paced modules |
Original |
Rotation requirements
35 scans Pass POCUS OSCE (7 |
Original |
PGY-2 |
4-week procedure/ultrasound rotation |
Scheduled ultrasounds
|
Original |
PGY-3 |
2 week ultrasound requirement |
Required additional scanning block added to curriculum |
Added later |
All years |
Ongoing didactic integration |
Ultrasound topics integrated monthly |
Original |
|
Quarterly open scanning sessions |
Opportunity for continuous scanning and logging during didactics |
Added later |
|
Graduation requirement |
|
Original |
Observations among alumni |
Practice in rural setting |
Frequency of POCUS use |
P=.046 |
Receiving ultrasound experience in medical school |
Frequency of POCUS use |
P=.350 |
# POCUS exams done in residency |
Frequency of POCUS use |
P=.638 |
Barrier: lack of equipment |
Lower frequency of POCUS use |
P=.006 |
Barrier: lack of time |
Lower frequency of POCUS use |
P=.131 |
PRIVILEGED BUT STRETCHED: FACULTY CAPACITY IN POCUS
Our inaugural POCUS faculty had significant ultrasound training and experience. When our health system established criteria for POCUS providers in 2019, these faculty were able to obtain privileges. Faculty without prior training were required to take POCUS continuous medical education and log 150 proctored exams for full POCUS privileges. Despite strong efforts and interest, this requirement proved too time-consuming for most faculty to achieve without dedicated, funded time. Most of our success in expanding POCUS-trained faculty has been in hiring our own graduates. Currently, we have 15 faculty privileged in some form of POCUS, eight trained via our curriculum, three as inaugural POCUS faculty, and four from outside institutions.
Aside from acquiring POCUS training faculty, faculty availability has been a challenge. Our initial POCUS curriculum included a 4-week PGY-1 rotation, which utilized a diverse array of ultrasound educators, including general sonographers, obstetric sonographers, and echocardiogram technicians.1 In addition, our POCUS program’s initial launch was aided by the allotment of a half-day per week of dedicated faculty time, paid for by our School of Medicine’s Ultrasound Institute. This time was invaluable during the initial years of our POCUS program, but the funding was sunsetted in 2022. Since that time, our ultrasound faculty have managed to teach the most time-intensive components of this PGY-1 rotation (including the hands-on orientation, weekly supervised scanning sessions, and the end-of-rotation objective structured clinical examination) by double dipping—that is, utilizing administrative time and low-volume call days. Preserving the weekly supervised scanning sessions (gel rounds) has been particularly challenging, given time pressures and competing commitments for both faculty and the rotating PGY-1 residents. In the absence of protected faculty time, some curricular components have required adaptation, with image review sessions adopting a more flexible, resident-focused format. Image review is now commonly conducted during gel rounds or in smaller informal sessions with PGY-1 residents, allowing timely feedback while maintaining continuity of supervision. While the curriculum has been sustained through distributed faculty effort and workflow integration, renewed institutional investment in protected time would enhance opportunities for innovation and future program development.
FROM INTEREST TO EXPERTISE: SUSTAINING RESIDENT BUY-IN
One of the challenges throughout the continued development of our curriculum has been keeping continuity of ultrasound training throughout residency. Our PGY-1 residents complete a 4-week ultrasound rotation, but those without significant interest are often weak in ongoing self-directed learning and practice. Variable rotation training sites also has led to large gaps of time our learners had away from POCUS, leading to attrition. To further enhance the longitudinal experience, we added quarterly ultrasound didactic sessions with standardized patients in our clinic. These sessions have direct supervision by POCUS faculty and count toward total scan requirements. We also developed a 2 week ultrasound rotation completed in PGY-3 with dedicated time to complete required scans and the expectation to mentor the PGY-1 and PGY-2 rotators. This rotation has allowed faculty to reevaluate resident skills and ensure that residents have completed the required scans for graduation, evaluate competency for future practice, and increase bedside teaching in a way that off-loads teaching responsibilities of faculty.
EQUIPMENT, BILLING, AND WORKFLOW INTEGRATION
Additional challenges have been the issues of equipment and billing.2,3 Within the hospital setting, ultrasound machines are available in the emergency department, labor and delivery floor, medical-surgical floor, and intensive care unit. Obtaining machines for the ambulatory clinic has required concerted efforts because of the high dollar capital expense with an uncertain pathway for revenue generation. The first generation of machines came to our clinic through an educational grant, but scans using this device were not approved for medical decision-making or billing. As we worked with the medical system to use billing codes for these limited ultrasound scans, we had to have a way to upload images into an electronic record to justify the bills. Initially, this data storage was done through POCUS specialized software, which was later integrated into the electronic medical record. Fortunately, this process became more streamlined as our institution moved to a common interdepartmental workflow.
More cost-effective, handheld devices came later, allowing for easier acquisition. However, we have found that larger, laptop-style models still outperform handheld devices for educational purposes because of their larger screens and more nuanced capabilities.
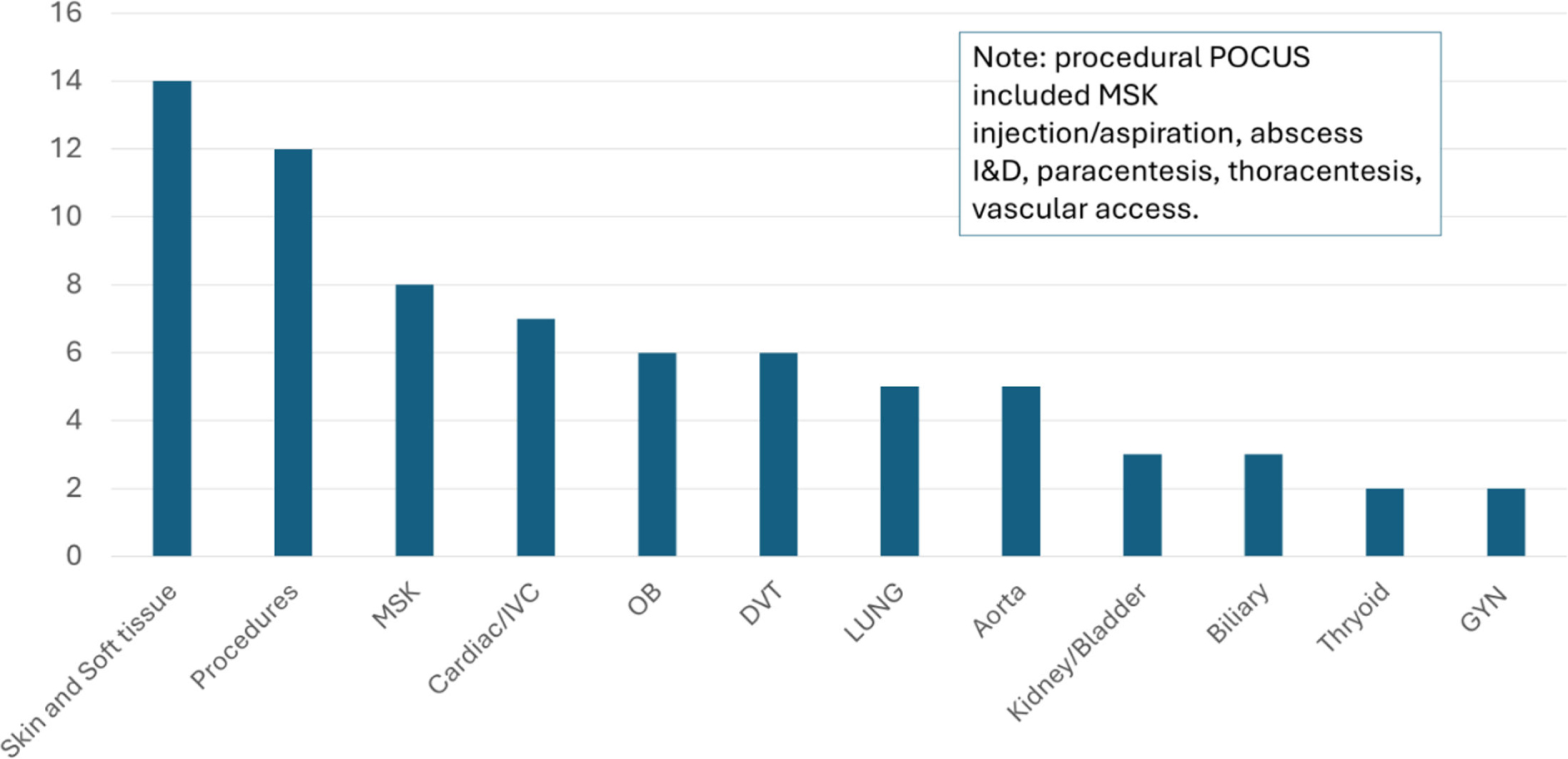
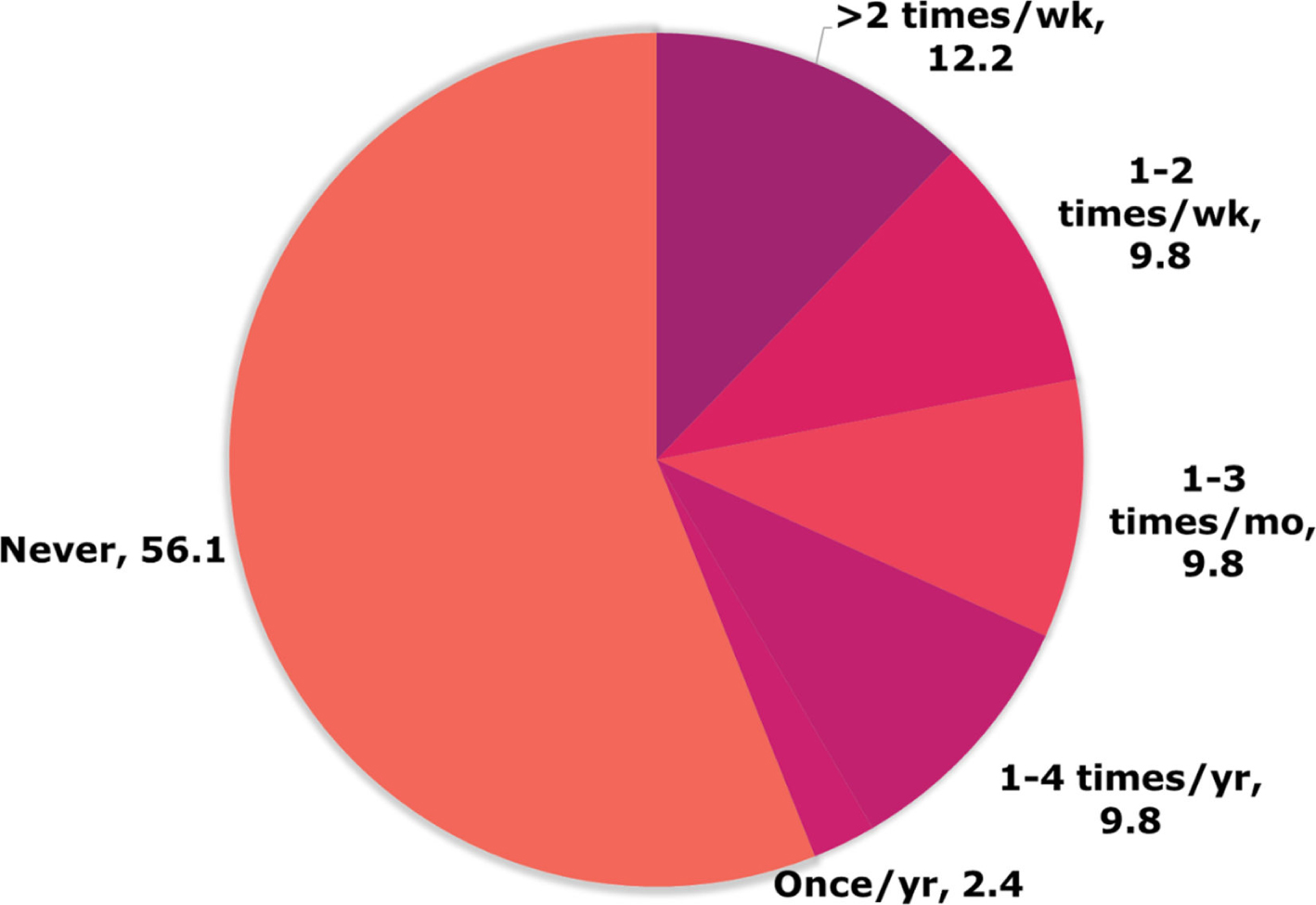
In 2023, we surveyed alumni who graduated between 2015 and 2022 from the Prisma Health Midlands Family Medicine Residency (PHMFMR) to evaluate their POCUS use, barriers, and perceptions. This project was reviewed by the Prisma Health Institutional Review Board (IRB) and determined to be exempt from IRB review. Seventy-one alumni were surveyed, with 41 responses (Figure 1). Alumni from PHMFMR were more likely to bill for POCUS (19.5%) compared to the national average among primary care physicians (9.5%).4 Alumni who reported practicing in a rural area were significantly more likely to use POCUS (P = 0.046). Among alumni who did not continue to utilize POCUS, the most common barriers noted were the lack of equipment and time (P = 0.006). Of the respondents, 5.9% reported that they did not feel that they had received proper training, and 7.9% listed difficulty in financial reimbursement. POCUS was most utilized for skin and soft tissue, musculoskeletal, and procedural applications (Figure 2). The results of this survey, though not powered for statistical significance, suggest that the POCUS curriculum did influence POCUS use among graduates and underscore the fact that the variable practice environments, time, and available equipment have large impacts on regular use. This information could be used to direct training toward more commonly used exams in the ambulatory setting, as well as in coaching trainees toward implementation and compliant billing practices to increase confidence.
CONTEXT MATTERS: POCUS TRAINING in FAMILY MEDICINE
POCUS education in family medicine faces numerous challenges. Many of these—including the need for capable faculty, limited faculty availability, and barriers related to technology acquisition and integration—are not unique to family medicine. However, the breadth and variability inherent to family medicine training introduce distinct challenges. Residents frequently rotate through diverse clinical environments where POCUS may not be readily available, making regular longitudinal touchpoints essential to reinforce skills. Additionally, the wide range of practice models, settings, and clinical demands within family medicine suggests that a one-size-fits-all approach to POCUS education may be insufficient. Our data indicate that an emphasis on skin and soft tissue imaging, musculoskeletal applications, and procedural guidance may be particularly valuable for residents pursuing traditional ambulatory practice, whereas those planning to practice in rural settings may benefit from a broader POCUS skill set. Additional educational focus on best practices in billing, compliance, and workflow may also result in more confident and capable family medicine POCUS graduates.
References
-
Bornemann P. Assessment of a Novel Point-of-Care Ultrasound Curriculum’s Effect on Competency Measures in Family Medicine Graduate Medical Education.
J Ultrasound Med. 2017;36(6):1205–1211. doi:10.7863/ultra.16.05002
-
Capizzano JN, O’Dwyer M-C, Furst W, et al. Current State of Point-of-Care Ultrasound Use Within Family Medicine.
J Am Board Fam Med. 2022;35(4):809–813. doi:10.3122/jabfm.2022.04.220019
-
Hall JWW, Holman H, Barreto TW, et al. Point-of-Care Ultrasound in Family Medicine Residencies 5-Year Update: A CERA Study.
Fam Med. 2020;52(7):505–511. doi:10.22454/FamMed.2020.223648
-
Shen-Wagner J. Family Medicine Billing for Point-of-Care Ultrasound (POCUS).
J Am Board Fam Med. 2021;34(4):856–858. doi:10.3122/jabfm.2021.04.210187



There are no comments for this article.