Introduction: Physicians need to foster healthy relationships with patients to optimize care, with time constraints and workloads being barriers. Studies have shown the importance of first impressions, which are influenced by attire. Studies of physician attire have previously been conducted in metropolitan populations. This study’s goal was to investigate patient preferences for physician attire among rural populations.
Methods: A cross-sectional study of patients was conducted in waiting rooms of five ambulatory clinics dispersed throughout rural northern Michigan. Anonymous surveys contained a series of photos of a male and a female physician, with photos within the series differing only by apparel. Participants indicated which male and female physician they would prefer in various scenarios. Participants provided demographic information and indicated their own physician’s usual attire. Responses were analyzed using comparative statistics and logistic regression.
Results: Survey response rate was 78% (92/118). Similar to metropolitan studies, patients preferred professional attire including white coat in almost all scenarios. For most scenarios, participants preferred professional attire for both male and female physicians, however respondents were more tolerant of casual attire for female physicians. Older participants and those whose physician dressed casually tended to be more tolerant of casual attire. Patients preferred surgical attire only in emergency situations.
Conclusions: This study of a rural population showed a clear preference for professional physician attire. In general, rural physicians should consider wearing professional attire with white coat in order to best meet patient expectations. Further investigations are needed to enhance the generalizability of study findings.
Physicians need to establish rapport, gain trust, and provide quality care, all within a busy environment. In busy settings it is often imperative for physicians to make a good impression quickly. Appearance plays a role in the formation of an observer’s initial opinion,1 especially in professional settings.2 Previous studies have shown that physician attire is an important factor for patient trust, confidence, and satisfaction.3-6 Importantly, patients are more likely to disclose personal information and incorporate physician recommendations when they view physicians as competent, supportive, and respectful.7
Previous research has shown that patients generally prefer traditional attire for physicians, specifically a white coat.8-17 These studies were conducted in metropolitan populations however. Values and perceptions of rural patients may differ from their urban counterparts. As 20% of the nation’s population is rural, understanding rural preferences may help interested physicians better meet patients’ expectations.
The goal of this study is to determine whether views of rural patients toward physician attire differ from those of urban populations. To do this, rural patients in northern Michigan were surveyed regarding preferences and attitudes toward physician attire.
Researchers conducted a cross sectional study utilizing a previously validated and published survey on physician attire.6 The surveys contained a series of pictures depicting both a female and male doctor. The only difference between each series of photos was the attire the two physicians wore; facial expressions, hairstyle, stance, and jewelry were identical. The pictures contained four different categories of attire for each gender: business, professional, surgical, and casual. Table 1 describes each category.
The surveys contained 14 questions for both the female and the male set of photos. Examples of survey questions included “Which would you prefer to be your family doctor? Which of these doctors would you trust the most? Which of these doctors would you expect to be more responsible?”. For all questions, patients were instructed to mark the box under the picture that corresponded to their preference. Participants also completed demographic information and indicated which type of attire their personal physician typically wore.
Surveys were distributed during a three-month period in 2014 to outpatient clinics in rural northern Michigan, including two family medicine clinics, an internal medicine clinic, a general surgery clinic, and an OBGYN clinic. Employees were instructed to distribute surveys to adult clients in the waiting room randomly throughout the workday. Completed surveys were collected anonymously, and response rate was calculated based on the number of surveys distributed and those returned. All surveys clearly marked by patients were used in the analysis.
Results were analyzed using chi-square or Fisher’s exact test as appropriate. The responses for female physician and male physician attire for each scenario were compared using the McNemar-Bowker test. Binary logistic regression was used to compare the contribution of significant variables. Data was compared using SPSS Statistical Software Version 23, with significance for all analyses set at p<0.05. The study was approved by Munson Medical Center’s IRB.
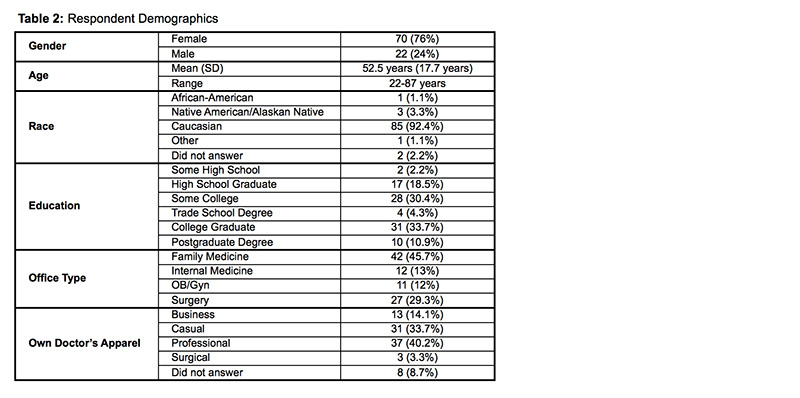
A total of 118 surveys were distributed, with 92 surveys returned (response rate 78%). Respondents were 76% female. The majority of participants were Caucasian (92.4%), which is reflective of the region’s population. Of study participants, 49% had a degree higher than a high school diploma. Table 2 describes participant demographics.
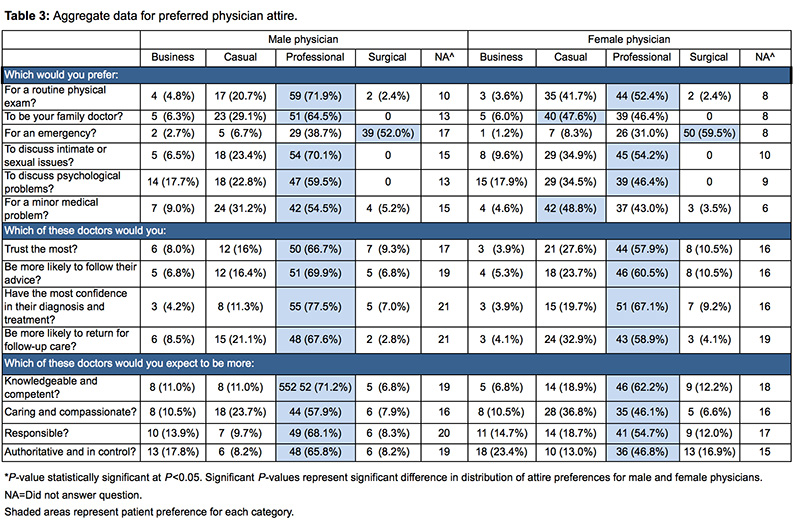
Rural patient preferences for physician attire for male and female physicians are presented in Table 3. For nearly all scenarios, participants preferred professional attire for both male and female physicians, but where differences existed, respondents tended to be more tolerant of casual attire for female physicians. A notable exception to this preference for professional attire was surgical attire in emergency situations for both male and female physicians. As professional attire was preferred in nearly all situations, professional attire was compared to a grouping of all other attire categories for the remainder of the analysis.
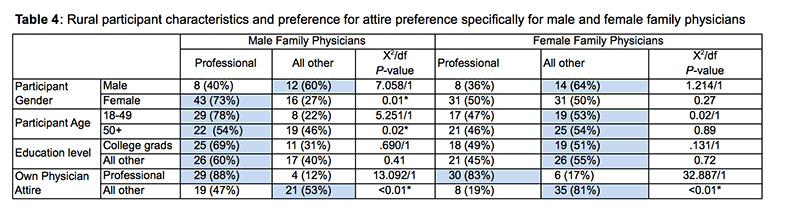
Preference of attire for family physicians was used to comparatively analyze results based on survey participant demographics. Results of preferred attire for male and female family physicians were compared by participants’ gender, age (18-49 vs. 50+), educational level (college graduates vs. all other), and own physician attire (professional vs. all others). Results are shown in Table 4. There was a trend toward preferring professional attire for male family physicians among most groups, with older male participants and those whose physicians dressed more casually showing some tolerance of casual attire. Interestingly, most groups showed a slight preference for casual attire for female family physicians, with the exception of patients whose physicians dressed professionally. Logistic regression was performed to assess the impact of participant demographic factors on preference for male family physician attire. The model included three independent variables (age of participant, gender of participant, and attire of participant’s physician). The full model, including all variables, was statistically significant (X2(3, N=72)=22.83, P<0.01). Age and the attire worn by the participant’s physician made unique statistically significant contributions to the model, with the strongest predictor of preferring professional attire for male family physicians being if the participant’s physician dressed professionally (odds ratio of 11.8), followed by age less than 50 years (odds ratio of 4.0).
In this study focused on rural populations, respondents overall preferred professional attire with white coats for physicians. The results of this study are similar to previously conducted studies in metropolitan areas, most of which showed a similar predilection for physicians to dress professionally with white coats.
Although rural patients preferred professional physician attire, there was a higher tolerance for casual attire compared to previous metropolitan-based studies.6 This trend was strongest among patients who indicated their own physicians dressed casually. It may be that patients become accustomed to the appearance of physicians in their community, affecting expectations. In addition, rural populations may have a more relaxed view of society and may place less emphasis on attire, resulting in more tolerance for casual apparel. Physicians are often well known in small communities, and familiarity may break down traditional hierarchal separations that may exist in larger communities. Regardless, despite this trend toward some tolerance for casual apparel, in most situations rural patients expressed a preference for physicians to dress professionally.
The study is limited in generalizability in that all respondents were surveyed in rural northern Michigan. Future studies could focus on diverse geographical locations and include more ethnic diversity. Study was also limited by the use of self-reported data rather than observing actual behavior. The research methods used in this study relied on a two dimensional view that did not delve into other important attitudinal or experiential factors that contribute to a person’s perception, which could have impacted results. It is also unclear whether a physician’s attire remains important once a relationship is established. A final important limitation of the study is that the female series of photos depicted a female physician in surgical attire, a skirt, or a dress. This was true even with casual attire, which was a casual appearing denim dress. These photographs were used to allow comparison to the previously published metropolitan-based study, but may be why participants were more tolerant of casual attire specifically for the female physician when compared to the male. Due to this limitation, logistic regression comparing participant demographics and attire preference was performed using only the male physician model.
In conclusion, this study of a rural population demonstrated a preference for professional physician attire. In general, rural physicians should consider wearing professional attire with white coat in order to best meet patient expectations, especially when relying on a first impression. Further studies to increase generalizability of findings are needed.
References
- Naumann LP, Vazire S, Rentfrow PJ, Gosling SD. Personality judgments based on physical appearance. Pers Soc Psychol Bull. 2009;35(12):1661-1671. https://doi.org/10.1177/0146167209346309
- Easterling CR, Leslie JE, Jones MA. Perceived importance and usage of dress codes among organizations that market professional services. Public Pers Manage. 1992;21(2):211-219. https://doi.org/10.1177/009102609202100208
- Chung H, Lee H, Chang DS, et al. Doctor’s attire influences perceived empathy in the patient-doctor relationship. Patient Educ Couns. 2012;89(3):387-391. https://doi.org/10.1016/j.pec.2012.02.017
- Bianchi MT. Desiderata or dogma: what the evidence reveals about physician attire. J Gen Intern Med. 2008;23(5):641-643. https://doi.org/10.1007/s11606-008-0546-8
- Brandt LJ. On the value of an old dress code in the new millennium. Arch Intern Med. 2003;163(11):1277-1281. https://doi.org/10.1001/archinte.163.11.1277
- Rehman SU, Nietert PJ, Cope DW, Kilpatrick AO. What to wear today? Effect of doctor’s attire on the trust and confidence of patients. Am J Med. 2005;118(11):1279-1286. https://doi.org/10.1016/j.amjmed.2005.04.026
- Jin J, Sklar GE, Min Sen Oh V, Chuen Li S. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther Clin Risk Manag. 2008;4(1):269-286. https://doi.org/10.2147/TCRM.S1458
- Gjerdingen DK, Simpson DE. Physicians’ attitudes about their professional appearance. Fam Pract Res J. 1989;9(1):57-64.
- Gjerdingen DK, Simpson DE, Titus SL. Patients’ and physicians’ attitudes regarding the physician’s professional appearance. Arch Intern Med. 1987;147(7):1209-1212. https://doi.org/10.1001/archinte.1987.00370070023002
- Gjerdingen DK, Thorpe W, List-Holt P. The physician’s appearance and professionalism. Resid Staff Physician. 1990;36(1):65-66, 71.
- McKinstry B, Wang JX. Putting on the style: what patients think of the way their doctor dresses. Br J Gen Pract. 1991;41(348):270, 275-278. https://doi.org/10.3399/bjgp08X264036
- McNaughton-Filion L, Chen JS, Norton PG. The physician’s appearance. Fam Med. 1991;23(3):208-211.
- Keenum AJ, Wallace LS, Stevens AR. Patients’ attitudes regarding physical characteristics of family practice physicians. South Med J. 2003;96(12):1190-1194. https://doi.org/10.1097/01.SMJ.0000077011.58103.C1
- Dover S. Glasgow patients’ attitude to doctors’ dress and appearance. Health Bull (Edinb). 1991;49(6):293-296.
- Cha A, Hecht BR, Nelson K, Hopkins MP. Resident physician attire: does it make a difference to our patients? Am J Obstet Gynecol. 2004;190(5):1484-1488. https://doi.org/10.1016/j.ajog.2004.02.022
- Au S, Khandwala F, Stelfox HT. Physician attire in the intensive care unit and patient family perceptions of physician professional characteristics. JAMA Intern Med. 2013;173(6):465-467. https://doi.org/10.1001/jamainternmed.2013.2732
- Petrilli CM, Mack M, Petrilli JJ, Hickner A, Saint S, Chopra V. Understanding the role of physician attire on patient perceptions: a systematic review of the literature—targeting attire to improve likelihood of rapport (TAILOR) investigators. BMJ Open. 2015;5(1):e006578. https://doi.org/10.1136/bmjopen-2014-006578