Introduction: Adolescents are often thought of as a healthy population, however, they routinely engage in high-risk behaviors that can lead to health problems. Medical students designed MiHealth, a program in which medical students teach health lessons in the high school classroom to help address these behaviors.
Methods: A series of six lessons were created and implemented in the classroom for this pilot study focused on sexual health, intimate partner violence, mental health, smoking and marijuana, nutrition, and physical fitness. High school students in grades nine through twelve at a public high school in southeast Michigan receiving the MiHealth curriculum (N=52) or the standard health education curriculum (N=61) were surveyed on health knowledge, attitudes, and intentions before and after the program.
Results: Six weeks after program completion, high school students who received the MiHealth curriculum scored significantly higher on health knowledge (P=0.007), and expressed significantly healthier attitudes and intentions toward risk behavior compared to controls (P=0.025). Among individual themes, MiHealth resulted in significant knowledge gains in sexual health (P=0.001) and mental health (P<0.025), and significantly healthier attitudes regarding sexual health (P=0.047), nutrition (P=0.040), and smoking and marijuana (P=0.012).
Conclusions: MiHealth demonstrated promising improvements in health knowledge retention and attitude changes in adolescents 6 weeks after program completion. An interactive curriculum targeting key adolescent health topics given by near-peer medical student educators may provide benefits beyond traditional high school health curricula.
Adolescents are often thought of as a healthy population, however, they routinely engage in behaviors that can lead to health problems.1-5 Many US teens engage in behaviors such as smoking, unprotected sexual intercourse, or physical inactivity.6
High-risk behavior may be preventable with appropriate intervention. Well-implemented sexual health education, for example, has been shown to reduce risk by delaying sexual debut and increasing condom use.7 Many schools nationwide lag in providing comprehensive, quality health curricula, and the lack of universal, high-quality health education leaves teens vulnerable to making uninformed, potentially dangerous choices.8
Medical students at the University of Michigan Medical School (UMMS) reviewed local data on adolescent risk behavior to better understand the prevalence of these behaviors in their community, and identified potential opportunities for intervention. A program, MiHealth, was created in which medical students serve as instructors in the high school classroom. The pilot year consisted of six lessons delivered to two classes at a local high school, emphasizing topics related to high-risk behaviors prevalent among local teens. This study aims to assess MiHealth’s impact on high school students’ knowledge, attitudes, and intentions related to health and risk behavior.
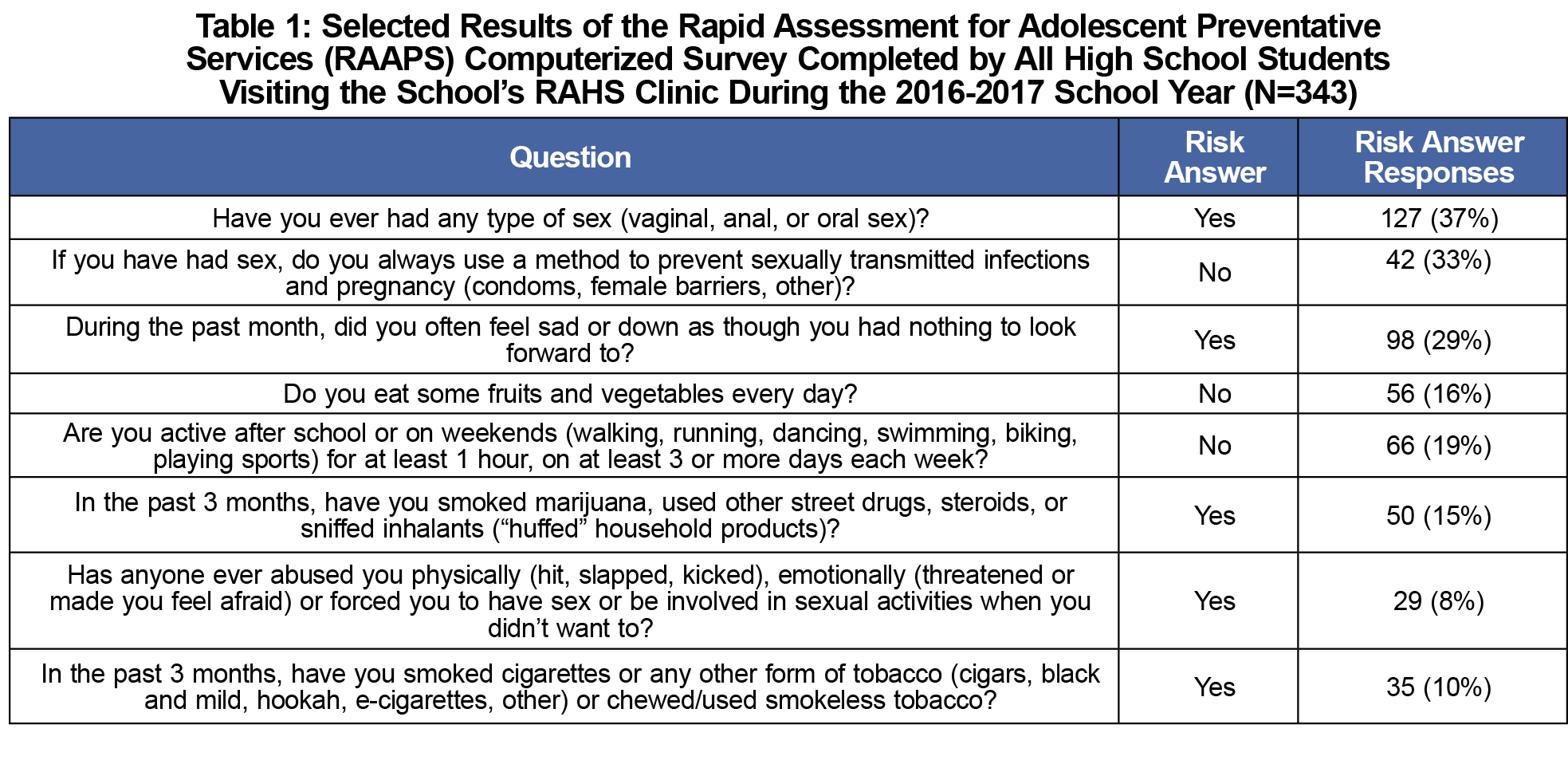
A high school in Washtenaw County, MI was chosen as the pilot site due to its population of economically disadvantaged students (41% received free or reduced lunch in 2016-2017)9 and its participation in the Regional Alliance for Healthy Schools (RAHS), a network of school-based clinics run by Michigan Medicine (MM). The school requires all students to take a one-semester health course, offered during four class periods each semester. Baseline risk behavior of the student body was gathered through the Rapid Assessment for Adolescent Preventive Services (RAAPS), a survey for high-risk behaviors completed yearly by each student visiting the school’s RAHS clinic (Table 1).
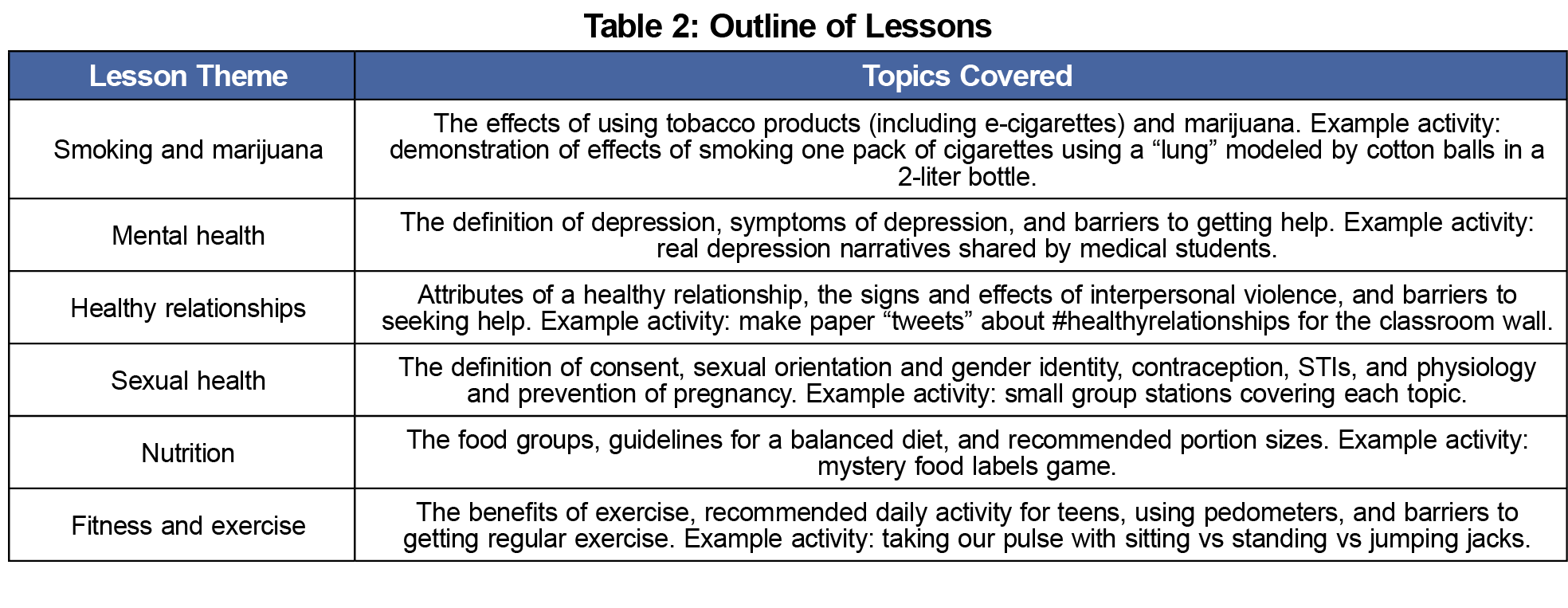
Using RAAPS-identified areas of highest risk behavior, medical students created six 60-minute lessons with the themes sexual health, smoking and drugs, mental health, healthy relationships, nutrition, and fitness and exercise. Lessons focused on teaching through interactive, engaging learning activities (Table 2).
Over 2 months in early 2016, groups of four to six medical students administered the MiHealth curriculum to two of the four high school health classes. The remaining two health classes served as the control group and received only the standard high school health curriculum that incorporates units entitled Making Healthy Choices, Managing Stress, Mental Health, Building Healthy Relationships, Eating Well, Fitness and Health, and Protecting Oneself and Others.
Evaluation of MiHealth was granted “not regulated” status by the MM Institutional Review Board as a quality improvement initiative. A 44-item questionnaire was created based on lesson learning objectives.10 The anonymous questionnaire was administered to all four health classes in the week directly preceding the program (preprogram) and 6 weeks after program completion (postprogram). All questions used a 5-point Likert scale (1=strongly disagree, 5=strongly agree). For analysis, responses were coded so that 5 always represented the most healthy or least risky answer, eg a response of 1 (strongly disagree) to the statement, “depression can be controlled through willpower,” would be recoded as a 5 for analysis. Mean composite and lesson-specific scores were calculated for MiHealth and control classes, for knowledge items and for items assessing attitudes and intentions. These were compared at preprogram and postprogram time points. Due to questionnaire anonymity, unpaired t-tests were utilized; significance was set at P<0.05.
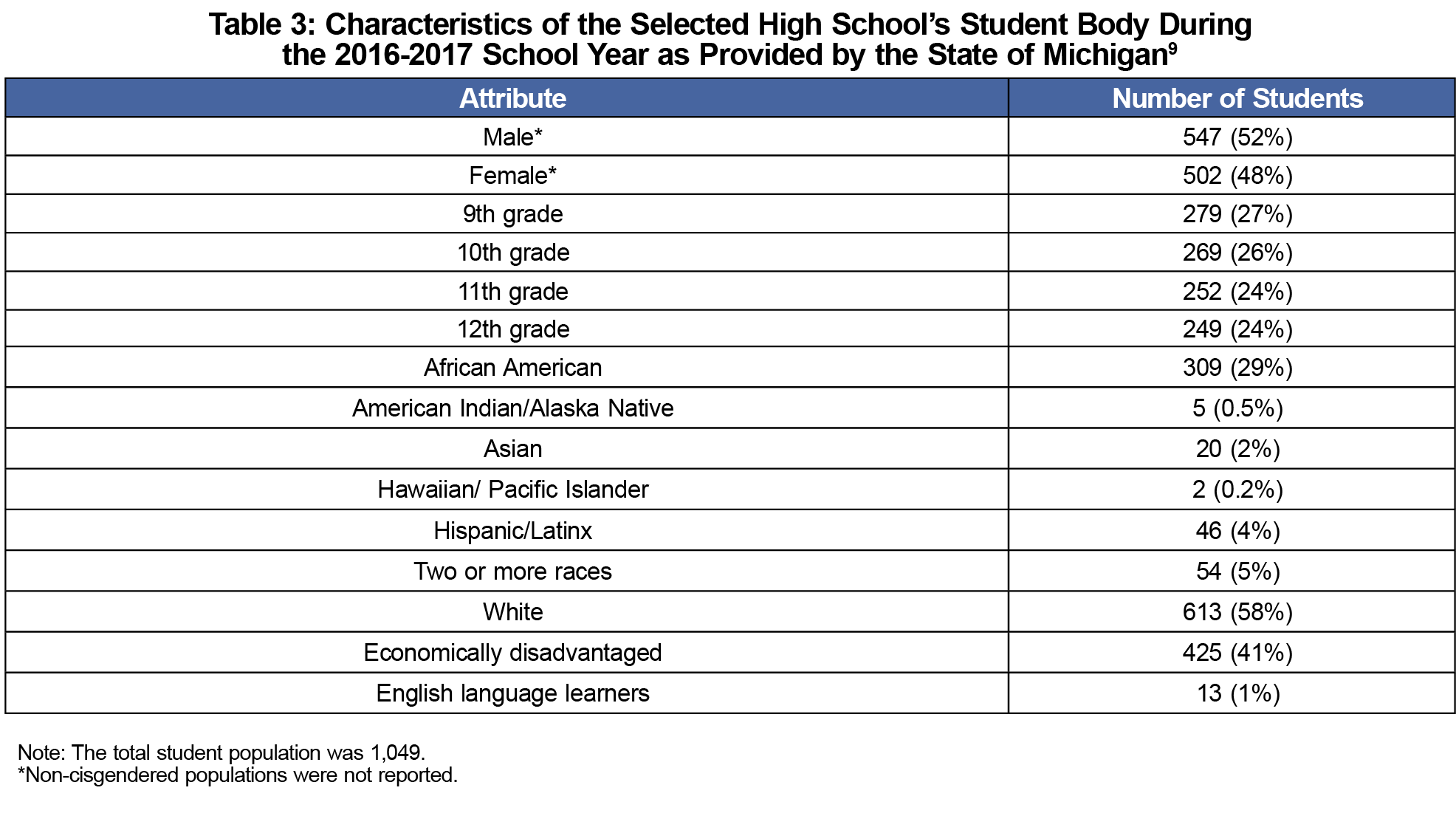
Fifty-two high school students received the MiHealth curriculum; 61 served as the control group. The students were mixed-grade (ninth-twelfth), reflecting the general characteristics of the full student body (Table 3). Eighteen preclinical medical students participated as lesson planners and instructors.
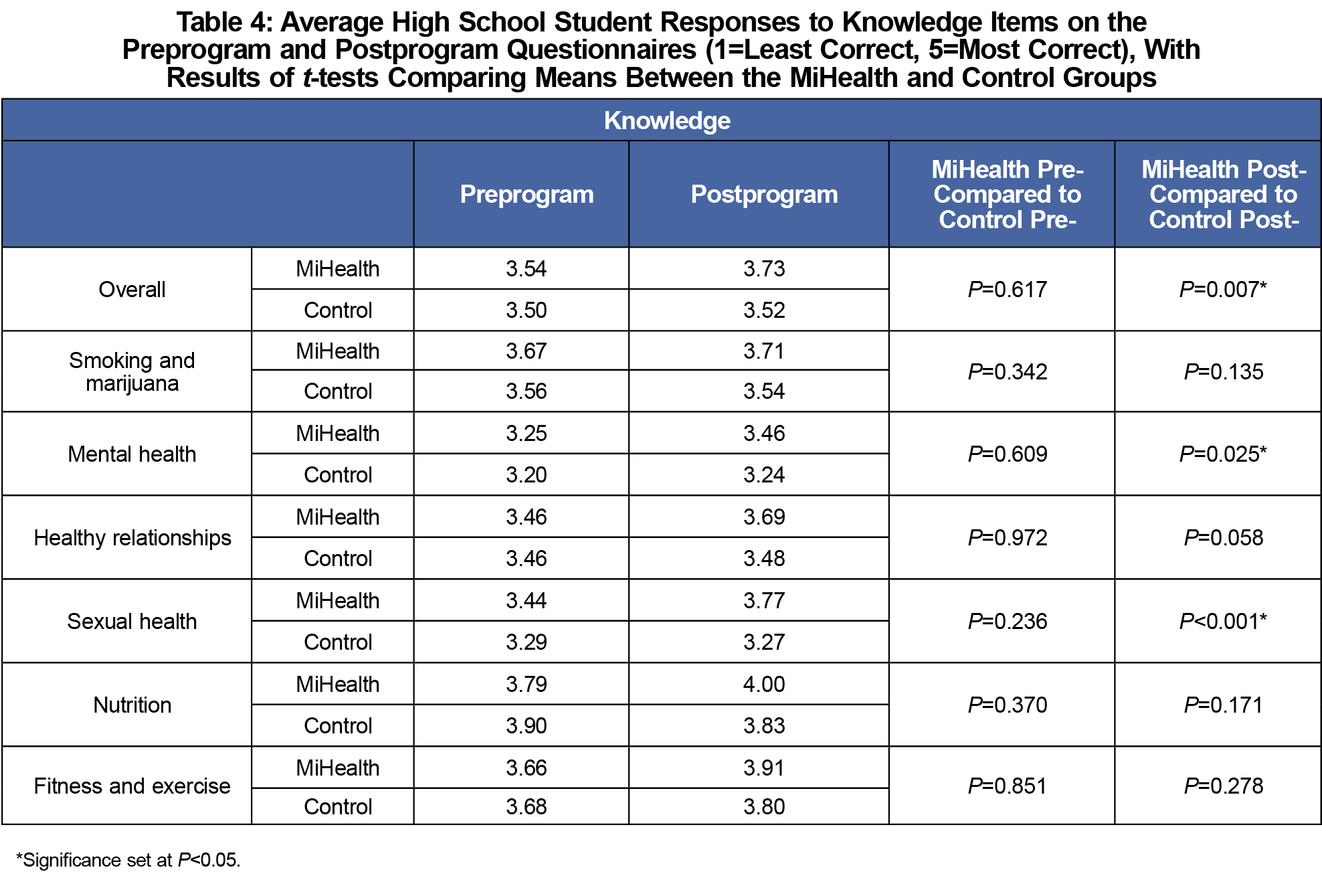
MiHealth and control preprogram health knowledge scores were not significantly different overall or in any of the six lesson themes. Six weeks after program completion, the composite health knowledge score was significantly higher for the MiHealth than the control group (P=0.007). Among individual lesson themes, the postprogram knowledge score was significantly higher for the MiHealth group compared to controls in mental health and sexual health (P=0.025, P<0.001; Table 4).
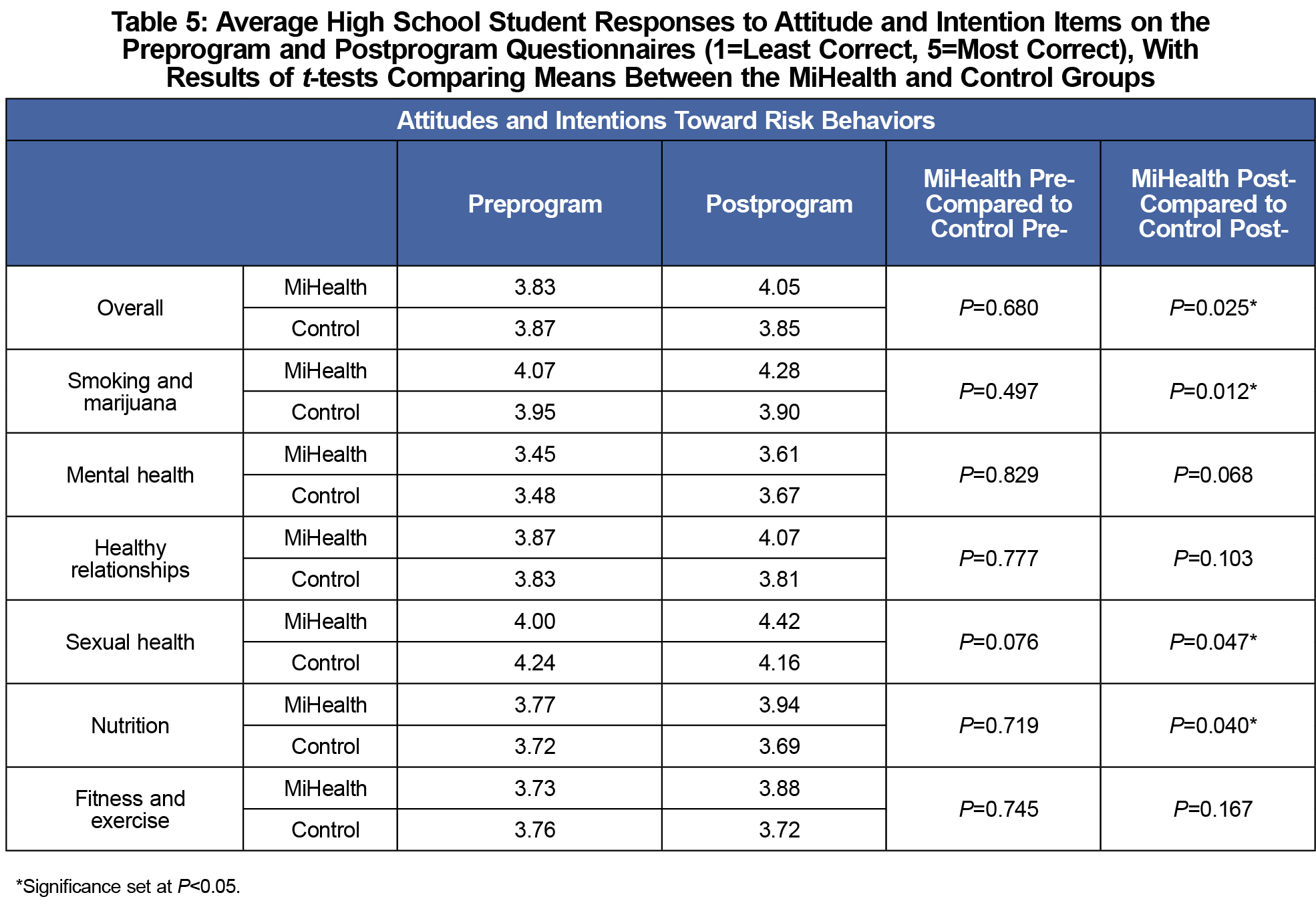
MiHealth and control preprogram attitudes and intentions toward high-risk behavior were not significantly different overall or in any specific theme. Six weeks after the program, students in the MiHealth group expressed significantly healthier attitudes and reduced intention to participate in high-risk behaviors compared to controls overall (P=0.025) and within the themes of sexual health, nutrition, and smoking and marijuana (P=0.047, P=0.040, P=0.012; Table 5).
Adolescents navigate myriad choices related to health behaviors that affect them into adulthood. The school plays a vital role in providing core curricula to promote positive health behavior.11 Yet, the quality of high school health education is variable. MiHealth aimed to fill this gap by presenting core concepts in an evidence-based, optimally effective learning environment. We used an engaging, interactive curriculum and young guest instructors with a health care background.7,12-15 The use of such instructors provided benefits of near-peer teaching, since medical and high school students share social congruence as students and young people.16,17 MiHealth produced promising improvements in high school students’ health knowledge and decreased intentions toward risky behavior, although directly measuring behaviors would be needed to fully elucidate MiHealth’s effect.18-20
MiHealth did not improve health knowledge or attitudes within every specific lesson theme. This may be due to students’ differing baseline levels of familiarity with the themes; for example, knowledge was significantly increased in sexual health and mental health, the themes with the two lowest preprogram scores. Alternatively, the array of our results could have been due to differences in lesson quality, or influenced by students from the MiHealth group sharing information with those in the control group.
Our limited pilot program involving one high school and one medical school demonstrates that an interactive curriculum targeting key adolescent health topics given by near-peer, medical student educators may provide benefits beyond existing high school health curricula. MiHealth is a successful example of an interactive, teen-focused educational intervention that can serve as a model for other health professional students and medical educators as they strive to improve the health of their communities.
Acknowledgments
Previous Presentations:
Brown KS, Meixner K. MiHealth: Medical Students Lead a Novel High School Health Education Program. Oral presentation at Conference on Adolescent Health 2017. Ypsilanti, MI. April 24, 2017.
Meixner K, Riley M. Transforming Preclinical Student Experiences through Adolescent Health Education: The Story of MiHealth. Oral presentation, STFM Annual Spring Conference. San Diego, CA. May, 2017.
References
- Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability. Am J Psychiatry. 2003;160(6):1041-1052. https://doi.org/10.1176/appi.ajp.160.6.1041
- Petit G, Kornreich C, Verbanck P, Cimochowska A, Campanella S. Why is adolescence a key period of alcohol initiation and who is prone to develop long-term problem use?: A review of current available data. Socioaffect Neurosci Psychol. 2013;3(1):21890. https://doi.org/10.3402/snp.v3i0.21890
- Casey BJ, Jones RM, Hare TA. The adolescent brain. Ann N Y Acad Sci. 2008;1124(1):111-126. https://doi.org/10.1196/annals.1440.010
- Rolison JJ, Hanoch Y, Wood S, Liu PJ. Risk-taking differences across the adult life span: a question of age and domain. J Gerontol B Psychol Sci Soc Sci. 2014;69(6):870-880. https://doi.org/10.1093/geronb/gbt081
- Jaworska N, MacQueen G. Adolescence as a unique developmental period. J Psychiatry Neurosci. 2015;40(5):291-293.
- Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance -- United States, 2015. MMWR.. 2016; 65(6):1–174.
- Kirby D. Emerging Answers 2007: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted Diseases. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2007.
- Brener ND, Demissie Z, McManus T, Shanklin SL, Queen B, Kann L. School Health Profiles 2016: Characteristics of Health Programs Among Secondary Schools. Atlanta: Centers for Disease Control and Prevention; 2017.
- Michigan’s Center for Educational Performance and Information. Student Counts for 2016-17. Available at: https://www.mischooldata.org. Accessed April 17, 2018
- Brown K. MiHealth Curriculum Assessment Questionnaire (Assessment of Selected Adolescent Health Knowledge and Intentions). STFM Resource Library. https://resourcelibrary.stfm.org/viewdocument/mihealth-curriculum-assessment-ques?CommunityKey=2751b51d-483f-45e2-81de-4faced0a290a. Accessed December 5, 2018.
- Guttmacher Institute. American Adolescents’ Sources of Sexual Health Information: Fact Sheet. http://www.guttmacher.org/pubs/FB-Teen-Sex-Ed.html. Accessed March 1, 2016.
- Cuijpers P. Effective ingredients of school-based drug prevention programs. A systematic review. Addict Behav. 2002;27(6):1009-1023. https://doi.org/10.1016/S0306-4603(02)00295-2
- Porath-Waller AJ, Beasley E, Beirness DJ. A meta-analytic review of school-based prevention for cannabis use. Health Educ Behav. 2010;37(5):709-723. https://doi.org/10.1177/1090198110361315
- Tobler NS, Roona MR, Ochshorn P, Marshall DG, Streke AV, Stackpole KM. School-based adolescent drug prevention programs: 1998 meta-analysis. J Prim Prev. 2000;20(4):275-336. https://doi.org/10.1023/A:1021314704811
- Moyer VA; U.S. Preventive Services Task Force. Primary care interventions to prevent tobacco use in children and adolescents: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2013;159(8):552-557.
- Benè KL, Bergus G. When learners become teachers: a review of peer teaching in medical student education. Fam Med. 2014;46(10):783-787.
- Yu T-C, Wilson NC, Singh PP, Lemanu DP, Hawken SJ, Hill AG. Medical students-as-teachers: a systematic review of peer-assisted teaching during medical school. Adv Med Educ Pract. 2011;2:157-172.
- Kim CR, Free C. Recent evaluations of the peer-led approach in adolescent sexual health education: a systematic review. Perspect Sex Reprod Health. 2008;40(3):144-151. https://doi.org/10.1363/4014408
- Giannotta F, Vigna-Taglianti F, Rosaria Galanti M, Scatigna M, Faggiano F. Short-term mediating factors of a school-based intervention to prevent youth substance use in Europe. J Adolesc Health. 2014;54(5):565-573. https://doi.org/10.1016/j.jadohealth.2013.10.009
- Wharf Higgins J, Begoray D, MacDonald M. A social ecological conceptual framework for understanding adolescent health literacy in the health education classroom. Am J Community Psychol. 2009;44(3-4):350-362. https://doi.org/10.1007/s10464-009-9270-8



There are no comments for this article.