During the preclinical years of medical school, education on health inequalities is mostly incorporated in lecture-based learning, whereas firsthand interaction with patients experiencing these inequities is less common. Just as inserting a chest tube cannot be fully learned from a textbook, it has been suggested that addressing health inequities is best learned in a clinical setting.1
Studies have shown that involvement in student-run free clinics (SRFCs) improved attitudes toward and interest working with the medically underserved.3,4 As of 2016, 75% of medical schools were associated with an SRFC.2 SRFCs can expose students to diverse clinical scenarios and collaborate with underresourced populations.
THRIVE is a medical student-run bridge clinic located within a sheltered housing center for individuals experiencing substance use disorder. People experiencing homelessness (PEH) endure societal stigma and face socioeconomic barriers that limit access to care, leading to disproportionately worse health outcomes compared to their housed peers.5 We conducted a cohort analysis that assessed whether volunteering at THRIVE improved first-year medical students’ (M1s) attitudes toward PEH utilizing a validated survey tool.
M1s at a Philadelphia-based medical school received a pre- and postintervention survey in September 2019 and May 2020, respectively. In the interim, students had the option to volunteer at THRIVE. The Temple University Institutional Review Board determined the study was exempt from review.
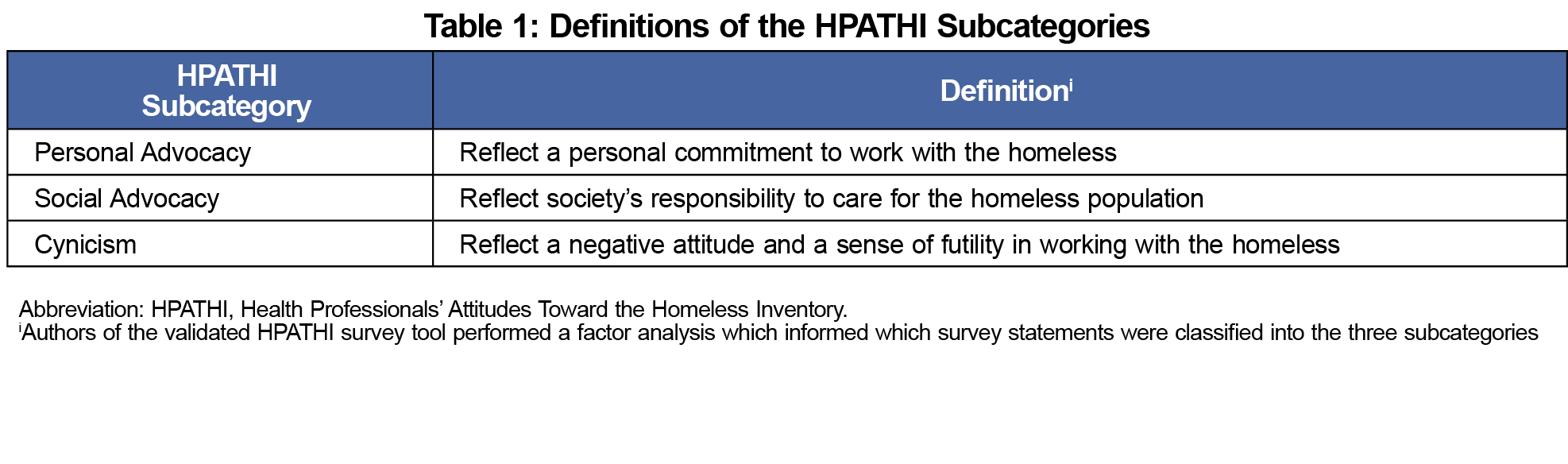
The survey captured the number of times students volunteered, demographics, experiential information, and the initial draft Health Professional Attitudes’ Towards the Homeless Inventory (HPATHI). HPATHI is a survey tool composed of statements presented on a 5-point Likert scale with statements classified into three subcategories: Personal Advocacy, Social Advocacy, and Cynicism (Table 1).6
Study data were collected and managed using REDCap (REDCap Consortium, Nashville, TN) electronic data capture tools.7,8 REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
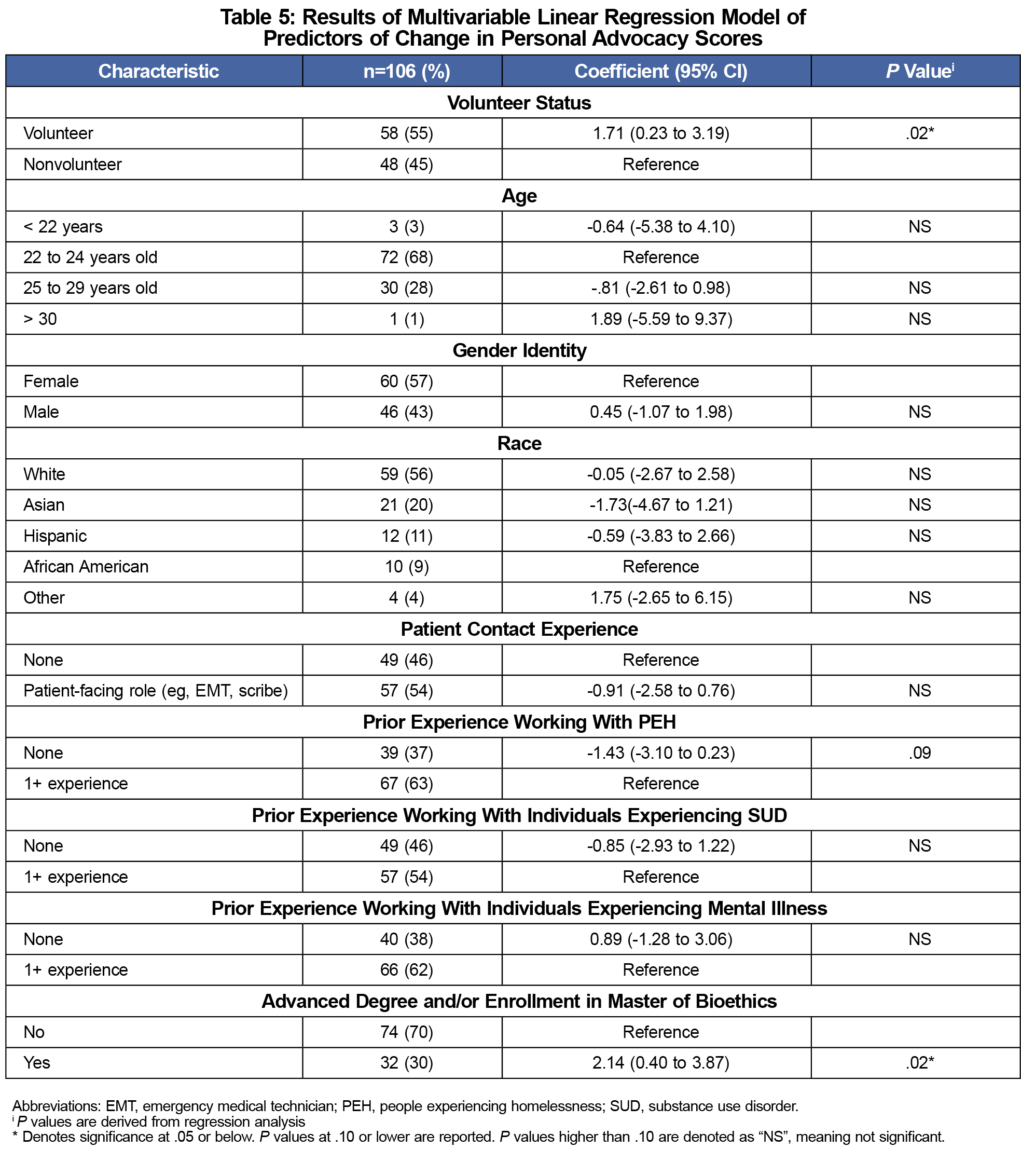
We compared demographic data for nonvolunteers and volunteers using 𝝌2 analysis. We calculated subcategory scores, with higher scores representing more positive attitudes. We calculated the differences in pre- and postsurvey scores and compared nonvolunteers and volunteers using Student t tests. We used a multivariable linear regression to determine the association between volunteering and change in Personal Advocacy scores, adjusting for participants’ demographic and experiential characteristics. Specifically, we adjusted for holding any prior advanced degree and/or enrollment in the master of bioethics program (Higher Education Students). The master of bioethics is an optional program offered to M1s that overlaps with THRIVE’s mission to highlight inequities in care. We then evaluated the association between change in Personal Advocacy scores and frequency of volunteering using analysis of variance.
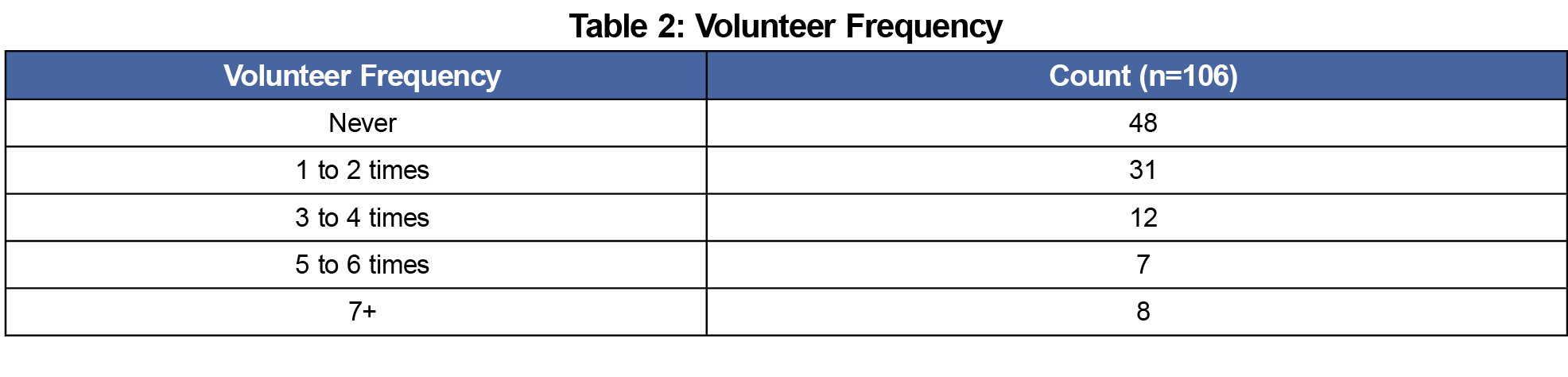
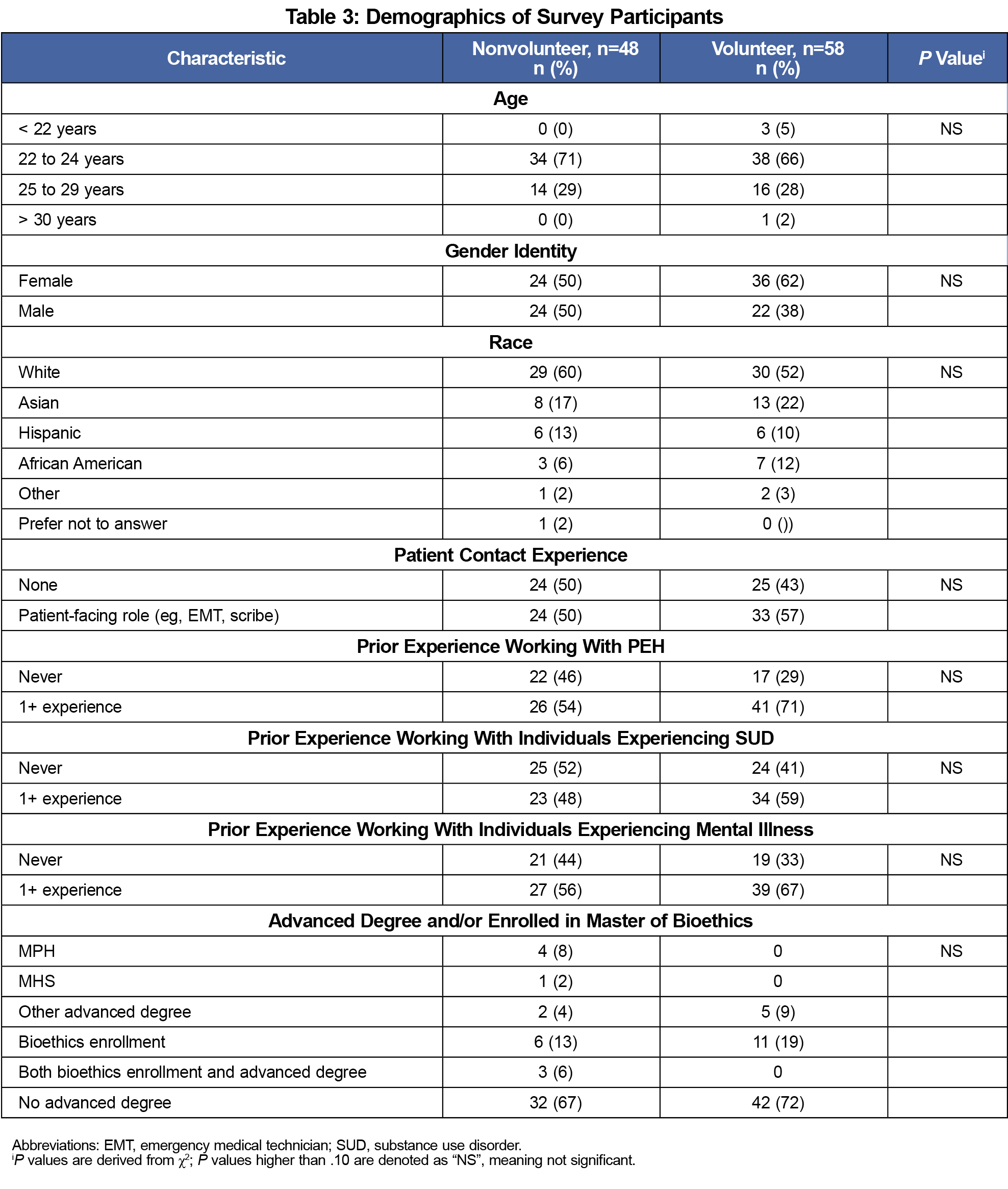
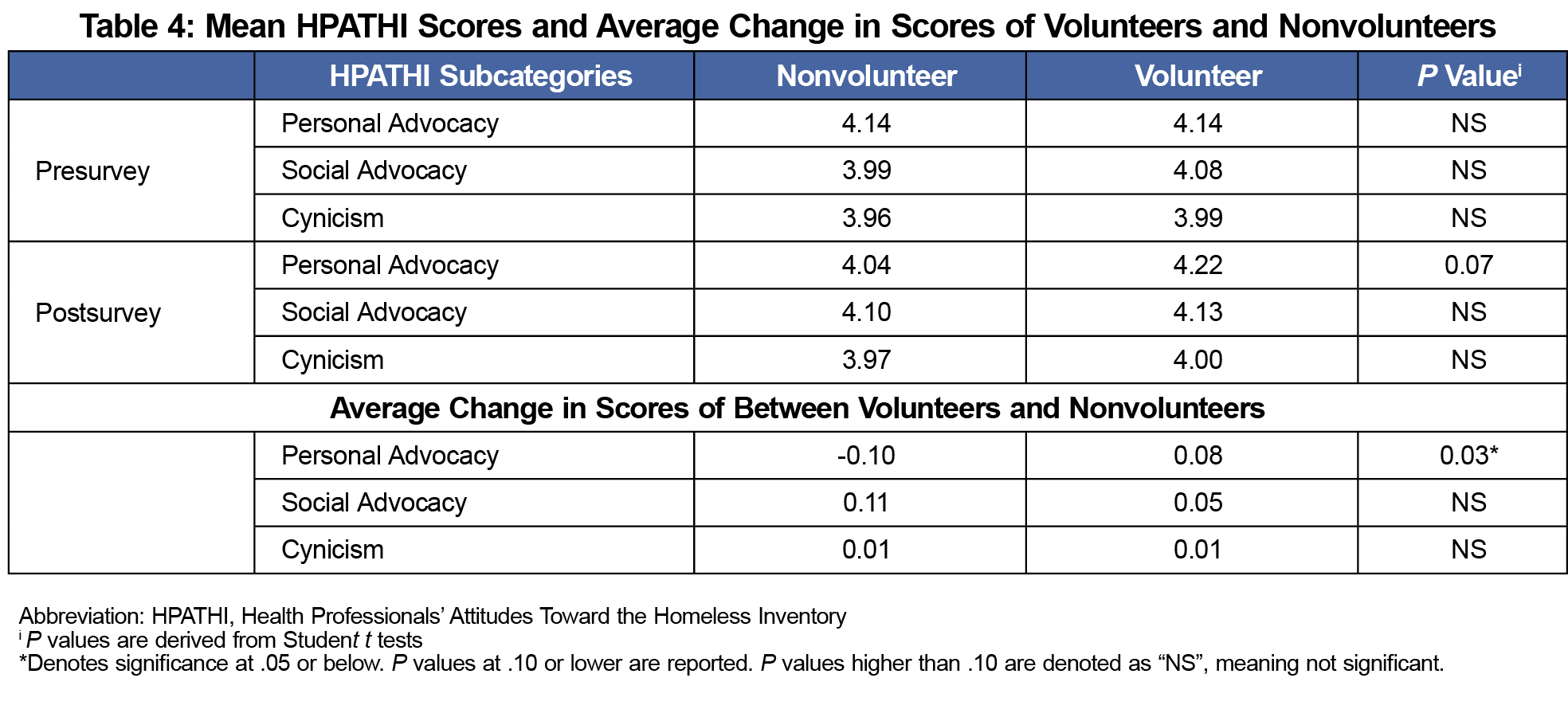
We collected 106 matched pre- and postsurvey responses (response rate 53%). Of the 106 responses, 58 (55%) students volunteered at the THRIVE Clinic at least once (Table 2). These individuals were predominantly female (62%), White (52%), aged 22 to 24 years (66%), and had previous experience working with PEH (71%). There were no statistical differences in the characteristics between non-volunteers and volunteers (Table 3) or in presurvey Personal Advocacy, Social Advocacy, and Cynicism scores (Table 4) for nonvolunteers and volunteers. The mean change in Personal Advocacy scores pre- and postsurvey was higher for volunteers than for nonvolunteers (0.08 vs -0.1; P=.03). The number of times students volunteered was not associated with an increase in Personal Advocacy scores (P=.57). There was no statistically significant difference in the mean change pre- and postsurvey in Social Advocacy (P=.40) and Cynicism (P=.97) scores among nonvolunteers and volunteers.
When adjusting for survey participants’ information, a positive association between volunteering at the THRIVE Clinic and change in Personal Advocacy score persisted (P=.02) (Table 5). In the regression analysis, Higher Education Students also demonstrated a positive association with change in Personal Advocacy scores (P=.02, Table 5).
THRIVE Clinic volunteers had increased Personal Advocacy scores compared to nonvolunteers, suggesting that interacting with PEH may improve medical student commitment to working with this population. Frequency of volunteering was not positively associated with Personal Advocacy scores, likely because grouping the volunteer cohort yielded smaller sample sizes (Table 2). Our study did not reveal a meaningful change in students’ perception of society’s responsibility to care for PEH (Social Advocacy) nor the perceived futility in caring for PEH (Cynicism). These categories may be more shaped by society’s values. In contrast, Personal Advocacy represents a individual commitment that may be more influenced by one-on-one interactions, as experienced at THRIVE. Our study also revealed that Higher Education Students were positively associated with a change in Personal Advocacy scores. This suggests that a higher level education, specifically related to public health, health science, or bioethics, may influence one’s personal commitment to work with PEH.
To date, results from other HPATHI studies have shown changes in attitudes, but none have shown statistically significant changes in the survey’s subcategories.9-12 Our study is unique because THRIVE is physically located inside a shelter, providing more context for barriers faced by patients. Additionally, this study is the first to use a regression analysis to adjust for confounders, specifically adjusting for the impact of higher education. The literature’s evaluation of the impact of higher education on a commitment to working with PEH is limited. Comparable studies include one that claimed dual-degree, MD/MPH graduates were more likely to work in primary care compared to MD graduates, though it is unclear if primary care was inclusive of underserved patient populations.13
Many factors can affect medical students’ attitudes, such as the ones that we adjusted for in the regression analysis: age, sex, race, education, and prior experience. However, our study has multiple limitations. First, we were unable to assess the temporal impact of the medical school experience on students’ attitudes. For example, several studies have shown that overall student empathy declines and burnout increases over the course of medical school.14-16 Furthermore, one study suggests that student interest in working with the underserved declines as you progress through medical school.17 Therefore, literature indicates that students have their highest level of empathy or idealism during their first year of school. Since our pre/postsurvey takes place at the beginning and end of students’ first year, it is possible that our study’s timeline reflects students’ attitudes at their most idealistic state. It has been suggested that medical student burnout can be mitigated. One study discovered that students with high levels of empathetic concern had lower levels of burnout over time.18 Other studies suggested that volunteering with PEH is important in the development and sustainment of said empathy throughout medical school.19,20 While our study highlights the potential for SRFCs to positively change students’ attitudes, it is unclear if this change in students’ attitudes will be sustained since the study occurred over an approximately 8-month period.
Second, our survey had a 53% response rate, which limited our sample size and potential findings. Furthermore, the temporary closure of the clinic in March 2020 due to COVID-19 may have contributed to our small sample size due to the limited volunteer opportunities. Third, our study does not determine how students’ attitudes translate into actions toward patients due to difficulty converting the HPATHI score into a meaningful metric in the clinical setting.
Finally, since volunteering at the THRIVE clinic is optional, self-selection bias may have influenced our study. For example, volunteers may have had a baseline interest in working with or learning about an underserved patient population. Therefore, opt-in volunteering may have self-selected for open-minded students with a preinclination to change. There is evidence in the literature that opt-in interventions may attract people who are more open minded. For example, one study evaluated the personality characteristics of respondents and nonrespondents of online surveys and concluded that respondents were more likely to have higher extraversion and higher openness to experience compared to nonrespondents.2 This example highlights that our sample of volunteers may have a higher preinclination to change compared to nonvolunteers, and hence may have an inflated change in attitudes. Therefore, future research should aim to minimize self-selection bias by evaluating mandatory experiences or measuring and adjusting for a variable representative of preinclination to change.
The regression analysis revealed a weak trend that those with no previous experience working with PEH had a negative association with change in Personal Advocacy scores. This may seem surprising, because one may expect those with limited experience to have the greatest capacity for change. However, these results further suggest a self-selection bias within the study. For example, those without prior experience with PEH, may be less open to learning about PEH, and hence less likely for their attitudes to meaningfully change. In general, this variable is difficult to interpret, because prior experiences before medical school vary considerably in setting and quality.
In conclusion, our study found that increased Personal Advocacy Scores was associated with being THRIVE clinic volunteers and students with higher education. However, these results should be interpreted in the context of multiple limitations. Future research should follow this cohort of volunteers to assess if they are actually more committed to work with PEH.



There are no comments for this article.