Background and Objectives: Resident physicians experience high levels of burnout and depression compared to the general population. While focus on promoting resident wellness, including required wellness programming from the Accreditation Council for General Medical Education (ACGME), has increased, research into resident perspectives on what should be included in these programs has been limited. This study aimed to evaluate resident perspectives on a wellness program at the University of Michigan Family Medicine Residency (UM FMR).
Methods: This qualitative study evaluated transcripts from a focus group and an anonymous survey of residents at UM FMR. Two authors reviewed transcripts using descriptive coding and a classical analysis strategy. All authors reached consensus on themes, which were then sent to residents for review and feedback.
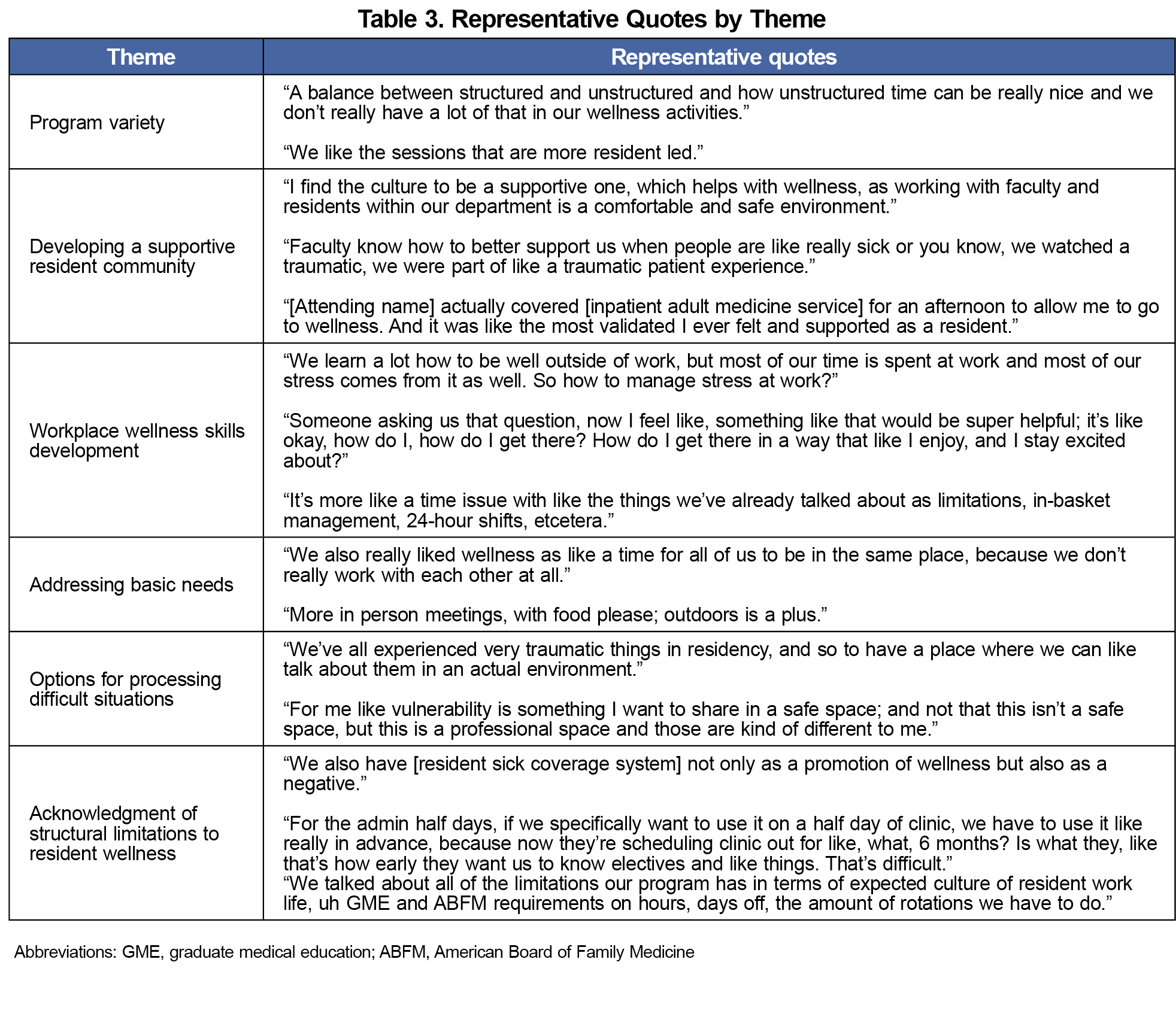
Results: Six themes emerged as important to the resident wellness program: (a) program variety, (b) developing a supportive resident community, (c) workplace wellness skills development, (d) addressing basic needs, (e) options for processing difficult situations, and (f) acknowledgment of structural limitations to resident wellness.
Conclusions: This analysis of the survey revealed opportunities for improvements in this residency wellness program and also serves as a model for future studies on resident perspectives on resident wellness.
Burnout and depression in physicians are increasingly common, particularly during residency. Though physicians are more resilient than the general population, even these resilient physicians face rising burnout rates.1 One meta-analysis found that approximately one-fourth of residents experience depression or depression symptoms annually, with rates increasing yearly.2 Family physicians should strive to increase the resiliency and wellness of trainees to improve patient safety, because burnout negatively impacts care.3,4
To combat depression and burnout, many residencies have implemented wellness programs, with mixed evidence on effectiveness.5 One study of family medicine residents noted that substandard wellness programs and insufficient time for self-care were associated with increased rates of emotional exhaustion, depersonalization, and depressive symptoms.6 Research has indicated that family medicine residents have lower satisfaction with wellness programs compared to program directors.7 For these programs to succeed, further research is needed to identify what residents find helpful in wellness curricula.
This study aimed to evaluate family medicine resident perspectives on a wellness curriculum and to develop a framework that can be used in other programs; an expanded study then could identify common themes across residency programs. Before this study, the wellness curriculum at University of Michigan Family Medicine Residency (UM FMR) consisted of 18 to 20 sessions of 1 to 3 hours each per academic year, with content based on Accreditation Council for General Medical Education (ACGME)8 requirements, residency psychologist expertise, and informal resident feedback.
Design
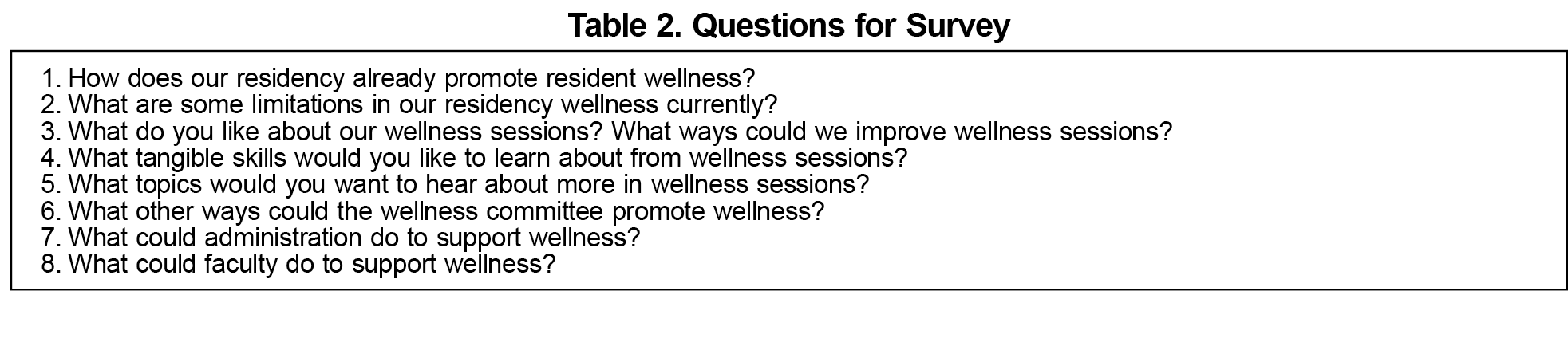
This study took place at UM FMR and was determined to be exempt from review by the Michigan Medicine Institutional Review Board (HUM00241909). A second-year family medicine resident in the same program, with experience in conducting focus groups, facilitated but did not participate in one focus group for all available residents using a question framework developed by the authors to elicit resident perspectives on strengths, weaknesses, and areas for development in the current wellness program (Table 1). This focus group was audio-recorded, then transcribed and de-identified by the facilitator. Questions from the focus group (Table 2) were adapted for an open-ended, anonymous survey that was sent to all residents in an attempt to capture all feedback and responses, and were compiled into two transcripts based on attendance at the focus group.
Analysis
Two authors reviewed the deidentified transcript of the focus group and the compiled survey responses using electronic descriptive coding and a classical analysis strategy.9 All authors reviewed the codes, which were then thematically analyzed using a grounded theory informed approach.9 Theme consensus was reached across all transcripts, and the results were presented to residents to ensure the themes reflected resident experiences and perspectives.
Out of 35 eligible residents, 21 participated in the focus group, and 16 residents completed the survey, 8 of whom participated in the focus group and 8 of whom did not participate, to achieve a response rate of 82%. Six themes, described in the following text, emerged from the data about what residents identified as important to a wellness curriculum. A selection of representative supporting quotes for the themes are included in Table 3. We found no difference in the themes between the focus group and survey responses.
1. Program Variety
Residents appreciate when wellness programming is varied, particularly in providing options for their level of participation within an activity and facilitating resident-led activities. They also recognize that each session may not be helpful for all residents, so variety in types of wellness sessions should help more residents find benefit over time.
2. Developing a Supportive Resident Community
Residents value creating a supportive community, including support from other residents, faculty, and staff, and value being involved in developing a supportive culture. Part of a wellness program needs to be giving residents a space to develop a community.
3. Workplace Wellness Skills Development
Residents identify knowledge gaps in how to maintain wellness in the workplace and how to identify role models. They identify development of these skills along with other workplace skills, including charting efficiency and workplace boundaries, as opportunities for future wellness programs.
4. Addressing Basic Needs
When wellness sessions help address needs such as providing food and creating a space for social connection, residents find them helpful. Residents currently find focusing on wellness sessions is difficult when they have to worry about trying to eat when going to or coming from busy clinics or inpatient shifts.
5. Options for Processing Difficult Situations
Residents feel that discussion of traumatic events and ways to cope are limited, but also recognize that some may feel uncomfortable being vulnerable in the workplace. Providing options for level of involvement in processing emotions is identified as important to make sure residents feel comfortable in these spaces.
6. Acknowledgment of Structural Limitations to Resident Wellness
Resident wellness has many structural limitations, including program and ACGME requirements that limit free time, schedule control, and ability to schedule time for self-care, which contribute to burnout. These are not within the control of the individual program but affect the larger context of resident wellness.
Residents identified several core areas that they would like included in wellness programs, including addressing basic needs, workplace wellness skills development, and options for processing difficult or traumatic situations. They also appreciated variety in wellness sessions and opportunities to develop community. Residents also expressed that having food at wellness sessions made them more likely to engage in the session. These findings are significant because they include topics that may not be typically considered in wellness programs.
Though this study was limited by a small sample size at a single institution, it can serve as a model for other institutions to complete reviews of their wellness programs. We also aim to expand this project to other residencies to identify common themes to improve resident wellness curricula beyond the level of the individual program. While the focus group was facilitated by a resident to improve honesty of participants, this may have introduced bias; however, the facilitator did not participate in the feedback. Responses were de-identified before analysis by a paired resident and attending, who were not involved in wellness program planning, but were interested in improving resident satisfaction, which could be another potential area for bias.
Acknowledgments
The authors thank E. Christopher Bush, MD, for his mentorship of Alyssa Warburton-Silva, MD, and this project through the American Academy of Family Physicians Family Medicine Leads Emerging Leader Institute.
References
- West CP, Dyrbye LN, Sinsky C, et al. Resilience and burnout among physicians and the general US working population. JAMA Netw Open. 2020;3(7):e209385. doi:10.1001/jamanetworkopen.2020.9385
- Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314(22):2,373-2,383. doi:10.1001/jama.2015.15845
- Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7,642):488-491. doi:10.1136/bmj.39469.763218.BE
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1,071-1,078. doi:10.1001/jama.296.9.1071
- Eskander J, Rajaguru PP, Greenberg PB. Evaluating wellness interventions for resident physicians: a systematic review. J Grad Med Educ. 2021;13(1):58-69. doi:10.4300/JGME-D-20-00359.1
- Freedy JR, Staley C, Mims LD, et al. Social, individual, and environmental characteristics of family medicine resident burnout: a CERA study. Fam Med. 2022;54(4):270-276. doi:10.22454/FamMed.2022.526799
- Penwell-Waines L, Kulshreshtha A, Brennan J, et al. Comparing resident and program director perspectives on wellness curricula: a CERA study. PRiMER. 2023;7:33. doi:10.22454/PRiMER.2023.300982
- Accreditation Council for Graduate Medical Education. ACGME Common Program Requirements (Residency). Updated September 2022. Accessed October 5, 2024. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-prs/cprresidency_2025.pdf
- Krueger RA, Casey MA. Focus Groups: A Practical Guide for Applied Research.5th ed. SAGE; 2014.




There are no comments for this article.