Introduction: The Council of Academic Family Medicine (CAFM) Educational Research Alliance (CERA) consists of four family medicine organizations that aim to promote family medicine research. Each year, CAFM members can submit audience-specific survey questions. The purpose of this paper is to review the methods and demographics of the 2024 General Membership Survey and determine the generalizability of the survey respondents.
Methods: CERA opened its call for the annual General Membership Survey proposals from May 2024 to June 2024. Twelve proposals underwent a competitive peer-reviewed process, and five were chosen. Select CAFM members received survey invitations via SurveyMonkey between October 15, 2024 and November 22, 2024. Demographics of potential survey respondents and actual survey respondents were compared using χ² tests or Fisher’s exact tests.
Results: Of the 4,844 CAFM members invited to participate, 1,194 responded, yielding a response rate of 24.7%. Demographic data from potential survey respondents were compared to actual respondents. Statistically significant differences were found at the categorical variable analysis level for variables of race/ethnicity, self-identification as underrepresented in medicine, highest degree earned, and state/province of practice/program, between the potential respondents and actual respondents. Differences in age and gender were not statistically significant between responders and nonresponders. Several characteristics were also found to not be statistically significantly different at an α of 0.05.
Conclusion: This paper describes the methods and the generalizability of the 2024 CERA General Membership Survey. The CERA surveys provide a mechanism for CAFM members to conduct national surveys on topics important to family medicine education.
The Council of Academic Family Medicine (CAFM) Educational Research Alliance (CERA), established in 2011, aims to create a centralized framework for advancing medical education research and fostering collaboration within family medicine.1–4 CERA is supported by key family medicine organizations, including the Association of Departments of Family Medicine (ADFM), Association of Family Medicine Residency Directors (AFMRD), North American Primary Care Research Group (NAPCRG), and the Society of Teachers of Family Medicine (STFM).1
CERA conducts rigorous, generalizable research in family medicine education by regularly surveying specific audiences such as family medicine department chairs, residency program directors, clerkship directors, and general members. These surveys address topics such as clinical care, curriculum development, public policy, and medical education. In addition to producing research, CERA provides mentorship and training to CAFM members on educational research methodologies.
The General Membership (GM) Survey, distributed annually, reaches a diverse audience that includes family physicians, pharmacists, behavioral health professionals, administrators, and researchers. Each survey combines member-submitted questions with recurring demographic and organizational questions. This paper summarizes the methods, demographics, and generalizability of the 2024 GM Survey.
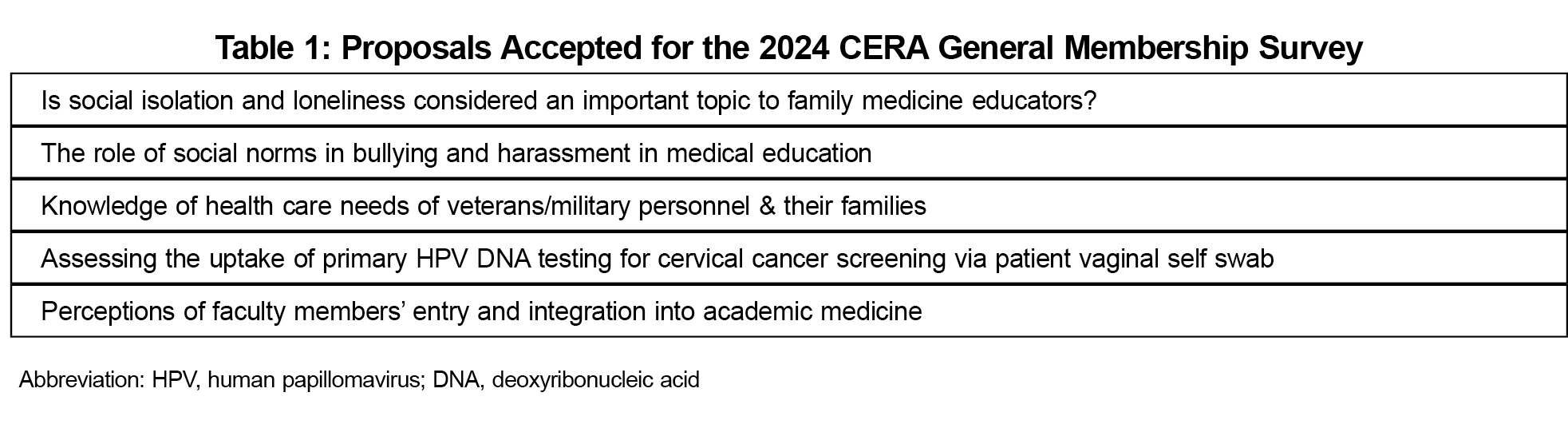
The 2024 call for GM survey proposals was open from May 27, 2024 to June 25, 2024. Of the 12 proposals received, five were selected following a peer-review process (Table 1). Each accepted proposal underwent revisions with the support of mentors, the GM survey director, and a CERA research fellow. A small team piloted the final questions to ensure clarity and readability. The American Academy of Family Physicians Institutional Review Board approved the study in October 2024.
Sample
The sample pool was based on CAFM-affiliated organization membership type in the United States and in Canada, and excluded members who were students, residents, program directors, clerkship directors, and department chairs. For individuals with multiple memberships, demographic information was based on their STFM membership. The sample pool demographics were based on membership data collected from ADFM, STFM, and NAPCRG, as demographic data from AFMRD were not available.
The initial pool of potential respondents was 5,168 individuals. We excluded 94 individuals who had previously opted out of receiving surveys from SurveyMonkey and 230 surveys were returned as undeliverable email addresses. The final pool of potential respondents was 4,844 individuals. A survey link through SurveyMonkey was sent to members in the sample pool. Nonrespondents received a total of six reminders, with five weekly emails and a final reminder sent 1 day before the survey closed. The survey was open from October 15, 2024 to November 22, 2024.
Analysis
We calculated descriptive statistics including frequencies and percentages, and we used χ² tests or Fisher’s exact tests to compare potential versus actual respondents, excluding the options of “No Response” and “Choose not to disclose.” We calculated comparisons at the demographic variable level (ie, gender as a categorical variable) and at an individual demographic response level (ie, White). We applied a significance threshold of .05 for all two-sided statistical tests, conducted using Stata SE18 software (STATA Corp, College Station, TX).
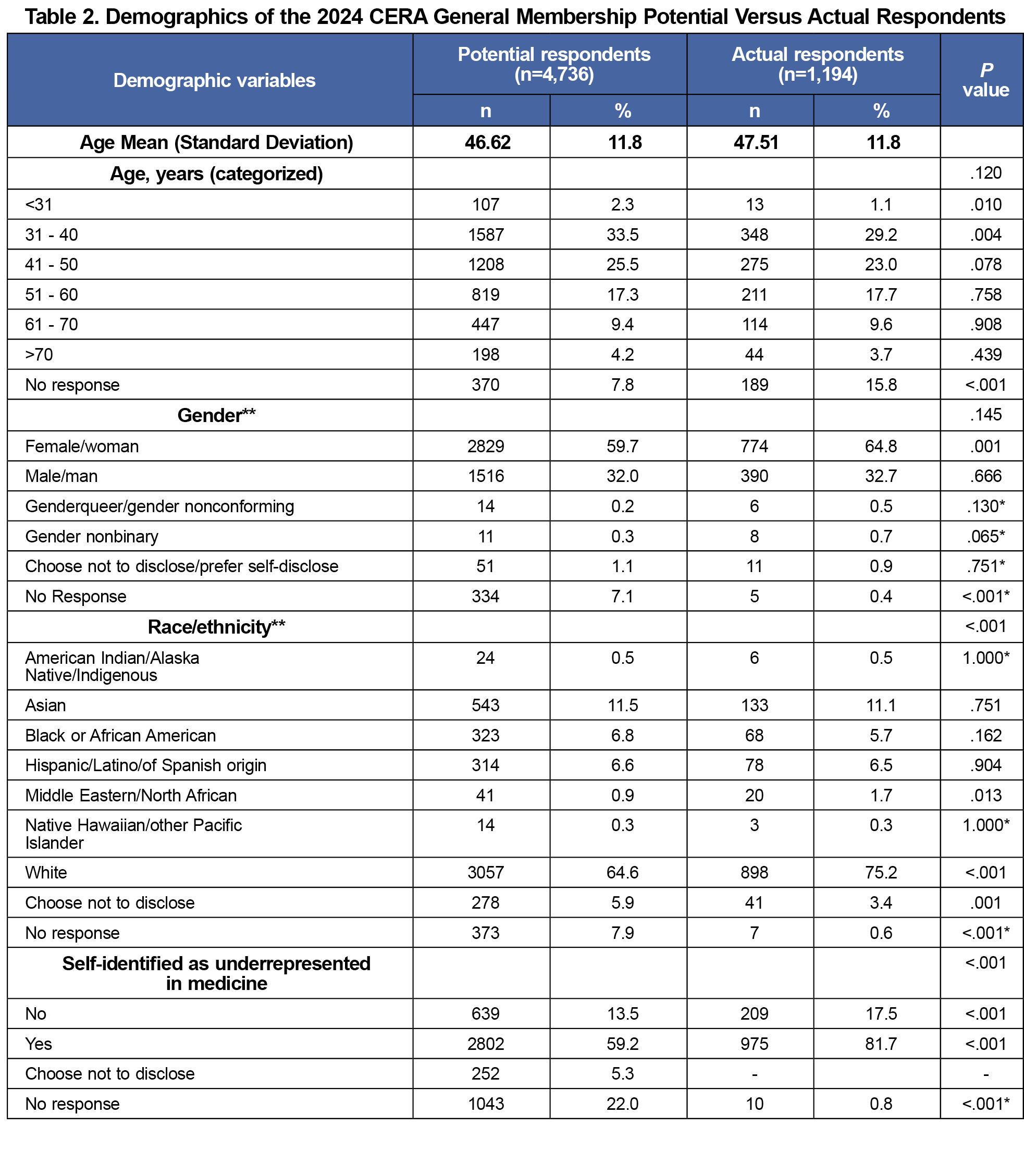
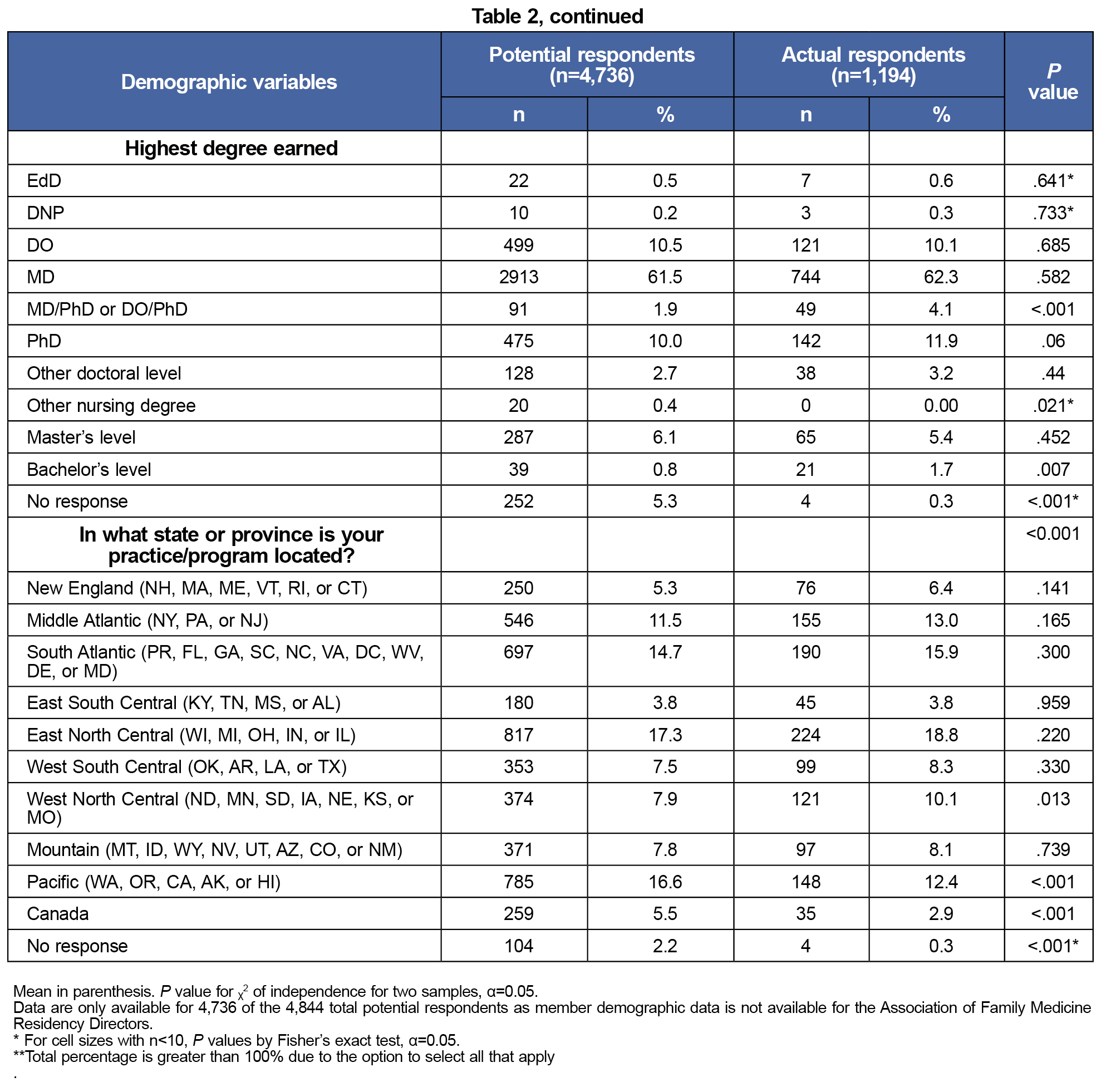
Of 4,844 potential respondents, 1,194 completed the survey, resulting in a 24.7% response rate. Demographic data for 4,736 (97.8%) of the potential respondents are based on STFM, ADFM and NAPCRG membership data. Demographic data for AFMRD members were unavailable. Table 2 compares the demographics between potential and actual survey respondents. While gender (P=.145) and age (P=.120) were not statistically significantly different, the remaining categorical variables showed statistically significant differences. Comparison at the individual demographic characteristic level revealed many of the race/ethnicity, highest degree earned, and practice/program location variables to not be statistically significant. Compared to potential respondents, actual survey respondents were more likely to be White (64.5% vs 75.2%, P<.001) or Middle Eastern/North African (0.3% vs 1.7%, P=.013), and identify as underrepresented in medicine (59.2% vs 81.7%, P<.001). Respondents were more likely to report an MD-DO/PhD as their highest degree (4.1% vs 1.9%, P<.001) and reside in the West North Central United States (10.1% vs 7.9%, P=.013) but less likely to reside in the Pacific region (16.6% vs 12.4%, P<.001).
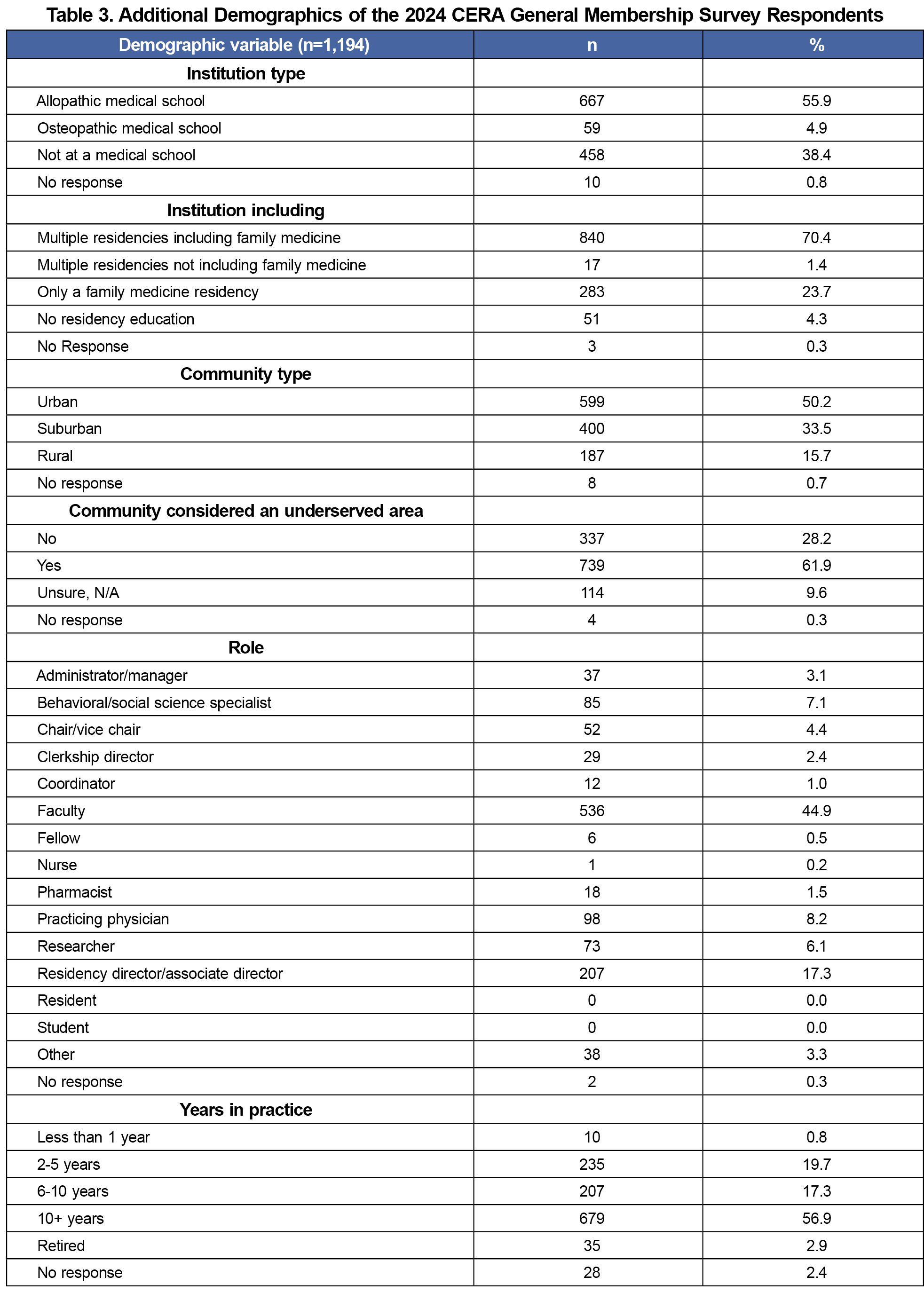
Table 3 summarizes demographic data asked in the CERA survey. More than half of respondents (55.95%) work at an allopathic medical school, and 70.4% work at an institution that has multiple residencies including family medicine. About half (50.2%) work in an urban setting, and 61.9% work in a community considered an underserved area. The highest percentage of respondents identified their role as faculty (44.9%). Of those in practice, 56.9% have worked more than 10 years.
CERA’s vision is excellence in family medicine educational research, with the mission to provide a centralized infrastructure for rigorous and generalizable medical education research, to facilitate collaboration, to provide research methods training and mentorship, and to support CERA efforts to address equity, diversity, and antiracism.5,6 The 2024 General Membership Survey investigated topics important to CAFM members and timely in the field of family medicine education.
Although some demographics differed significantly between potential and actual survey respondents, the quantity of no responses for each category limits our calculations. The missing data limits our ability to conclude that this survey sample is representative of the general membership and may influence the generalizability of survey results. Authors using CERA data can still use demographic data to perform subgroup analyses and interpret accordingly.
A strength of the CERA survey is its ability to provide a consistent, organized structure for members to conduct research that targets a national audience both in the United States and in Canada. A unique aspect of the GM survey is that members can target subgroups of professionals engaged in family medicine at various levels. For example, the 2023 GM Survey focused on active physicians, while other years have focused on nonphysician faculty.7,8
CERA survey limitations include a maximum of 10 close-ended questions per proposal and a cap on accepted proposals to decrease survey fatigue, with the current survey taking about 15 minutes to complete.
To incentivize timely submission, authors of accepted proposals have exclusive access to their data for 90 days before the 2024 GM survey data becomes accessible to all CAFM members for secondary analysis, such as hypotheses that span the questions of two or more survey teams.
Acknowledgments
The authors acknowledge the CERA Steering Committee for their help developing the manuscript version of this article.
Financial Support
CERA is supported by the academic family medicine organizations (STFM, ADFM, NAPCRG, and AFMRD). Dr Miranda Moore reports receiving funding from National Institutes of Health, Agency for Healthcare Research and Quality's, Health Resources and Services Administration, Ardmore Institute of Health, Georgia State Department of Human Services, and the Alzheimer’s Association.
Conflict Disclosure:
CERA is supported by the academic family medicine organizations (STFM, ADFM, NAPCRG, and AFMRD).
References
- Shokar N, Bergus G, Bazemore A, et al. Calling all scholars to the council of academic family medicine educational research alliance (CERA). Ann Fam Med. 2011;9(4):372-373. doi:10.1370/afm.1283
- Maxwell L, Mazzone M, Abercrombie S, et al. CERA: What? So what? Now what? Ann Fam Med. 2012;10(6):576-577. doi:10.1370/afm.1455
- Seehusen DA, Mainous AG III, Chessman AW. Creating a centralized infrastructure to facilitate medical education research. Ann Fam Med. 2018;16(3):257-260. doi:10.1370/afm.2228
- Tanner C. CERA: advancing family medicine education research. Ann Fam Med. 2024;22(2):177-177. doi:10.1370/afm.3113
- Society of Teachers of Family Medicine. Significant Events in STFM History. Accessed December 17, 2024. https://www.stfm.org/about/about/history/
- CAFM Educational Research Alliance. Accessed December 17, 2024. https://www.stfm.org/Research/CERA
- Ho T, Marzolf BA, Curtin AD, Biggs R. Protocol for the 2023 CERA General Membership Survey. Primer Peer-Rev Rep Med Educ Res. 8:26. doi:10.22454/PRiMER.2024.609918
- Mainous AG III, Rahmanian KP, Ledford CJW, Carek PJ. Professional identity, job satisfaction, and commitment of nonphysician faculty in academic family medicine. Fam Med. 2018;50(10):739-745. doi:10.22454/FamMed.2018.273724



There are no comments for this article.