Introduction: Burnout among family medicine residents remains a significant challenge, often exacerbated by electronic health record (EHR) documentation burden.1 Emerging technologies such as ambient artificial intelligence (AI), may reduce clinical documentation time while simultaneously enhancing work satisfaction. We looked to evaluate the impact of ambient AI on resident well-being, satisfaction, and documentation time.
Methods: This prospective pilot study was conducted at two community-based family medicine residency programs. Sixteen third-year residents were invited to participate in the study. Residents used ambient AI software for outpatient clinical documentation. Pre- and postintervention data included objective EHR usage metrics and well-being assessments using the Mini ReZ survey. Primary outcomes included subjective well-being, changes in documentation time per patient, and total EHR time.
Results: Fifteen residents enrolled in the study and 13 completed pre/postsurveys. The documentation time per patient decreased significantly postintervention (−3.09 min, P=.002). The overall EHR time also decreased though not significantly (P=.760). Survey data showed a significant improvement in the total Mini ReZ score (P=.012; Holm-adjusted P=.037), and improvements in subscales related to work pace/EHR stress (P=.0032; Holm-adjusted P=.013) and resident experience (P=.024; Holm-adjusted P=.048).
Conclusion: The use of ambient AI software in a family medicine resident population was associated with improved well-being, satisfaction, and documentation efficiency. This study indicates that a larger study focused on resident efficiency and subsequent satisfaction is warranted.
Burnout among resident physicians has reached critical levels, with studies estimating that over one-third of family medicine residents report burnout symptoms related to workload-related exhaustion, time spent on documentation and messaging and impacts on work-life balance.1,2 Traditional wellness initiatives focus on individual resiliency but do not address structural contributors like electronic health record (EHR) burden.3,4
Ambient artificial intelligence (AI) refers to background clinical support technology that uses natural language processing and machine learning to capture and structure patient–physician conversations into medical documentation in real time, with the potential to reduce clerical load and improve provider satisfaction.5-7 Documentation burden is a significant factor in physician burnout, especially in primary care, where charting often extends beyond clinical hours. Barr et al found upper-level family medicine residents spent more than 3 hours per day in the EHR after normal working hours, referred to as “pajama time.”8 Voice recognition software and scribe models can be applied to alleviate this burden, but face limitations in cost, training, and workflow disruption.9 Ambient AI software offers another solution. Early studies of attending-level providers show reductions in after-hours documentation and increased visit capacity.10,11
Despite promising findings among attending physicians, little is known about ambient AI’s impact on resident physicians, who face unique challenges in developing clinical reasoning and documentation skills. This pilot study examines whether integrating ambient AI into outpatient workflows can improve documentation efficiency and increase the well-being of family medicine residents.
This prospective pilot study was conducted at two community-based family medicine residency programs from January 2025 to June 2025. The study was approved by BayCare’s Institutional Review Board. The intervention used commercially available ambient AI software (Clinical Agent) for outpatient documentation and worked for all visit types over 3 months (April to June). The software directly interfaces with the EHR (Cerner), automatically transcribing clinical encounters and generating structured documentation in real time. The same EHR and AI software were used at both sites. No modifications were made to patient care processes, smart phrase usage, or supervision. Data were collected before (January–March) and during (April–June) the intervention. All third-year family medicine residents at both training sites were eligible to participate (n=16). Residents with prior AI documentation experience were excluded from the study to minimize information bias. Participation was strictly voluntary. Fifteen residents contributed EHR data, and 13 completed both pre- and postintervention surveys.
Primary quantitative outcomes focused on EHR metrics, including documentation time per patient, total EHR time per patient, and tab hops per patient encounter, captured using Lights On software (Lights On, Toronto, ON, Canada). Lights On is an analytics platform that integrates with Cerner EHR and produces dashboards with insights on clinical workflows and user efficiency within the EHR. The Mini ReZ survey was administered via RedCap Software (Vanderbilt University) before and after the intervention to assess resident satisfaction and well-being. This survey is a brief, validated tool used to measure clinician or resident well-being, burnout risk, and workplace factors that influence professional satisfaction. It provides a total score and three subscale scores: (1) supportive work environment, (2) work pace and EHR stress, and (3) resident experience.12
Statistical Analysis
We summarized continuous variables as means (SD) or median (IQR), and categorical variables as counts and percentages. We then compared outcomes for these two data sets between the pre and the post period using the paired t tests or Wilcoxon signed-rank tests, depending on normality. We applied the Holm–Bonferroni method for multiple comparison correction to reduce the risk of type-I error.
We used an interrupted time series method with the linear mixed model (LMM) to evaluate whether the outcomes of Lights On data differed significantly monthly in the pre and post periods, accounting for existing baseline trends and enhancing causal inference. With the ITS method, the aim was to evaluate if the AI intervention had an immediate significant impact on these outcomes, and if the outcomes continue to change at a different rate after the intervention.
We considered a two-sided P value <.05 statistically significant. We performed all analyses using statistical software R (version 4.5.0; R Core Team, 2025).
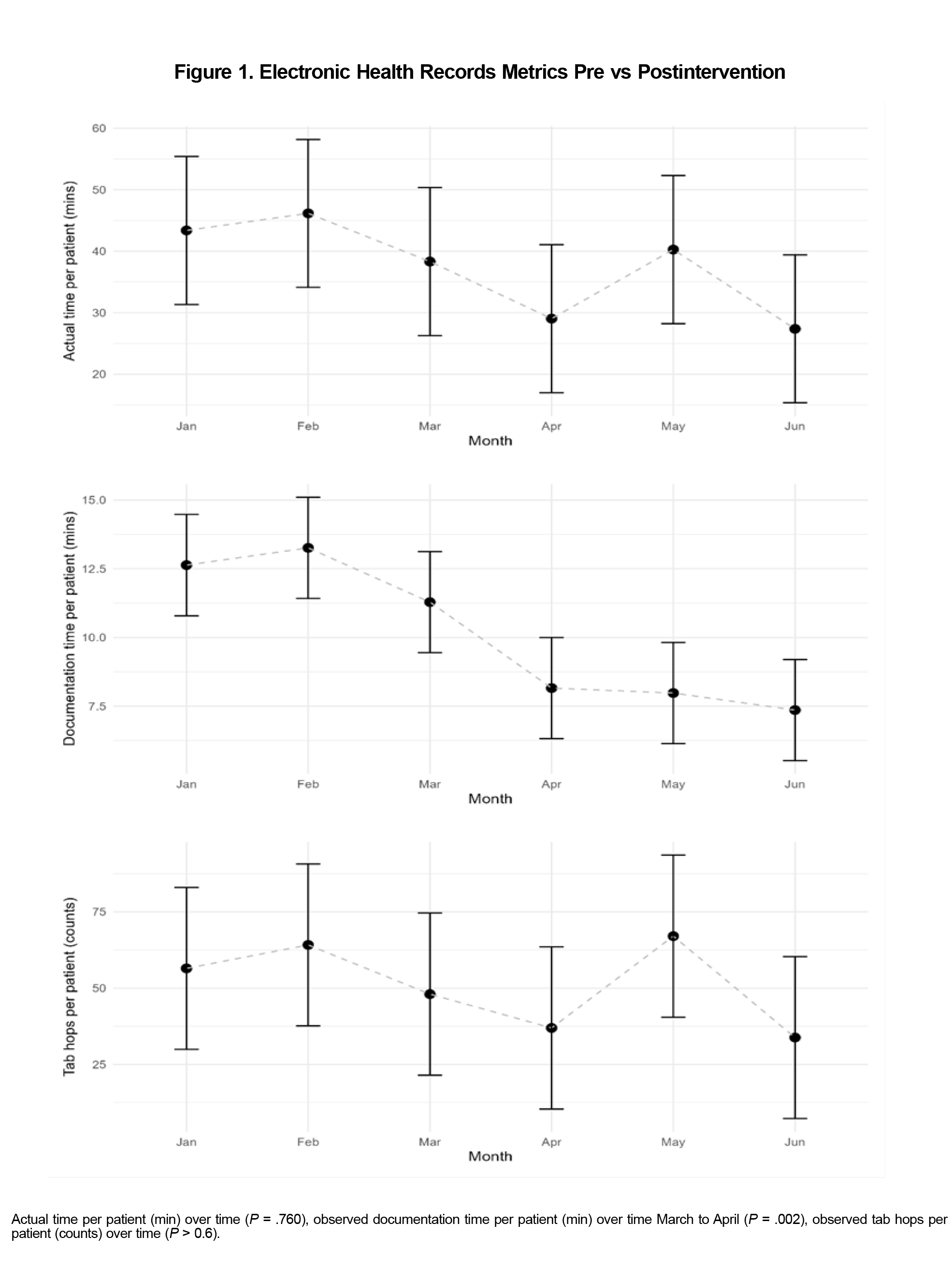
Three metrics evaluated time spent in the EHR: (1) documentation time per patient in minutes (time documenting the patient encounter), (2) total EHR time per patient in minutes (total time in patient EHR), and (3) tab hops per patient encounter (clicks between tabs in the EHR). Results showed total EHR time decreased from 39 minutes in March to 29 minutes in April. However, a rebound occurred in May and June, up to approximately 40 minutes, and was thus not statistically significant (P=.760). Documentation time per patient showed a sustained decrease after AI software initiation, dropping from approximately 11 minutes in March to approximately 8 minutes in April and remained low through June (P=.002). Tab hops, a workflow inefficiency proxy, dropped in April (from about 50 to about 36) but rebounded in May and June (P>.6, Figure 1).
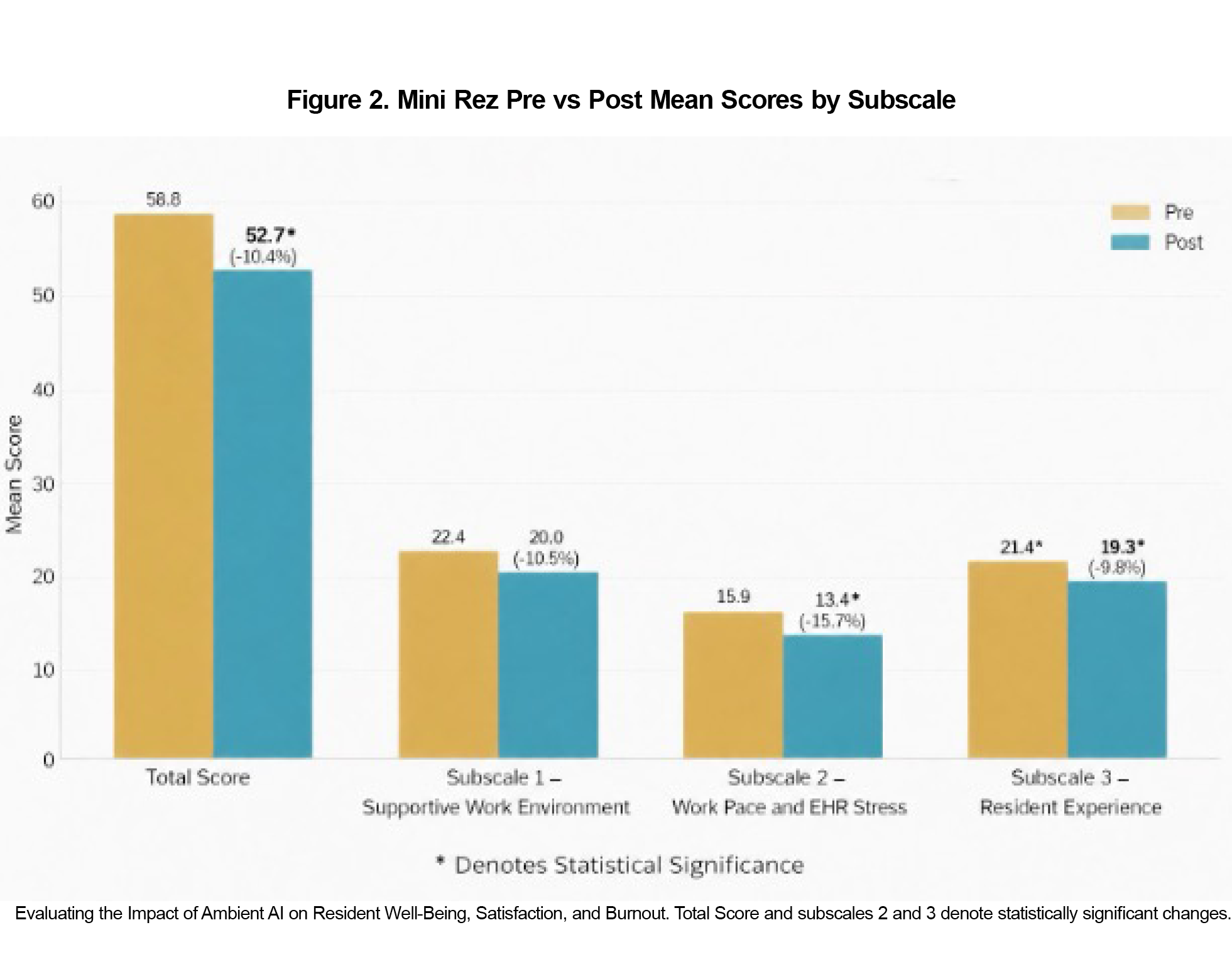
Using Mini ReZ scoring, we calculated total scores and three subscale scores. Mini ReZ Total Scores (influenced by the three subscales combined) improved significantly after intervention (paired t test: raw P=.012, Holm-adjusted P=.037). Two subscale scores, work pace and EHR stress and resident experience, showed statistical improvement (P=.0032 and P=.024, respectively). Subscale 1, supportive work environment, did not significantly change (P=.107, Figure 2).
This pilot study provides preliminary evidence that ambient AI offers family medicine residents meaningful benefits by reducing documentation burden and improving well-being. Documentation time per patient decreased by over 3 minutes, representing a significant gain for time-constrained trainees. Mini ReZ scores showed significant improvements in work pace, EHR stress, and resident experience, while supportive work environment and tab-hopping behavior did not change significantly, possibly reflecting structural inefficiencies unaddressed by AI or individual patterns of EHR usage.
Study strengths include objective EHR metrics, validated surveys, and a multisite design. Limitations include small sample size, lack of control group, and potential selection bias. As AI integrates into medical education, training sites must ensure trainees first independently develop critical thinking and documentation skills before adopting AI-assisted models. Further research should explore per-resident documentation time savings and analyze changes by visit type and note section. Additionally, as AI adoption expands, it will be important for graduate medical education programs to evaluate optimal implementation strategies, effective workflow integration, and its impact on learner outcomes and patient care. The availability of AI scribes may also serve as a potential recruitment asset, signaling institutional commitment to workflow efficiency, reduced administrative burden and learner wellbeing. While early experience with ambient AI demonstrates immediate benefits in efficiency, and resident experience, further investigation is warranted to evaluate long-term effects and identify opportunities for optimization.
Acknowledgments
The authors thank the residents and faculty at the USF/MPM and FSU/Winter Haven Family Medicine Residency Programs for their participation. They also sincerely thank Tina Cimini for her contributions to this project, particularly her expertise in navigating the Lights On system.
AI Use Disclosure: The authors used ChatGPT to create Figure 2 and correct grammatical errors.
Funding Statement: The authors received no external funding for this study.
Conflict Disclosure: The authors declare no conflicts of interest.
Presentation: This study was presented as a poster at the STFM Annual Spring Conference in New Orleans, Louisiana, May 2-6, 2026.
References
- Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. 2023;14:21501319231166921. doi:10.1177/21501319231166921
- Doe S, Coutinho AJ, Weidner A, et al. Prevalence and Predictors of Burnout Among Resident Family Physicians. Fam Med. 2024;56(3):148-155. doi:10.22454/FamMed.2024.875388
- Eskander J, Rajaguru PP, Greenberg PB. Evaluating wellness interventions for resident physicians: a systematic review. J Grad Med Educ. 2021;13(1):58-69. doi:10.4300/JGME-D-20-00359.1
- Pipas CF. Improving Physician Well-Being Through Organizational Change. Fam Pract Manag. 2020;27(6):23-28.
- Olson K, Marchalik D, Farley H, et al. Organizational strategies to reduce physician burnout and improve professional fulfillment. Curr Probl Pediatr Adolesc Health Care. 2019;49(12):100664. doi:10.1016/j.cppeds.2019.100664
- Lee C, Britto S, Diwan K. Evaluating the Impact of AI on documentation efficiency: a scoping review. Cureus. 2024;16(11):e73994.
- Nahar JK, Kachnowski S. Current and potential applications of ambient artificial intelligence. Mayo Clin Proc Digit Health. 2023;1(3):241-246. doi:10.1016/j.mcpdig.2023.05.003
- Barr W, Peterson L, Fleischer S. Pajama time: the association of ehr documentation time with family medicine resident outcomes. Ann Fam Med. 2024;22(suppl 1):6628. doi:10.1370/afm.22.s1.6628
- Gidwani R, Nguyen C, Kofoed A, et al. Impact of scribes on physician satisfaction, patient satisfaction, and charting efficiency: a randomized controlled trial. Ann Fam Med. 2017;15(5):427-433. doi:10.1370/afm.2122
- Ma SP, Liang AS, Shah SJ, et al. Ambient artificial intelligence scribes: utilization and impact on documentation time. J Am Med Inform Assoc. 2025;32(2):381-385. doi:10.1093/jamia/ocae304
- Holmgren AJ, Fenton CL, Thombley R, et al. Ambient artificial intelligence scribes and physician financial productivity. JAMA Netw Open. 2026;9(1):e2553233. doi:10.1001/jamanetworkopen.2025.53233
- Linzer M, Shah P, Nankivil N, Cappelucci K, Poplau S, Sinsky C. The Mini Z Resident (Mini ReZ): psychometric assessment of a brief burnout reduction measure. J Gen Intern Med. 2023;38(2):545-548. doi:10.1007/s11606-022-07720-0



There are no comments for this article.