Introduction: Group concept mapping (GCM) is a mixed-method participatory research approach that integrates stakeholder input to visually represent complex ideas and issues. Within medical and public health education, GCM has gained traction for its ability to synthesize diverse perspectives and guide decision-making in curriculum development, assessment, and support strategies.
Methods: This article details the GCM methodology and synthesizes the literature on its applied use in medical and public health education. Included studies employed GCM’s multistep process—idea generation, sorting and rating, data analysis, and stakeholder interpretation—to identify thematic structures and inform educational practices. Studies involved varied participant groups, including students, faculty, health care providers, and community stakeholders, using both online and in-person modalities.
Results: Across studies, GCM was used to address curriculum alignment, competency. development, student well-being, mentorship, diversity, and assessment. For instance, GCM revealed educational blind spots, guided development of interdisciplinary competencies, and prioritized public health outcomes. It also identified resilience factors and mentorship qualities critical for student and faculty development. In assessment contexts, GCM structured feedback mechanisms and clarified selection criteria for residency programs. The method consistently provided structured, stakeholder-informed visual maps to inform actionable changes.
Conclusions: GCM has proven to be a versatile and effective tool in medical and public health education. Its participatory nature enhances relevance, content validity, and stakeholder engagement, while its structured outputs support curricular reforms, competency development, and equity-driven initiatives. As the educational landscape evolves, GCM offers a valuable methodology for navigating complexity and fostering inclusive, evidence-informed strategies.
Group concept mapping (GCM) is a mixed-method, participatory research methodology widely applied in social science, health care, education, and organizational research. GCM is used to identify and organize ideas related to a specific topic or issue through the engagement of stakeholders in the research process.1 Developed by Trochim,2 GCM enables researchers to amplify the voices of stakeholders and apply rigorous analytics to opinions, beliefs, and values to yield a visual framework. The GCM approach aligns with practical approaches for understanding what counts as valid knowledge (ie, pragmatic epistemology). As an applied methodology, GCM integrates qualitative and quantitative techniques to collaboratively generate, organize, and interpret ideas. Recognizing that knowledge is unequally distributed across individuals, researchers use GCM to uncover the collective understanding of concepts among members of a group, making the approach particularly insightful for complex or underidentified problems.3 Readers can find a general description of GCM and use cases at https://groupwisdom.com/gcmrg as well as in several widely available texts.1,4
Twenty years ago, Trochim and Kane5 outlined the potential of GCM as a conceptualization tool in the health care context. They argued that GCM is a unique approach to address the complexity found within the health care environment, owing to the need to collaborate across disciplines and include stakeholders at multiple levels. In the past decade, a growing number of GCM studies within medical and public health education have collectively demonstrated the versatility of GCM for identifying, organizing, and prioritizing a variety of factors within medical and public health education. This body of applied studies illustrates how GCM facilitates stakeholder engagement, consensus building, and actionable insights to enhance education, wellness, and equity in health professions training.
Overview of GCM Methodology
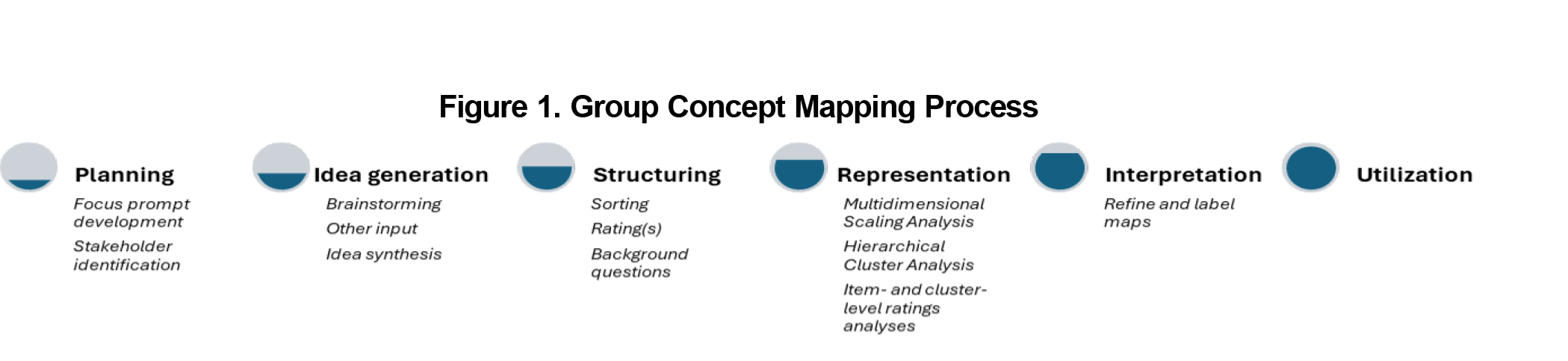
Readers may be familiar with other group input and engagement methods, such as Delphi methods, nominal group technique, or stepladder technique. In the same way, Trochim’s concept mapping model is a structured, sequenced, and systematic approach to capturing the way a group thinks about a specific topic. GCM typically is conducted in a series of steps, shown in Figure 1.
Planning
Beginning with planning, researchers define the focus of the study, develop a guiding research question, and identify key participants to provide relevant insights. During this step, a focus prompt is created to elicit ideas, often formatted as a sentence completion task (eg, “One issue that affects patient engagement in health care decisions is . . .”). This prompt guides the entire process and ensures that the group’s attention is directed toward a shared problem or concept. Here additional logistical decisions, such as whether data collection is online or in-person and overall study design, are considered.
Idea Generation
The next step is idea generation, where participants contribute responses to the focus prompt through brainstorming sessions, although open-ended surveys, interviews, or document analysis can be employed as well. Participants are asked to generate ideas or statements related to the focus question. The objective is to gather a broad and diverse range of statements that reflect different perspectives on the topic.
Structuring
These statements serve as the foundation for the structuring step, in which participants categorize the collected statements into meaningful groups based on perceived similarity. This step helps to reveal patterns or relationships among ideas and lays the foundation for creating a conceptual structure. In addition to sorting, participants rate each statement on predetermined criteria, such as importance or feasibility, often using a Likert-type scale. Demographic information also is collected to allow for subgroup analysis.
Representation
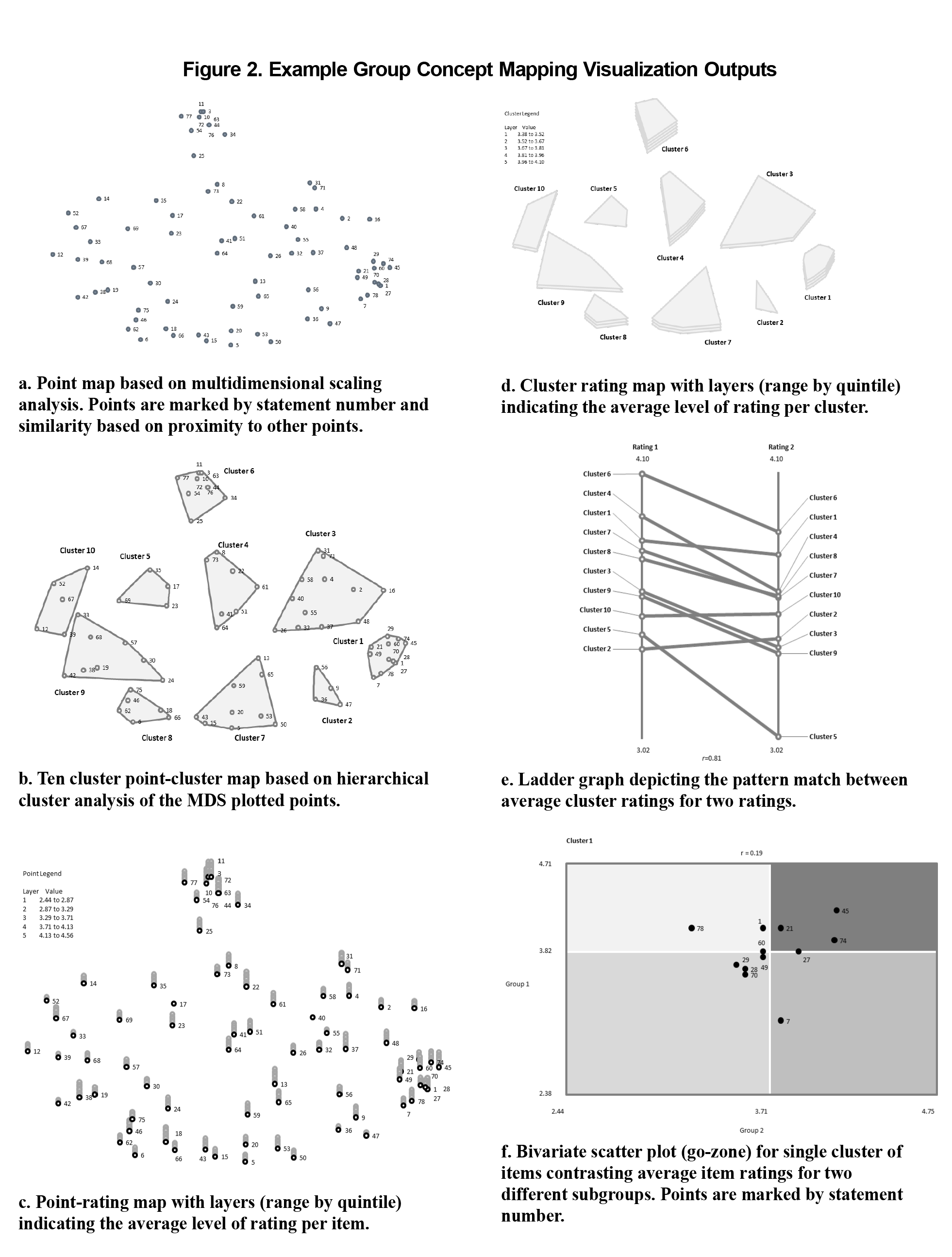
Once sorting and rating are completed, the representation step involves application of multivariate statistical analyses to generate visualizations of the data. Multidimensional scaling6 analysis of frequency of statement pairings (ie, nonmetric) positions statements in two-dimensional space, ensuring that closely related statements sorted together by participants appear near one another. The multidimensional scaling is followed by hierarchical cluster analysis,7 which groups closely positioned statements into nonoverlapping clusters representing overarching themes. This combination of multivariate analyses facilitates the emergence of a multilevel structure of the content, representing the beliefs and values implicitly held by the group.3 Resulting visuals include point maps displaying the location of individual statements and cluster maps illustrating thematic groupings of ideas (Figures 2a and 2b). For many, the strength of GCM lies in the sequencing and integration of qualitative input from participants with robust statistical analyses to yield interpretable results and limit researcher subjectivity.
Ratings data are overlayed on the structure providing an integrated view of the relational patterns (results from sorting) and the values assigned by participants (results from rating) at both the item (Figure 2c) and cluster levels (Figure 2d). Additional analyses, such as pattern-matching graphs (Figure 2e) and bivariate scatter plots (Figure 2f), help identify relationships among the ratings between clusters and different subgroups. This step ensures that the conceptual framework accurately reflects the value perspectives of those engaged.
Utilization
The final step, utilization, involves applying the GCM results to research, policy planning, program evaluation, or measurement development. The structured framework produced through GCM helps inform decision-making processes, as well as supports development of valid and reliable measurement instruments. Researchers value GCM for its ability to integrate diverse perspectives, enhance content validity, and provide a clear visual representation of complex concepts, thereby increasing the likelihood of use of the results.
Applications of GCM in Medical and Public Health Education
GCM has been widely applied to identify and address challenges in medical and public health education. Together, multiple studies underscore GCM’s adaptability and utility in addressing contemporary challenges present in this educational environment.
Curricula for Modern Health Care Systems
Several studies illustrate GCM’s capacity to structure diverse insights into actionable and better-aligned curricula for modern health care systems. Tackett et al8 used GCM with stakeholders to uncover blind spots in US medical education, organizing 208 identified issues into nine domains, such as admissions processes, teaching practices, patient perspectives, and inequities in education and health. Similarly, Ogden et al9 included health service providers from varied disciplines, health educators, health managers, and service users in mapping essential attributes and generic competencies for health care professionals. GCM processes resulted in several domains emphasizing leadership, communication, and systems thinking as key competency areas for modern complex adaptive health care systems. Stoyanov et al10 applied GCM to develop interdisciplinary learning outcomes for a biomedical design module, prioritizing skills like creativity, teamwork, and problem-solving. Morley et al’s11 use of GCM outlined public health competencies for medical students, emphasizing population health science, cultural understanding, and systems-based practice.
Well-Being and Support for Medical Students and New Faculty
Well-being and support for medical students and new faculty were priorities found in another set of GCM studies. Winseman et al12 identified nine clusters affecting student well-being, with personal wellness and supportive relationships being rated most significant. Donohoe et al13 focused on resilience strategies, finding that students valued family support and exercise most highly in stress management programs. Fu et al14 used GCM to identify the characteristics of successful mentorship relationships within the Society of Teachers of Family Medicine New Faculty Scholars program. Finally, given the potential differences among faculty, Szoko et al15 used GCM to elevate pediatric resident voice in conceptualizing factors impacting diversity, equity, and inclusion efforts at a Midwestern medical school.
Assessment Practices
Multiple studies underscore GCM’s potential to improve assessment practices in medical education, including criteria to evaluate applicants, as well as fostering actionable and inclusive feedback from students. Althans et al16 used GCM to derive five domains (eg, scholarly work and research, grades/formal assessments, program fit) of desirable characteristics of highly qualified, academic general surgery residency applicants. Furthering this work, Althans et al17 used GCM to identify barriers to feedback exchange in surgery clerkships and evaluate the Flash Feedback tool. Challenges such as time constraints and interpersonal dynamics were categorized, and the tool was effective in addressing key barriers. Hagell et al18 applied GCM in nursing education to evaluate research assignments, identifying high-priority areas such as research methodology and patient perspectives.
Collectively, the aforementioned studies highlight the versatility of GCM in tackling diverse challenges in medical and public health education. By facilitating structured stakeholder input, researchers and practitioners employing GCM identified gaps, developed a range of competencies, and created interventions tailored to the evolving needs of health care education. Researchers demonstrated that GCM’s participatory approach enriches the relevance and feasibility of medical and public health educational initiatives, fostering stronger alignment with community and institutional needs. Although the specific methods used in CGM are familiar and widely employed by researchers and students, the integration and sequencing of the techniques as well as utilization of the results require additional expertise. Several guides detailing the step-by-step approach, along with design recommendations, are available.1,4 In addition, training resources, workbooks, and videos can be found through a quick search of the Web. Interested users of GCM might consider formal training to learn how to design and implement the methodology or seek the guidance of an experienced methodologist/consultant to ensure that CGM meets the objectives of the project.
References
- Kane M, Trochim WMK. Concept Mapping for Planning and Evaluation. Sage; 2007. doi:10.4135/9781412983730
- Trochim WMK. An introduction to concept mapping for evaluation and planning. Eval Program Plann. 1989;12(1):1-16. doi:10.1016/0149-7189(89)90016-5
- Rosas SR. Group concept mapping methodology: toward an epistemology of group conceptualization, complexity, and emergence. Qual Quant. 2017;51(3):1,403-1,416. doi:10.1007/s11135-016-0340-3
- Kane M, Rosas S. Conversations About Group Concept Mapping: Applications, Examples, and Enhancements. Sage; 2017.
- Trochim W, Kane M. Concept mapping: an introduction to structured conceptualization in health care. Int J Qual Health Care. 2005;17(3):187-191. doi:10.1093/intqhc/mzi038
- Hout MC, Papesh MH, Goldinger SD. Multidimensional scaling. Wiley Interdiscip Rev Cogn Sci. 2013;4(1):93-103. doi:10.1002/wcs.1203
- Beckstead JW. Using hierarchical cluster analysis in nursing research. West J Nurs Res. 2002;24(3):307-319. doi:10.1177/01939450222045923
- Tackett S, Steinert Y, Mirabal S, Reed DA, Wright SM. Using group concept mapping to explore medical education’s blind spots. Teach Learn Med. 2025;37(1):75-85. doi:10.1080/10401334.2023.2274991
- Ogden K, Kilpatrick S, Elmer S, Rooney K. Attributes and generic competencies required of doctors: findings from a participatory concept mapping study. BMC Health Serv Res. 2021;21(1):560. doi:10.1186/s12913-021-06519-9
- Stoyanov S, Spoelstra H, Bennett D, et al. Use of a group concept mapping approach to define learning outcomes for an interdisciplinary module in medicine. Perspect Med Educ. 2014;3(3):245-253. doi:10.1007/S40037-013-0095-7
- Morley CP, Rosas SR, Mishori R, et al. Essential public health competencies for medical students: establishing a consensus in family medicine. Teach Learn Med. 2017;29(3):255-267. doi:10.1080/10401334.2016.1268964
- Winseman JS, Higgins EA, Balkoski VI, Rosas SR. What affects well-being during medical education? a student and faculty concept map. Ann Behav Sci Med Educ. 2015;21(1):19-29. doi:10.1007/BF03355305
- Donohoe J, O’Rourke M, Hammond S, Stoyanov S, O’Tuathaigh C. Strategies for enhancing resilience in medical students: a group concept mapping analysis. Acad Psychiatry. 2020;44(4):427-431. doi:10.1007/s40596-020-01208-x
- Fu J, Gardner-Buckshaw S, Schirmer JM, Minor S, Ogbeide S. Understanding successful mentor-mentee relationships in new faculty scholars program. PRiMER. 2024;8:31. doi:10.22454/PRiMER.2024.709691
- Szoko N, Radovic A, Wolford JE, Matheo L, Torres O. Trainee perspectives on diversity, equity, and inclusion: a group concept mapping study. Med Educ Online. 2025;30(1):2468936. doi:10.1080/10872981.2025.2468936
- Althans AR, Thompson JR, Rosas SR, et al. Exploring characteristics of academic general surgery residency applicants: a group concept-mapping approach. J Surg Educ. 2022;79(6):1,342-1,352. doi:10.1016/j.jsurg.2022.06.005
- Althans AR, Hashimi B, Rosas S, et al. A group concept mapping approach to understanding barriers to and possible solutions for quality feedback exchange on the surgery clerkship. Global Surg Educ. 2024;3(1):82. doi:10.1007/s44186-024-00282-1
- Hagell P, Edfors E, Hedin G, Westergren A, Hammarlund CS. Group concept mapping for evaluation and development in nursing education. Nurse Educ Pract. 2016;20:147-153. doi:10.1016/j.nepr.2016.08.006



There are no comments for this article.