
With their firsthand understanding of the challenges faced by their patients and a deep appreciation for adaptability and creating solutions, family physicians are needed at every level of leadership in medical education, health care systems, and government.1,2 No single strict path or required personal characteristics exist for successful family physician leadership.3 This project sought to explore characteristics and philosophies common to family physician leaders with the goal of better understanding commonalities and differences.
RESEARCH BRIEF
Characteristics and Philosophies of Family Physician Leaders: A Qualitative Investigation
Sarah E. Stumbar, MD, MPH | Magdalena Pasarica, MD, PhD | Suzanne Minor, MD | Marquita Samuels, MBA | Andres L. Rodriguez, MD
PRiMER. 2026;10:9.
Published: 3/2/2026 | DOI: 10.22454/PRiMER.2026.783608
Introduction: Supported by the Society of Teachers of Family Medicine Special Project Fund, the goal of this hypothesis-generating project was to better understand the characteristics and philosophies of family physicians who hold leadership positions within and beyond the specialty.
Methods: From July 2023 to May 2024, we conducted ten 1-hour semistructured interviews and one five-participant focus group with family physician leaders. Each transcript was analyzed by two researchers, who compiled codebooks. All researchers then met and reviewed the codebooks for all interviews, developing agreed-upon themes and subthemes through an iterative process.
Results: Our 15 interviewees described their careers in terms of personal influences and professional experiences. Identified career-related influences included personal traits, resources, identity, upbringing, and experiences. Interviewees agreed that family medicine training supported leadership preparation through the development of numerous competencies. Participants identified with multiple defined leadership philosophies, all of which reflected a resonant style.
Conclusions: Our findings suggest that no singular characteristics or philosophies are held by all family physician leaders. Identified themes center on collaborative, team-based leadership, which requires strong communication skills and relatability. Many identified themes converged on personal and professional development, as well as support, as essential to leadership growth.
This study was conducted by representatives from the Deans Associated With Family Medicine Special Project Team of the Society of Teachers of Family Medicine (STFM) and supported with funding from the STFM Special Projects Fund. Participants were recruited via email or through the STFM Connect platform; 10 people responded and consented to participate in 1-hour, semistructured, and recorded Zoom interviews (Appendix 1). Five participants were recruited and recorded during a focus group at the 2023 STFM Conference on Medical Student Education. While anyone who self-identified as a family medicine leader was eligible for inclusion in the study, only physicians responded to our calls for participants. Transcripts of the focus group and interviews were generated using ClariVita. The study was determined to be exempt from review by the institutional review boards (IRBs) of Florida International University and the University of Central Florida, citing exemption category 2.
Thematic analysis of the personal narratives was done using the Braun and Clarke method for reflexive analysis.4 Two independent raters coded the data for themes and subthemes; then the themes and subthemes were compared to the point of saturation. Disagreements were discussed with one to three additional reviewers using reflexive discussion, interrogation of different perspectives, and iterative refinement of themes until a consensus was reached.
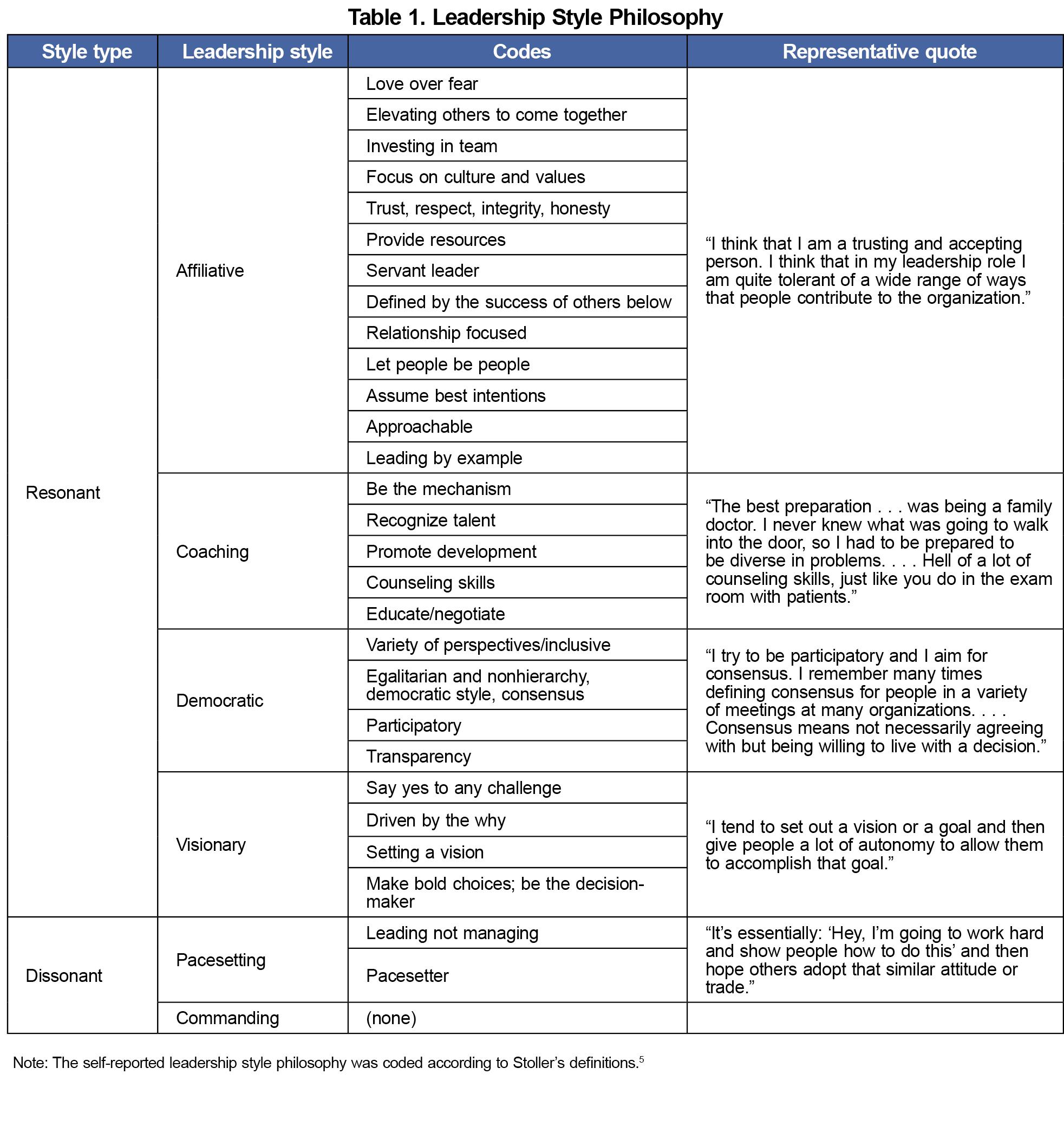
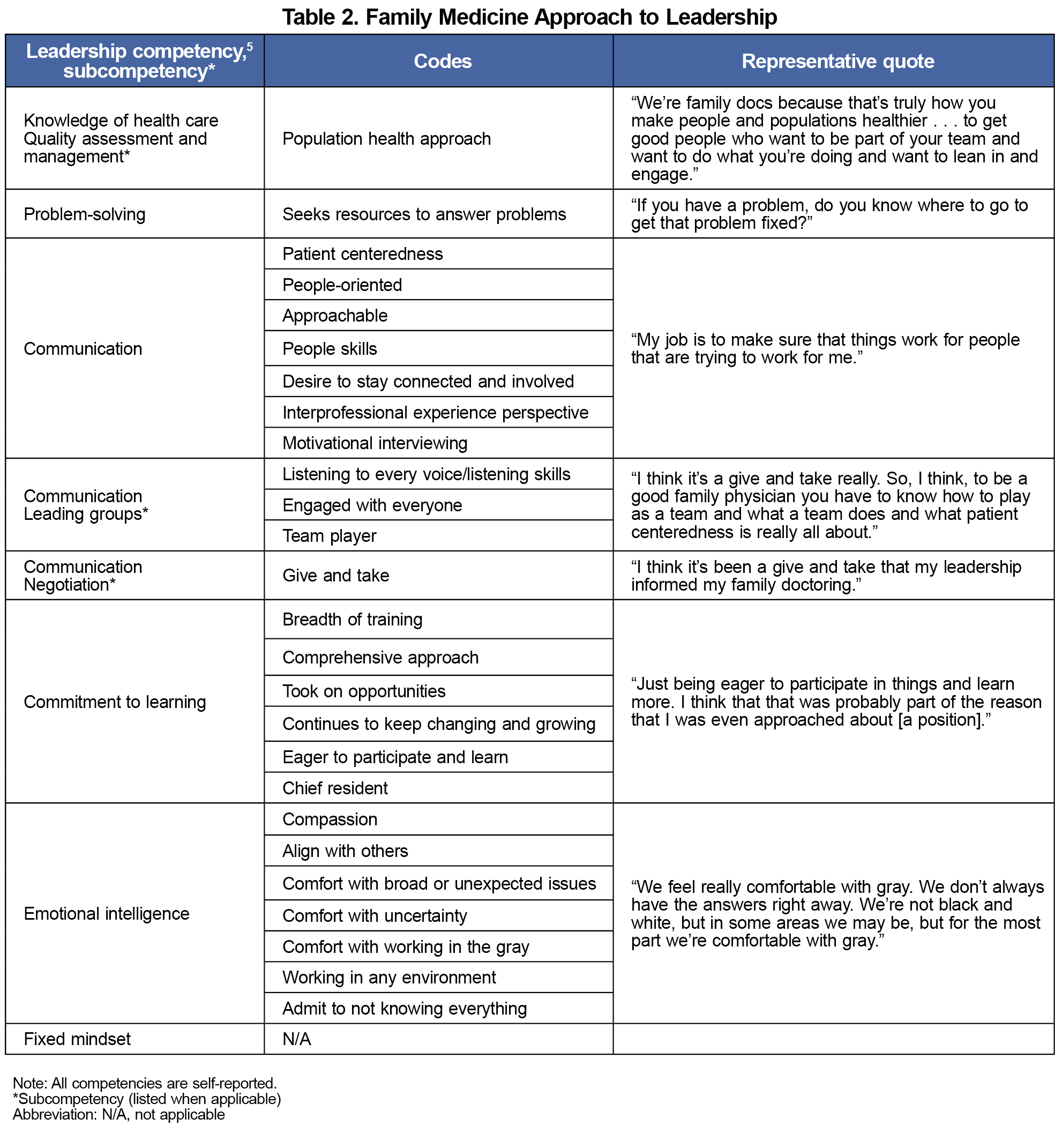
Stoller’s six leadership competencies in health care (technical skill and knowledge, health care systems knowledge, problem-solving skills, emotional intelligence, communication skills, and commitment to lifelong learning) were used as a framework for coding responses to the question “How has family medicine informed your leadership style?”5 Participants’ leadership philosophies were coded as resonant (visionary, coaching, affiliative, democratic) or dissonant (pacesetting, command and control) using Goleman et al’s classification of leadership styles as a framework.6
Participant Demographics
Of the 15 participants, 12 identified as being underrepresented in academic leadership due to their gender, race and ethnicity, or socioeconomic status. Three participants considered themselves underrepresented in academic medicine leadership because they were family physicians. Leaders used numerous titles to describe their identities, with most defining themselves by administrative rank, followed by personal identity. Some also defined themselves by their academic rank or clinical specialty. Additional self-descriptors included personal traits, approaches, and skills. The most cited personal traits were being driven, committed, and hardworking. Other traits mentioned include enthusiasm, honesty, humility, passion, creativity, optimism, thoughtfulness, inspiration, and energy. The three approaches most commonly employed by the leaders were being mission-driven, systematic, and advocating for the team. Interestingly, one participant described themself as introverted. Self-defined leadership skills included being organized, communicating well, delegating efficiently, and developing others while completing tasks on time.
Leadership Positions
The leadership positions held by the participants included those outside the specialty of family medicine (eg, designated institutional official and faculty development) and those within the specialty (eg, chair). Career path decisions primarily were influenced by personal factors, with the most common being family interests and military obligations.
Leadership Style
Overwhelmingly, respondents’ leadership philosophies (Table 1) reflected a resonant style (affiliative, coaching, democratic, visionary), with few responses indicating a dissonant style (pacesetting). No participant supported a commanding style of leadership philosophy. Participants reported that their family medicine training contributed to their leadership style in various ways that aligned with the specialty’s core skills. Identified subthemes all were matched to Stoller’s leadership competencies5 (Table 2, Appendices 2 and 3).
Leadership Development and Contributors
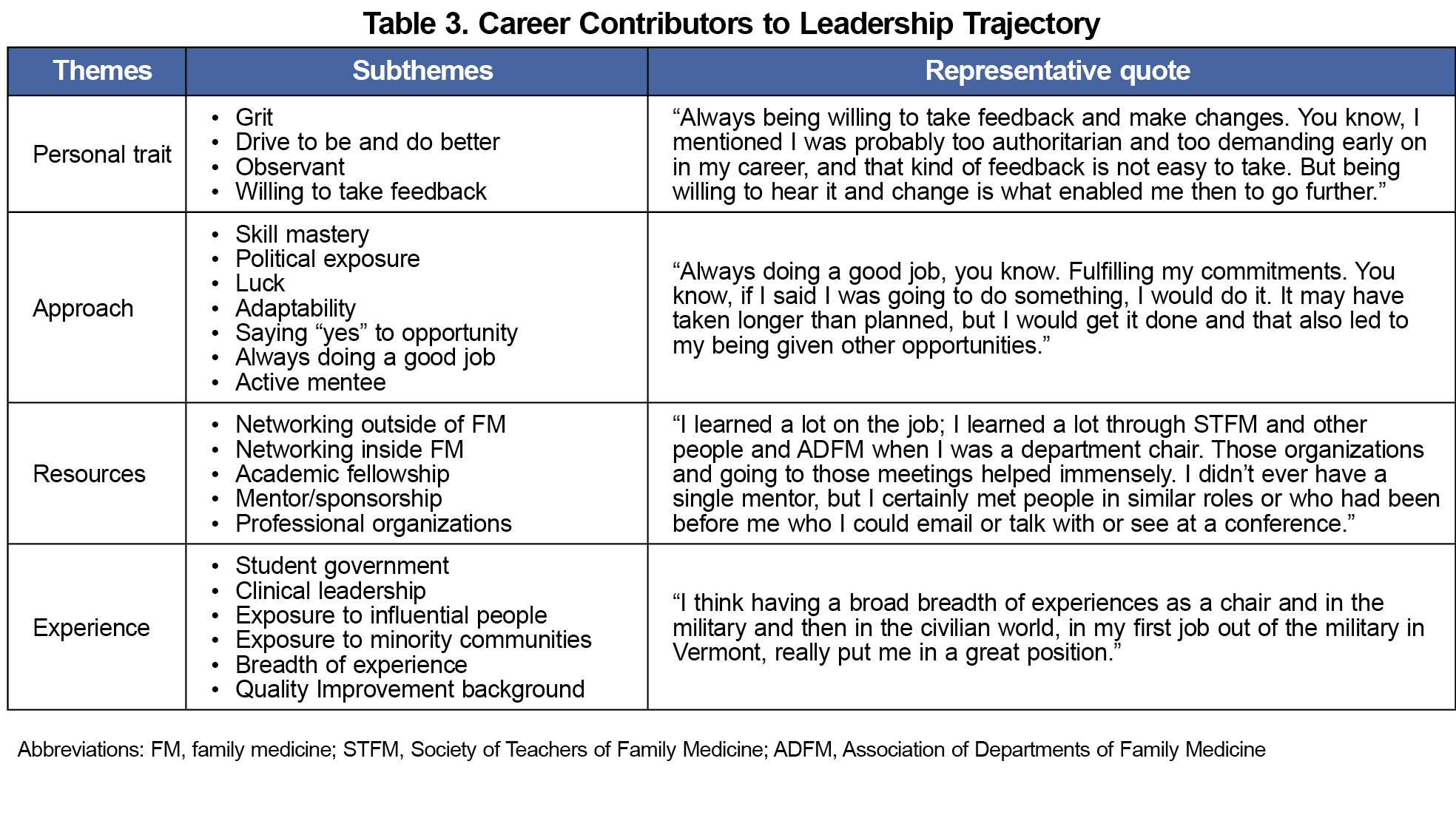
Study participants reported participation in a variety of leadership development activities at the personal, institutional, and national levels. Membership in family medicine–oriented and other national organizations also was noted as important to leadership development. Contributors to career advancement were categorized into four themes: personal traits, approaches, resources, and experiences (Table 3). The theme of resources was cited almost twice as often as the next most frequently cited themes, approach and personal traits. Within the resources theme, mentors and access to networks were cited as the most frequent contributors. When asked what mission helped them become successful leaders, participants identified teaching and clinical work slightly more frequently than service and research (Appendices 4, 5, and 6).
Barriers
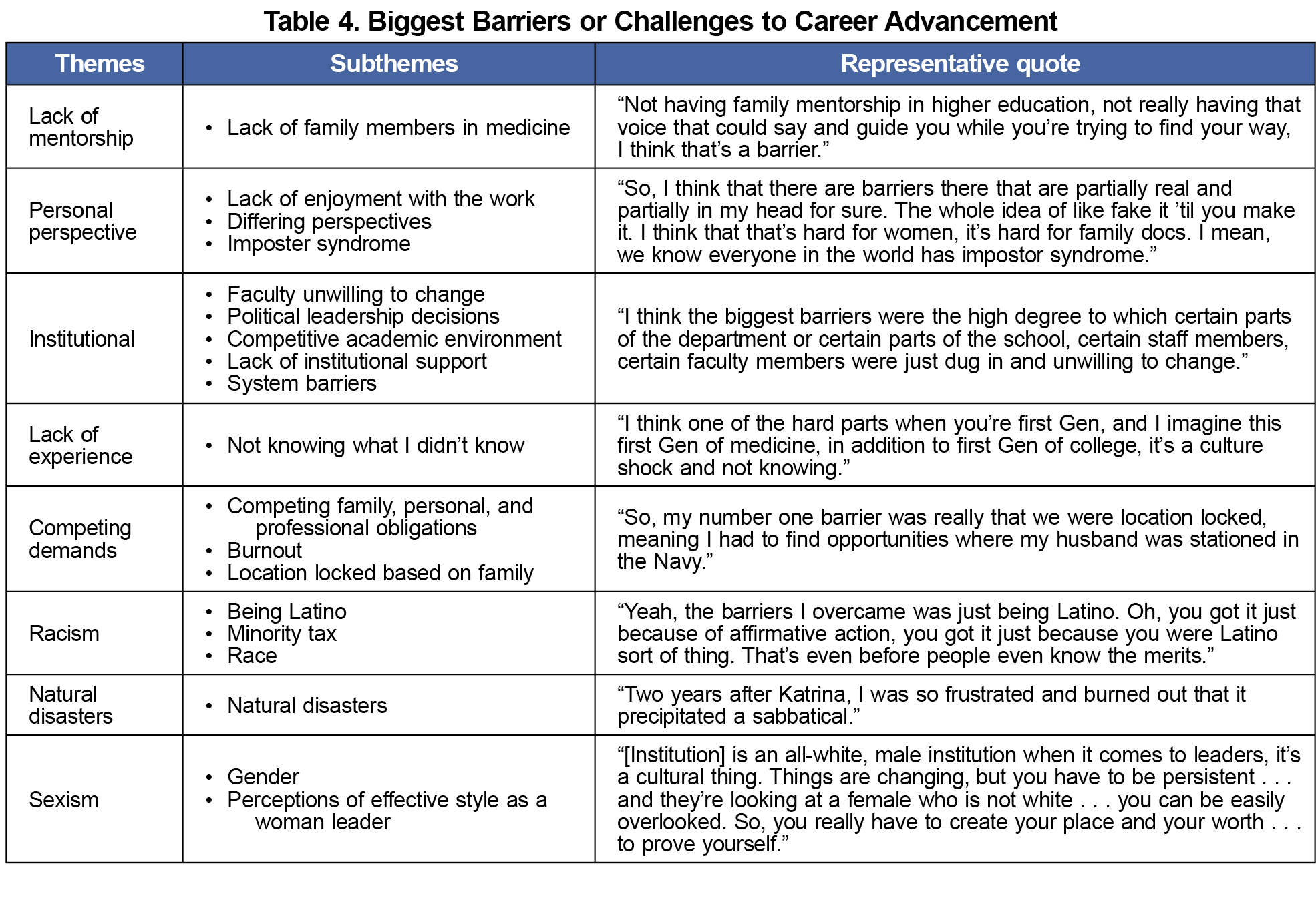
Study participants reported a variety of personal barriers to leadership (Table 4, Appendix 7), including a lack of early mentorship, limited experience, and competing demands. Societal barriers included themes related to natural disasters, racism, and sexism. Professional barriers included themes related to institutional challenges.
Leadership and Identity
Our study found that family physician leaders have dual professional and personal identities, as evidenced by the abundance of personal and professional titles and descriptors that they used when asked to describe themselves. Three participants identified themselves as underrepresented in academic medicine leadership because of their specialty, suggesting that some family physicians may feel isolated in high-level leadership positions. While loneliness or isolation may be multifactorial and common among leaders, little research has examined feelings of loneliness specifically among physician leaders; this presents a possible area for future study.7
Participants most frequently reported feeling underrepresented in academic medicine leadership because of their gender, a finding supported by the literature. While a 2019 investigation of specialty, gender, and race/ethnicity of deans of allopathic schools demonstrated an increase in the percentage of women deans to 18%, women continue to be underrepresented at the highest levels of academic medicine leadership.8
We found no common leadership position among the study participants, with interviewees noting positions equally within and outside of family medicine. Our findings are limited to physicians, as we had no participants with backgrounds in other training fields. Physicians’ career decisions were most influenced by personal factors, suggesting that personal and familial support may need to be combined with professional development to facilitate career advancement. Not surprisingly, family physician leaders overwhelmingly describe resonant leadership styles, which align with the values and ethos of family medicine training.
Leadership and Professional Development
Family physician leaders reported participating in numerous leadership development opportunities, both within and outside the specialty, at various stages of their professional timeline, including early in their careers and at career turning points. Membership in professional organizations was noted as important to leadership development, likely because these memberships may lead to opportunities for involvement in task forces, committees, or other programs. Most interviewees emphasized the importance of mentorship and access to networks for career advancement. Additionally, teaching, clinical, and research missions equally impacted leadership experiences. This finding supports the idea that the diversity of the specialty of family medicine helps build leaders—people who lead collaboratively and build alliances within and between teams, much like the alliance between a family physician and a patient.
Limitations
While factors such as race, ethnicity, sex, gender, and age are well-known to influence leadership philosophy and career opportunities, given the small sample size, the need for anonymity for participants, and the exploratory nature of our study, we chose not to focus on detailed and categorized demographic data of our interviewees. Additionally, the generalizability of our findings may be limited because all participants were recruited through STFM; family physicians outside this network may have different experiences, characteristics, and philosophies. Given the qualitative nature of our study, all information was self-reported; perceptions of leadership styles may be influenced by self-perception and bias. Additionally, we allowed leaders to self-identify, thereby resulting in interviews of people across a spectrum of leadership positions; a future study limited to one role (eg, medical school deans) may provide more consistent or nuanced findings. Furthermore, while the initial intention of this study was to examine the experiences of all family medicine leaders, only physicians responded to our recruitment efforts, thereby limiting our study findings to family physician leaders.
Our qualitative, hypothesis-generating study suggests that no singular skill set, philosophy, or characteristic is required for family physicians to obtain leadership positions. Future research should explore the characteristics and philosophies of family physicians in distinct roles, such as deans, chief executive officers, and designated institutional officials, as well as the leadership experiences of family medicine leaders who are not physicians. This research could help support the diverse training backgrounds of those who contribute to the specialty of family medicine and enable family physicians to make informed choices aligned with their unique skills, philosophies, and characteristics, ultimately enhancing their leadership trajectories.
Acknowledgments
Conflict of Interest Statement:
While not a conflict, this project was supported with funding from the Society of Teachers of Family (STFM) Special Projects Fund and conducted by representatives from the STFM Deans Associated With Family Medicine Special Project Team. No other actual or perceived conflicts of interest exist for any of the authors.
References
- Elliott TC, Li L. The legacy of leadership: our commitment to future generations of family medicine leaders. Fam Med. 2021;53(1):78-79. doi:10.22454/FamMed.2021.869496
- Muramoto M, Rankin P, Rodgers AD. Leadership development for the future of family medicine: training essential leaders for health care. Fam Med. 2021;53(7):650-653. doi:10.22454/FamMed.2021.125016
- Coe C, Piggott C, Davis A, et al. Leadership pathways in academic family medicine: focus on underrepresented minorities and women. Fam Med. 2020;52(2):104-111. doi:10.22454/FamMed.2020.545847
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101. doi:10.1191/1478088706qp063oa
- Stoller JK. Leadership essentials for CHEST medicine professionals: models, attributes, and styles. Chest. 2021;159(3):1,147-1,154. doi:10.1016/j.chest.2020.09.095
- Goleman D, Boyatzis RE, McKee A. Primal Leadership: Learning to Lead With Emotional Intelligence. Harvard Business School Press; 2004.
- Gilchrist V, Schrager S. Loneliness and leadership. Fam Med. 2025;57(10):688-689. doi:10.22454/FamMed.2025.641645
- Nobles A, Martin BA, Casimir J, Schmitt S, Broadbent G. Stalled progress: medical school dean demographics. J Am Board Fam Med. 2022;35(1):163-168. doi:10.3122/jabfm.2022.01.210171
Lead Author
Sarah E. Stumbar, MD, MPH
Affiliations: Herbert Wertheim College of Medicine, Florida International University, Miami, FL
Co-Authors
Magdalena Pasarica, MD, PhD - College of Medicine, University of Central Florida, Orlando, FL
Suzanne Minor, MD - Memorial Healthcare System, Hollywood, FL
Marquita Samuels, MBA - Herbert Wertheim College of Medicine, Florida International University, Miami, FL
Andres L. Rodriguez, MD - Herbert Wertheim College of Medicine, Florida International University, Miami, FL
Corresponding Author
Sarah E. Stumbar, MD, MPH
Correspondence: Herbert Wertheim College of Medicine, Florida International University, Miami, FL
Email: sstumbar@fiu.edu
Fetching other articles... 
Loading the comment form...
Submitting your comment...

There are no comments for this article.