Introduction: Decades of social norms research has highlighted the tendency for individuals to adjust their behaviors based on their reference (or peer) group. Often, inaccuracies in perceptions (eg, self-other difference [SOD]) can increase or decrease one’s behavior over time. In medical residency, SODs related to perceptions of others’ behaviors predicted the individuals’ who reported bullying behavior, a concerning behavior that is common in medicine. The goal of this study was to expand on previous research examining normative perceptions of bullying and negative acts in medicine.
Methods: This study used the 2025 Council of Academic Family Medicine Educational Research Alliance (CERA) survey of family department chairs. This survey was distributed to 197 family medicine department chairs in addition to other staff within the family medicine education department. Measures included perceived risk of experiencing retaliation and questions measuring perceived norms, which were used to calculate SODs.
Results: We assessed differences in perceptions (SODs) using t tests. Our analyses suggested that family medicine chairs significantly overestimated the frequency with which peers addressed negative acts but believed that others were less approving of addressing negative acts. We examined predictors of reporting using multiple linear regression. SOD predicted the individual’s tendency to report addressing negative acts.
Conclusions: This study expanded on previous research in family medicine and suggested that family medicine department chairs also have inaccurate peer perceptions of attitudes and behaviors related to bullying behavior. Future research might examine the use of social norms interventions as a mechanism to address bullying behavior in family medicine.
Decades of research on social norms has highlighted the tendency for individuals to adjust their behaviors based on their reference group.1-3 Norms can be categorized as either descriptive norms, referring to how often behavior occurs; or injunctive norms, perceptions of how acceptable a behavior is. Often, a discrepancy exists between what one believes others are doing compared to reality, defined as a self-other difference (SOD). Individuals who believe others are more frequently engaging in and/or are more approving of a behavior will increase their own behavior over time and vice versa.3-5
Medical professionals often work within a culture that emphasizes self-criticism and defers personal well-being.6-9 Negative acts or bullying in medical settings have been linked to job dissatisfaction, higher rates of burnout, and workplace errors.10,11
Effective responses to bullying or negative acts depend on the reporting of negative behaviors. In addition, leaders in medical settings are influential in shaping culture and policy, and their approaches and beliefs regarding reporting behavior can impact those around them.12 The primary goal of this study was to expand on previous research conducted in medical education13,14 by examining normative perceptions among a national sample of family medicine department chairs.
Data were obtained as part of the 2025 Council of Academic Family Medicine Educational Research Alliance (CERA) survey of family medicine department chairs. The study was approved by the American Academy of Family Physicians Institutional Review Board in October 2024, and the protocol has been detailed in previous publications.13
The survey was distributed to 197 family medicine department chairs (45.7% response rate) and has been previously distributed among individuals working in family medicine education.14
Measures
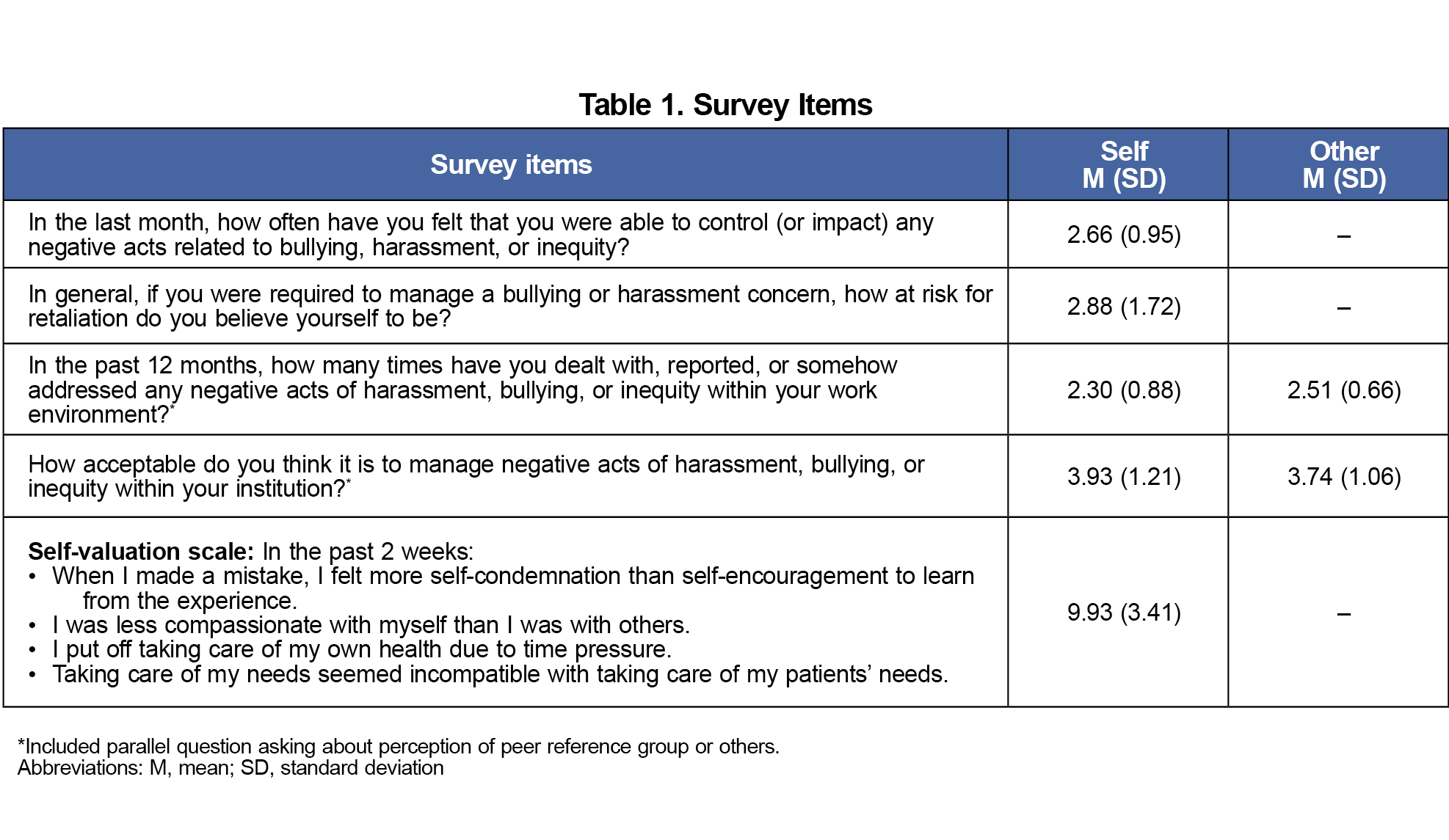
Questions included demographic information, perceived risk of experiencing retaliation, and perceived norms related to reporting bullying behavior (Table 1). Respondents also completed the self-valuation scale (ɑ=.82).15
Analysis Plan
We calculated SODs for both injunctive and descriptive norms by taking the participant’s own norm rating and subtracting the average perceived norm of their reference group. We used independent t tests to evaluate the accuracy of descriptive and injunctive estimates.
We used multiple linear regression to determine whether SODs predicted respondents’ tendency to address negative acts or bullying behaviors. We used perceived risk and perceived control as covariates, consistent with other studies13,16; and we used the theory of planned behavior, which suggests that these factors are predictors of behavioral intention.
We conducted exploratory analyses using linear regression to examine possible associations between (a) attitudes toward bullying and self-valuation, and (b) gender identity, URiM status, and risk of retaliation.
Participants
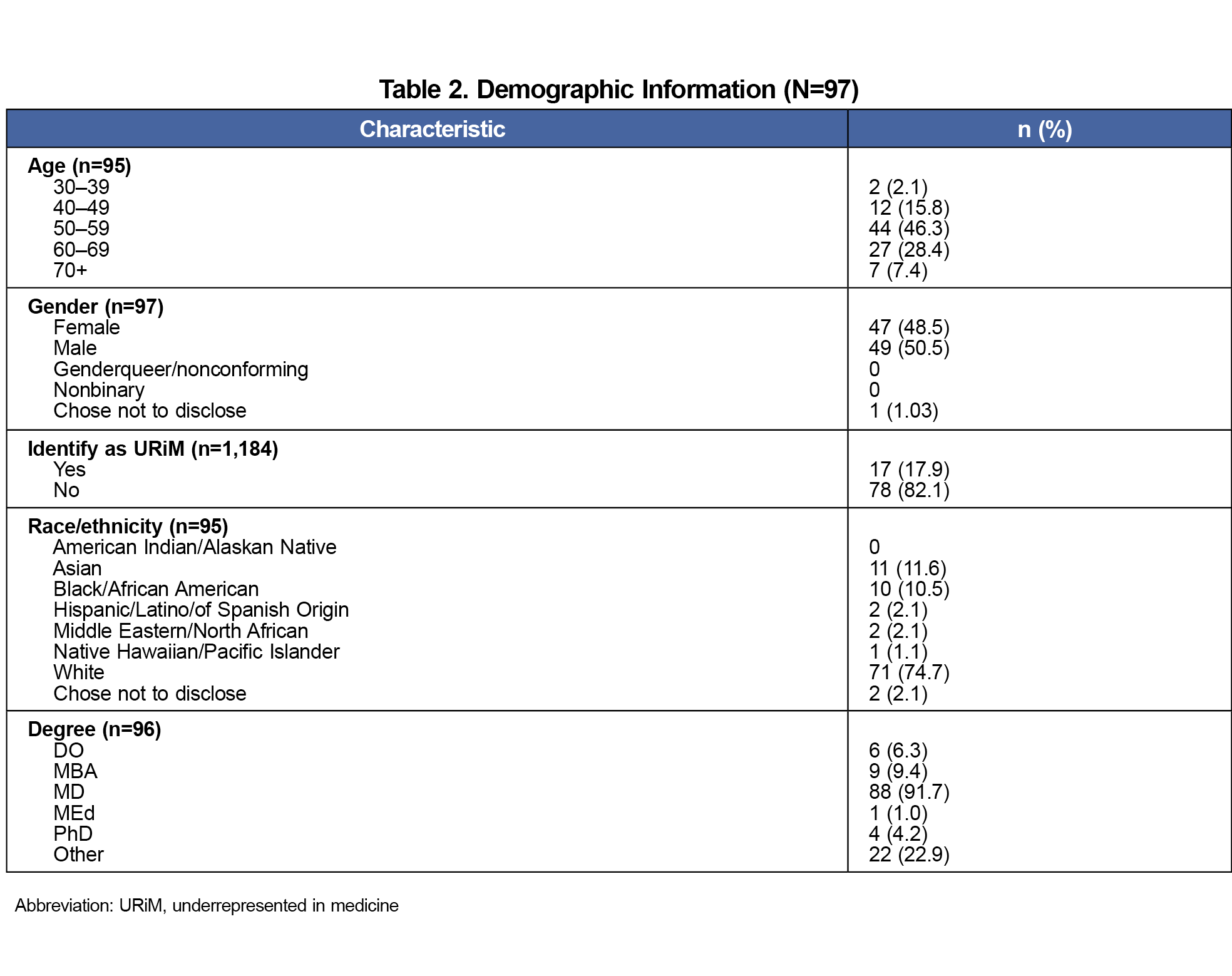
Respondents included 97 family medicine department chairs who were primarily male (n=49, 50.1%), between 50 and 59 years old (n=44, 46.3%), allopathic doctors (n=88, 91.7%), and identified as white (n=71, 74.7%; Table 2).
Accuracy of Normative Estimates
Self-reported behavioral estimates of addressing negative acts in the work environment were infrequent (M=2.30, SD=0.88, 1=never), with neutral to somewhat positive attitudes about doing so (M=3.93, SD=1.21, 5=completely acceptable). Respondents believed that they did not address bullying as frequently as their peers did; t(85)=–2.43, P=.02, d=0.27. They also believed peers were less approving of addressing negative acts in the workplace; t(84)=2.62, P=.01, d=0.17.
Perceived Descriptive Norms (Behaviors)
SODs of descriptive norms (eg, individual’s rating minus average perceived norm of their reference group) were an independent predictor of reporting negative acts; β=–.49, t(79)=–5.46, P<.01. The greater the SOD, the less likely individuals were to report bullying.
Perceived Injunctive Norms (Attitudes)
SODs of injunctive norms independently predicted reporting negative acts; β=–.49, t[79]=–10.61, P<.01. The greater the difference in perception in others’ attitudes, the less likely individuals were to report bullying themselves.
Self-Valuation and Attitudes Toward Reporting Bullying
The degree of self-valuation, or the tendency to engage in self-compassionate behavior, was not significantly associated with attitude toward reporting bullying behavior; F(1, 82)=3.18, β=.19, t(82)=1.78, P=.08.
Perceptions of Retaliation Risk: Women and URiM
Results that trended toward significance, such that those that identified as female, were more likely to report concerns of risk of retaliation; β=–.68, t(82)=–1.88, P=.06. We found no significance for those who identified as URiM (underrepresented in medicine) compared to those who did not identify as URiM.
This study expanded on existing research in several ways.13 It confirmed that negative acts are addressed relatively infrequently, and department chairs view others as less accepting of addressing negative acts in the workplace.
First, department chairs indicated that they addressed negative acts in their departments relatively infrequently. Taken in the context of previous research that suggests negative acts or bullying are a relatively common occurrence in medicine, this finding raises questions about why department chairs reported that they did not often address negative acts.10,16,17 Future research might further examine the relationship between actual and reported negative acts to better understand discrepancies in the frequency with which they occur and the subsequent responses to those behaviors.
Second, consistent with other research exploring normative estimates in rural medical residents and family medicine faculty and staff,14,18 we found significant differences in respondents’ reports of their own behavior and beliefs compared to their estimates of peers (as measured by SODs). Family medicine department chairs overestimated how often their peers addressed concerns and underestimated how accepting their peers were of addressing negative acts in the workplace. Future research might examine the behaviors and beliefs of those in other leadership positions, such as higher organizational administrative positions, associate program directors, or chief residents.
Third, this study expanded on previous findings in which the SODs (ie, degree of misperception within the individual) predicted the likelihood of addressing negative acts.14,19 Specifically, those who believed they were more different than their peers reported a lower frequency of responding to negative acts or bullying. Researchers have speculated that the maladaptive culture of medicine, which often involves deferral of self-care,7,9,20,21 may drive some of these social perceptions. Use of social norms interventions may be one way to shift these beliefs.22 Interventions that modify medical peers’ perception of others’ reporting behavior and others’ attitudes toward it may encourage individuals in leadership to change their own behavior over time.
Finally, exploratory analyses were not significant; however, the study may have been underpowered to detect effects seen in previous research.14 A small sample size reflects one of several limitations that should be noted of the present study. In addition to a limited sample size, results may be vulnerable to a voluntary response bias, such that those who completed the survey may not be representative of all department chairs. This study was correlational and therefore cannot address questions of causality. Lastly, survey data relied on self-reporting. Future research might include objective measures of reporting (eg, documented cases).
By focusing on perceptions, this study expanded on previous research in family medicine. Negative acts in medicine are commonplace, and understanding attitudes and behaviors of those in leadership positions provides additional insight into factors that may affect decisions to report such incidents. Future research might examine the use of social norms interventions as a mechanism to address bullying behavior in family medicine.
References
- Borsari B, Carey KB. Descriptive and injunctive norms in college drinking: a meta-analytic integration. J Stud Alcohol. 2003;64(3):331-341. doi:10.15288/jsa.2003.64.331
- Gerber AS, Rogers T. Descriptive social norms and motivation to vote: everybody’s voting and so should you. J Polit. 2009;71(1):178-191. doi:10.1017/S0022381608090117
- Neighbors C, Lewis MA, Atkins DC, et al. Efficacy of web-based personalized normative feedback: a two-year randomized controlled trial. J Consult Clin Psychol. 2010;78(6):898-911. doi:10.1037/a0020766
- Wenzel M. Misperceptions of social norms about tax compliance: from theory to intervention. J Econ Psychol. 2005;26(6):862-883. doi:10.1016/j.joep.2005.02.002
- Huber J, Viscusi WK, Bell J. Dynamic relationships between social norms and pro-environmental behavior: evidence from household recycling. Behav Public Policy. 2020;4(1):1-25. doi:10.1017/bpp.2017.13
- McClafferty HH, Hubbard DK, Foradori D, Brown ML, Profit J, Tawfik DS; Section on Integrative Medicine. Physician health and wellness. Pediatrics. 2022;150(5):e2022059665. doi:10.1542/peds.2022-059665
- Shanafelt TD, Schein E, Minor LB, Trockel M, Schein P, Kirch D. Healing the professional culture of medicine. Mayo Clin Proc. 2019;94(8):1,556-1,566. doi:10.1016/j.mayocp.2019.03.026
- Dyrbye LN, Eacker A, Durning SJ, et al. The impact of stigma and personal experiences on the help-seeking behaviors of medical students with burnout. Acad Med. 2015;90(7):961-969. https://academic.oup.com/academicmedicine/issue/90/7
- Terry DL, Safian G, Terry CP. Patterns and consequences of delayed self care among rural medical providers. Am J Health Promot. 2025;39(1):122-126. doi:10.1177/08901171241266401
- Paice E, Smith D. Bullying of trainee doctors is a patient safety issue. Clin Teach. 2009;6(1):13-17. doi:10.1111/j.1743-498X.2008.00251.x
- Samsudin EZ, Isahak M, Rampal S. The prevalence, risk factors and outcomes of workplace bullying among junior doctors: a systematic review. Eur J Work Organ Psychol. 2018;27(6):700-718. doi:10.1080/1359432X.2018.1502171
- Armit K. Evidence, culture and clinical outcome. Future Hosp J. 2015;2(3):194-196. doi:10.7861/futurehosp.2-3-194
- Ho T, Ringwald B, Walker P, Paladine H, Biggs R, Moore M. Methodology and past topics for the 2025 CERA department chair survey. PRiMER. 2026;10:4. doi:10.22454/PRiMER.2026.578247
- Terry DL, Graham J, Moore MA, Terry CP, Williamson M. Bullying, social norms, and reporting behavior among medical training programs: a national survey. Fam Med. 2026;58(1):27-33. doi:10.22454/FamMed.2026.526733
- Trockel MT, Hamidi MS, Menon NK, et al. Self-valuation: attending to the most important instrument in the practice of medicine. Mayo Clin Proc. 2019;94(10):2,022-2,031. doi:10.1016/j.mayocp.2019.04.040
- Fnais N, Soobiah C, Chen MH, et al. Harassment and discrimination in medical training: a systematic review and meta-analysis. Acad Med. 2014;89(5):817-827. https://academic.oup.com/academicmedicine/issue/89/5
- Chadaga AR, Villines D, Krikorian A. Bullying in the American graduate medical education system: a national cross-sectional survey. PLoS One. 2016;11(3):e0150246. doi:10.1371/journal.pone.0150246
- Terry DL, Mathews DP. Social norms and engagement in protective health behaviors among rural health providers. J Clin Psychol Med Settings. 2022;29(2):384-390. doi:10.1007/s10880-022-09845-0
- Terry DL, Williamson MLC. Bullying among medical residents: gender, social norms, and reporting behavior. PRiMER. 2022;6:17. doi:10.22454/PRiMER.2022.824936
- Wessely A, Gerada C. When doctors need treatment: an anthropological approach to why doctors make bad patients. BMJ. 2013;347:f6644. doi:10.1136/bmj.f6644
- Balch CM, Shanafelt TS. Dynamic tension between success in a surgical career and personal wellness: how can we succeed in a stressful environment and a “culture of bravado”? Ann Surg Oncol. 2011;18(5):1,213-1,216. doi:10.1245/s10434-011-1629-z
- Cislaghi B, Berkowitz AD. The evolution of social norms interventions for health promotion: distinguishing norms correction and norms transformation. J Glob Health. 2021;11:03065. doi:10.7189/jogh.11.03065



There are no comments for this article.