Introduction: The Council of Academic Family Medicine (CAFM) Educational Research Alliance (CERA) aims to promote family medicine research. Each year, the members of the four CAFM organizations submit audience-specific survey questions. This paper reviews the methods and demographics of the 2025 General Membership Survey and determine the representativeness of the survey respondents.
Methods: CERA opened its call for the annual General Membership Survey proposals in August 2025. Fourteen proposals underwent a peer-review process, with five selected for inclusion in the omnibus survey. CAFM members received invitations to complete the survey via SurveyMonkey between October 6, 2025 and November 14, 2025. Demographics of potential survey respondents were compared to demographics of the actual survey respondents using Fisher’s exact tests with an α of 0.05.
Results: Of the 3,834 CAFM members invited to participate, 884 responded, yielding a response rate of 23.1%. After removing missing data and “choose not to disclose” responses, fewer actual respondents self-identified as underrepresented in medicine compared to potential respondents (16.0% vs 19.4%, P<.001), and actual respondants more often had PhDs as their primary degree (11.5% vs 7.4%, P<0.001) compared to nonrespondents. Age and state/province of practice/program were not significantly different between respondents and nonrespondents. We did not perform statistical analysis on gender and race/ethnicity due to response options lacking mutual exclusivity. Gender showed similar distributions whereas race/ethnicity had a higher percentage of White respondents (75.7% vs 68.9%) and lower Black/African American respondents (4.9% vs 7.6%) between respondents and nonrespondents.
Conclusion: CERA explores topics vital to family medicine education, enabling stakeholders to develop informed policies important to family medicine education.
The Council of Academic Family Medicine (CAFM) Educational Research Alliance (CERA) seeks to develop a unified infrastructure to promote medical education research and collaboration in family medicine.1–4 CERA receives financial and staffing support from the Association of Departments of Family Medicine (ADFM), the Association of Family Medicine Residency Directors (AFMRD), the North American Primary Care Research Group (NAPCRG), and the Society of Teachers of Family Medicine (STFM).1 The distribution of recipients by organization is split into two groups, with members holding multiple memberships labeled as “STFM”. Of the 3,834 members who received the survey, 183 belonged to ADFM and 3,651 to STFM.
CERA performs comprehensive, generalizable research in family medicine education by regularly surveying targeted groups, including family medicine department chairs, residency program directors, clerkship directors, and members. These surveys cover areas like clinical care, curriculum development, public policy, and medical education. In addition to conducting research, CERA offers mentorship and training to CAFM members on educational research methods.
The annual General Membership (GM) Survey engages a diverse audience, including family physicians, pharmacists, behavioral health professionals, administrators, and researchers. It combines member-submitted questions with standard demographic and organizational queries. This paper outlines the methods and demographics of the 2025 GM Survey.
The 2025 call for GM Survey proposals was open from May 19, 2025 to June 17, 2025. Of the 14 proposals received, five were selected following a peer-review process. The peer-review process involved having all submitted surveys evaluated by reviewers selected from the CERA reviewer pool. The review criteria included domains of interest of the topic, background and significance, hypothesis-driven, publishability, and question quality. Reviewers were given 4 weeks to submit their scores for each domain and overall. At least three reviewers were assigned to each survey, and scores were averaged to make a final score. The top four highest-scoring surveys were selected. Two surveys were tied with the same score, and the CERA GM Survey Director (author A.Z.) chose between the two based on overall reviewer comments and timeliness of the topics. Each accepted proposal underwent revisions after feedback from mentors, the GM Survey Director, and a CERA Research Fellow. The final questions were piloted by the GM Survey Director and four academic family physicians to ensure validity, clarity, and readability. CAFM members were invited to complete the survey via SurveyMonkey from October 6, 2025, to November 14, 2025. The American Academy of Family Physicians’ Institutional Review Board approved the study on September 25, 2025.
Sample
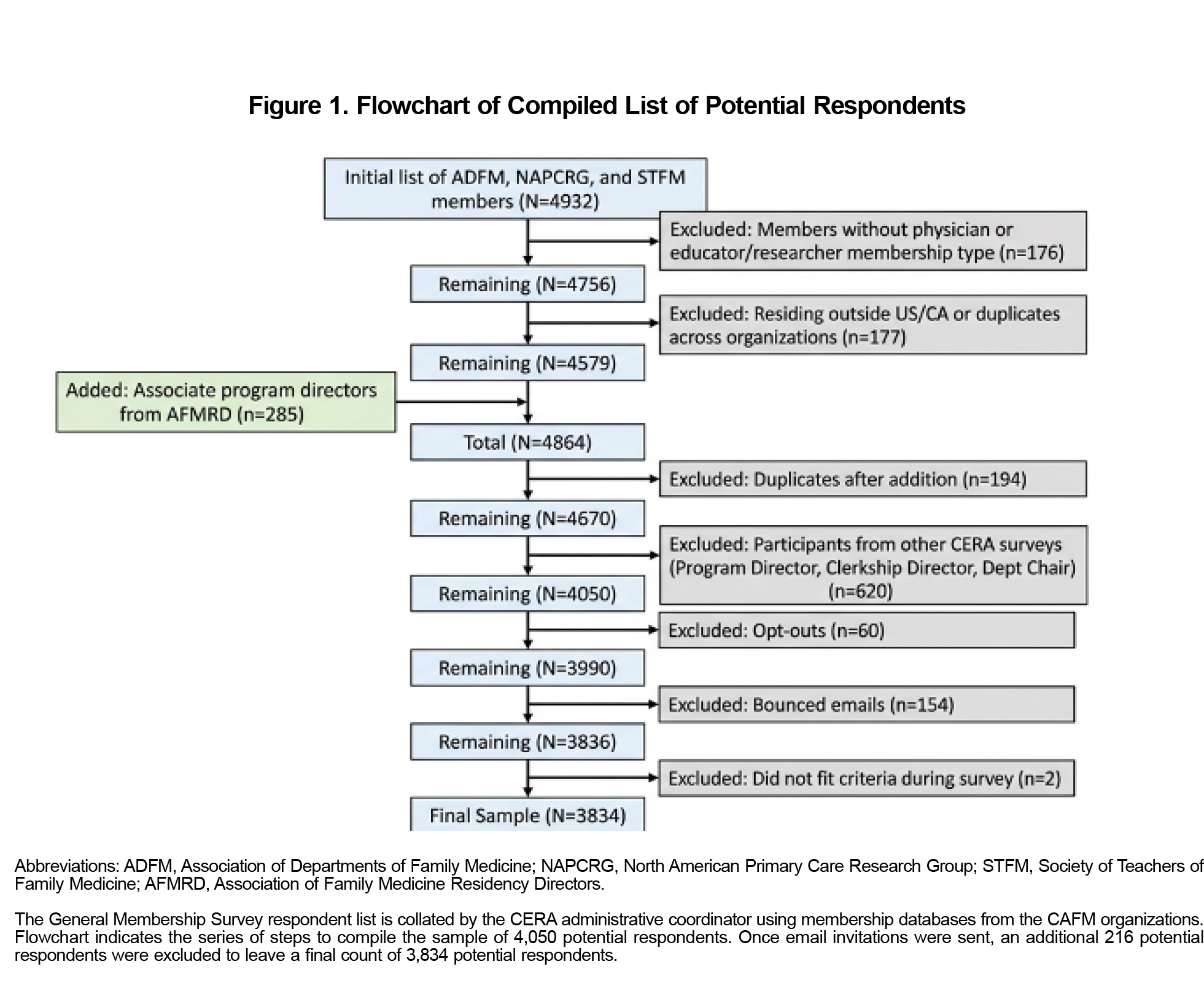
The sample pool was based on CAFM-affiliated organization membership type in the United States and Canada, excluding international, lifetime, emeritus, patient/community, student, resident, program director, clerkship director, and department chair members. The goal of the sample was to capture physician and educator/researcher members who did not participate in the other CERA surveys in 2025 (Figure 1). The demographics of the sample pool were derived from membership data obtained from ADFM, STFM, and NAPCRG, since demographic data from AFMRD was unavailable. For individuals with multiple memberships, demographic information was obtained from their STFM membership record.
The initial pool of potential respondents was 4,050 individuals. We excluded two members who indicated they did not fit the criteria of the survey, 60 individuals who opted out of surveys from SurveyMonkey, and 154 surveys were returned as undeliverable email addresses. The final pool of potential respondents was 3,834 individuals. Nonrespondents received a total of five reminders, one for each week the survey was open.
Analysis
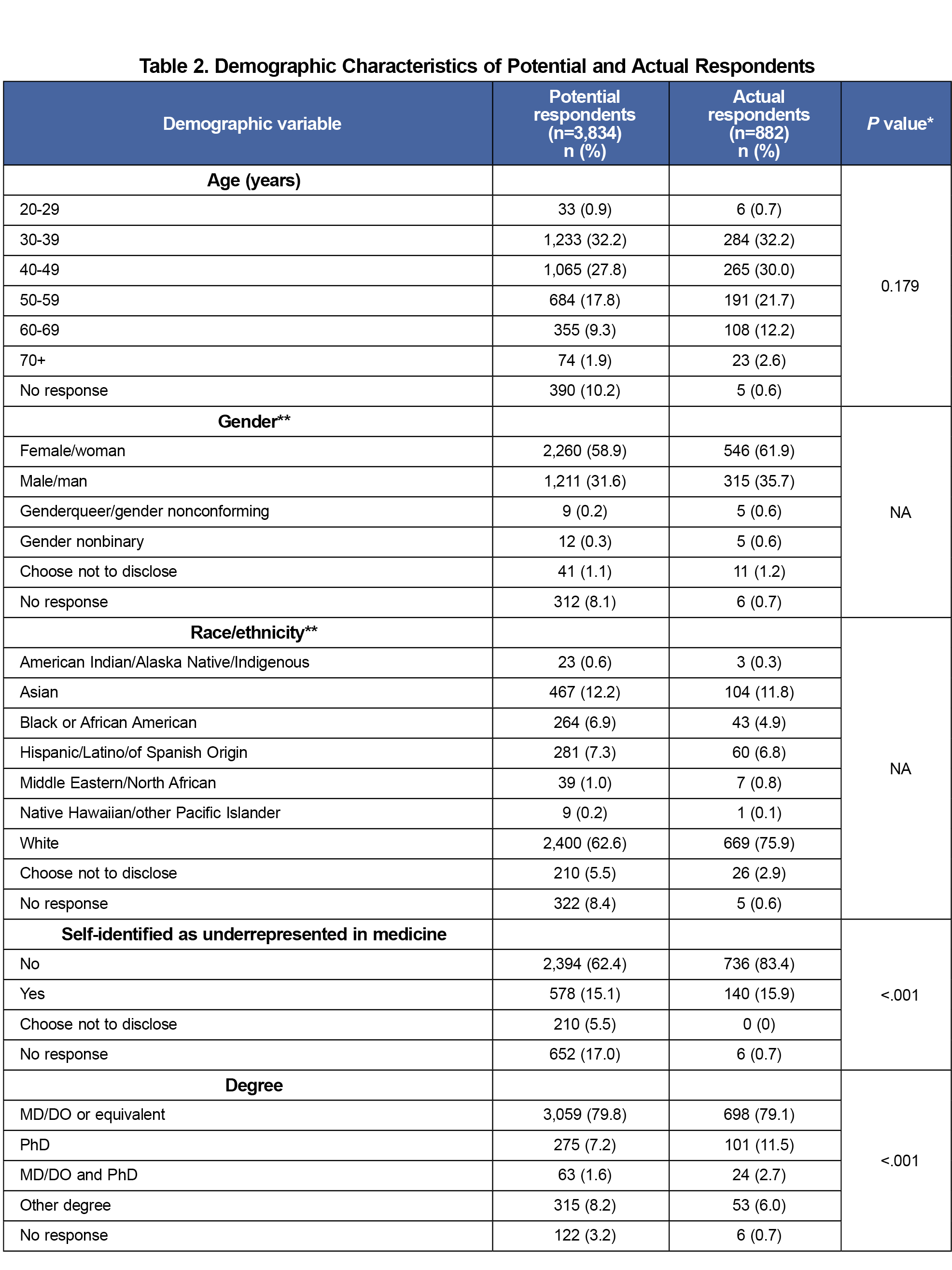
We calculated descriptive statistics, including frequencies and percentages, and we used Fisher’s exact tests to compare potential versus actual respondents, excluding the options of “No Response” and “Choose not to disclose.” We calculated comparisons at the demographic variable level. No statistical analysis was performed on gender and race/ethnicity due to the question response options not being mutually exclusive. We used a significance threshold of 0.05 for all two-sided statistical tests conducted using Stata SE18 software (STATA Corp, College Station, TX).
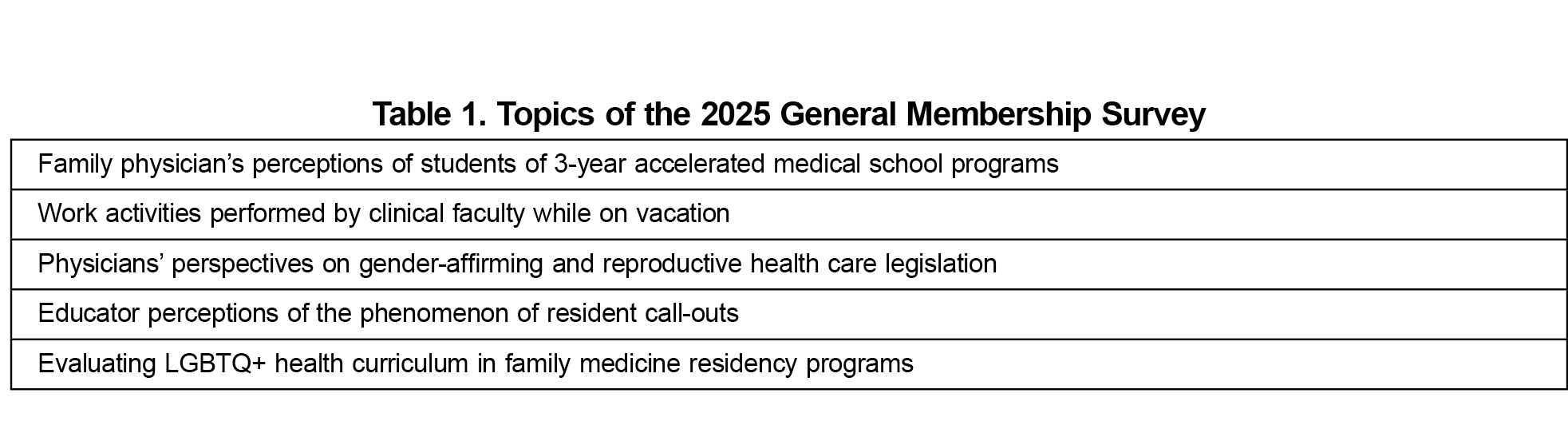
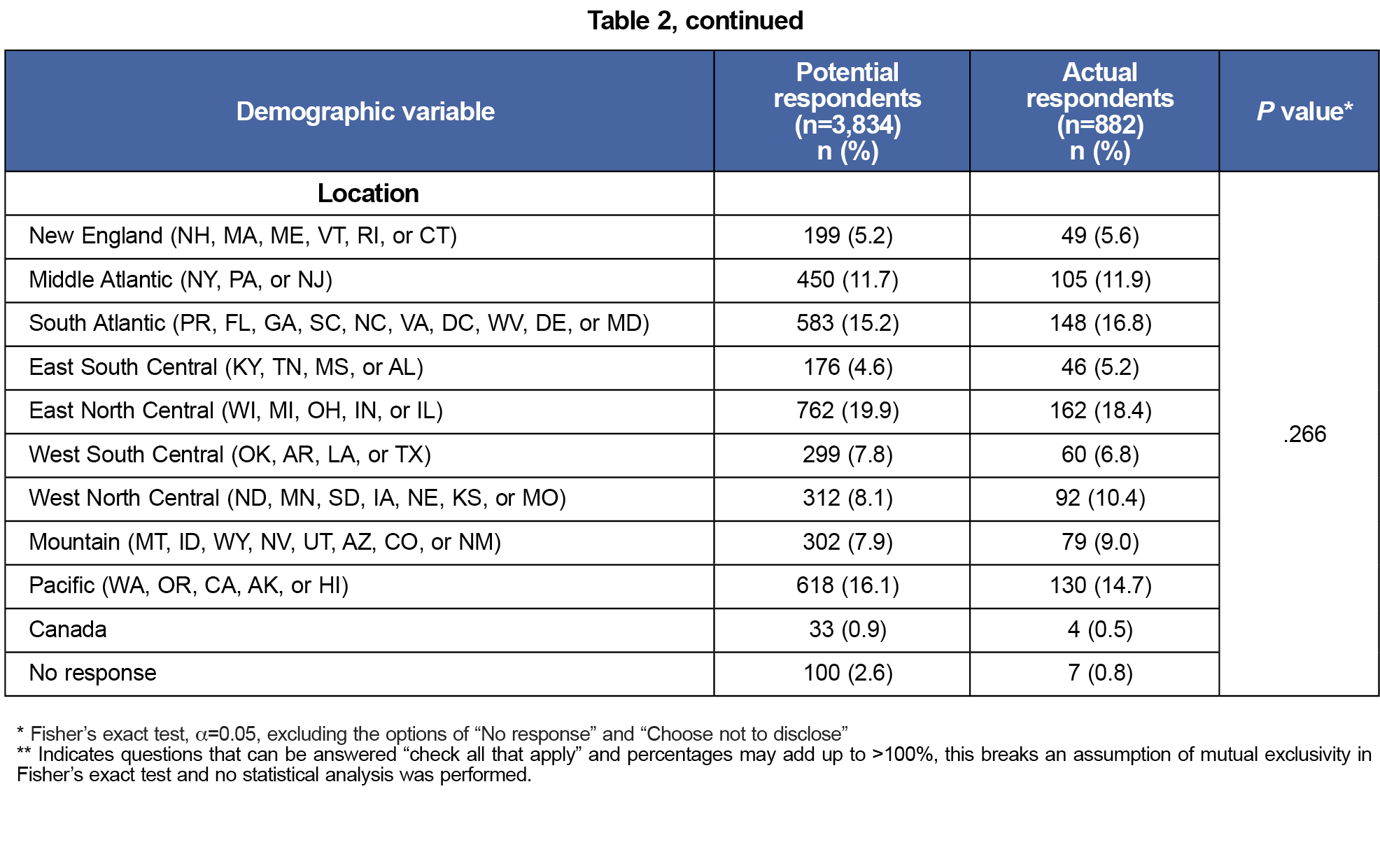
The topics of the accepted proposals are shown in Table 1. Of 3,834 potential respondents (Figure 1), 882 individuals completed the survey, resulting in a 23.1% response rate. While age (P=.179) and location (P=.266) were not statistically significant, the remaining categorical variables had statistically significant differences (Table 2). Compared to potential respondents, actual survey respondents were more likely to be White (75.9% vs 62.6%) and self-identify as not underrepresented in medicine (83.4% vs 19.4%, P<.001). “Underrepresented in medicine” was defined according to the Association of American Medical Colleges description and was self-identified by respondents in member databases. Respondents were also more likely to report a PhD as their primary degree (11.5% vs 7.2%, P<.001).
CERA aims for excellence in family medicine educational research by establishing a centralized infrastructure for rigorous medical education survey-based studies. Its goals include fostering collaboration, offering mentorship in survey methodologies, and supporting initiatives to enhance equity, diversity, and antiracism.5,6 The 2025 GM Survey addressed topics of importance to CAFM members and current issues in family medicine education.
Although some demographics differed significantly between potential and actual survey respondents, the number of no responses for each category limits our calculations. A large proportion of missing demographic data comes from the inclusion of potential participants from the AFMRD databases that does not contain demographic details, only contact information. The missing data limits our ability to conclude that this survey sample is representative of the full general membership and may influence generalizability of survey results. Authors using CERA data can still use demographic data to perform subgroup analyses and interpret accordingly.
A key strength of the CERA survey is its consistent and organized framework, enabling members to conduct survey-based research aimed at national audiences in both the United States and Canada. A distinctive feature of the GM survey is that it allows members to focus on subgroups of family medicine professionals at different levels.7,8 By addressing essential topics in family medicine education, CERA supports stakeholders in developing data-driven educational policies.
Acknowledgments
The authors acknowledge the CERA Steering Committee for their help developing the manuscript version of this article.
Financial Support: CERA is supported by the academic family medicine organizations (STFM, ADFM, NAPCRG, and AFMRD).
Dr Miranda Moore reports receiving funding from National Institutes of Health, Agency for Healthcare Research and Quality's, Health Resources and Services Administration, and Georgia State Department of Human Services.
Conflict Disclosure: The authors have no conflicts of interest to declare.
References
- Shokar N, Bergus G, Bazemore A, et al. Calling all scholars to the council of academic family medicine educational research alliance (CERA). Ann Fam Med. 2011;9(4):372-373. doi:10.1370/afm.1283
- Maxwell L, Mazzone M, Abercrombie S, et al. CERA: what? So what? Now what? Ann Fam Med. 2012;10(6):576-577. doi:10.1370/afm.1455
- Seehusen DA, Mainous AG III, Chessman AW. Creating a centralized infrastructure to facilitate medical education research. Ann Fam Med. 2018;16(3):257-260. doi:10.1370/afm.2228
- Tanner C. CERA: advancing family medicine education research. Ann Fam Med. 2024;22(2):177-177. doi:10.1370/afm.3113
- Society of Teachers of Family Medicine. Significant events in STFM history. Accessed December 17, 2024. https://www.stfm.org/about/about/history/
- CAFM Educational Research Alliance. Accessed December 17, 2024. https://www.stfm.org/Research/CERA
- Ho T, Marzolf BA, Curtin AD, Biggs R. Protocol for the 2023 CERA general membership survey. Primer Peer-Rev Rep Med Educ Res. 8:26. doi:10.22454/PRiMER.2024.609918
- Mainous AG III, Rahmanian KP, Ledford CJW, Carek PJ. Professional identity, job satisfaction, and commitment of nonphysician faculty in academic family medicine. Fam Med. 2018;50(10):739-745. doi:10.22454/FamMed.2018.273724



There are no comments for this article.