Background and Objectives: Dermatologic issues represent up to 12.4% of encounters in family medicine practices. Despite the high number of skin conditions seen, current curricular guidelines for dermatologic experiences in family medicine residencies are vague and provide limited structure. We used a two-round modified Delphi process to reach expert consensus on dermatology learning objectives for family medicine residencies.
Methods: Objectives were compiled from three sources: Accreditation Council for Graduate Medical Education Family Medicine Program Requirements, the American Academy of Family Physicians Conditions of the Skin curriculum, and the American Academy of Dermatology 4 week Basic Dermatology modules. We invited 20 experts (nine dermatologists, 11 family physicians) to rate objectives using a 5-point Likert-type scale. Consensus was defined as≥75% of panelists agreeing or strongly agreeing that an objective should be included as a learning objective with<1.0 standard deviation. Prioritization, using a content validity index, was defined as≥80% of respondents rating an item as strongly agree.
Results: Overall, 194 unique objectives were considered, of which 189 (97.4%) met consensus. Three topics were ranked as the highest priority: actinic keratosis and squamous cell carcinoma, basal cell carcinoma, and atopic dermatitis. The lowest prioritized topics were dermoscopy and basic science. Only one procedure, injection of local anesthesia, met the prioritization threshold.
Conclusions: The highest-ranked topics highlight key areas that should be emphasized in a typical 2 week family medicine–dermatology rotation. Our findings can inform the development of a dermatology block, ensuring that limited residency time is directed toward the most essential objectives.
Currently, up to 12.4% of all encounters in family medicine practices present with common skin disorders that are fully managed by primary care physicians.1-4 A need for primary care physicians’ management of skin disorders is particularly pressing in rural areas, where dermatologist density is 0.085 dermatologists per 100,000 people, compared to 4.11 in metropolitan areas.5-7 However, nationwide studies have found that many primary care residents report only 1 to 4 hours of dermatology or dermoscopy training time.8-10 Medical school dermatology training is similarly limited, with a median of only 10 hours of instruction.11 This lack of training time was reflected in diagnostic accuracy, with a study finding that dermatologists had a 76.9% diagnostic accuracy rate while primary care physicians had a 37.5% accuracy rate for clinical examination of melanoma and keratinocytic cancers.12
Current curricular resources are inadequate for guiding dermatology education in family medicine residency programs. The Accreditation Council for Graduate Medical Education (ACGME) Program Requirements for Graduate Medical Education in Family Medicine has only one core requirement that mentions dermatology, stated as “Residents must have experience evaluating dermatologic presentations and managing common dermatologic conditions.”13 This statement does not specify the scope or time requirements of dermatology practice in family medicine. On the other hand, the American Academy of Dermatology (AAD) offers a 4 week online, module-based curriculum that is too comprehensive for family medicine–specific practice.14 The modules include specialized topics such as surgical closure techniques, rare drug reactions, and inpatient dermatology.
The Delphi method is a widely used approach in medical education to achieve expert consensus on curriculum development in specialty training.10,15-17 We developed a consensus-driven list of dermatology objectives for family medicine residencies using the Delphi method.
This study was performed under an approved protocol by a medical ethical review committee (IRB 25–44069). Informed consent was obtained. The study used a two-round modified Delphi method with Qualtrics (Qualtrics LLC).
We compiled initial learning objectives from three established sources: the ACGME Program Requirements for Graduate Medical Education in Family Medicine; the American Academy of Family Physicians Conditions of the Skin: Recommended Curriculum Guidelines for Family Medicine Residents; and the AAD Basic Dermatology curriculum (4 week rotation) modules.13,14,18
We emailed a screening survey to family medicine and dermatology residency program directors, associate program directors, and educational leaders across the country, as well as to members of the Association of Professors of Dermatology. Selection criteria included educational leadership roles, clinical leadership roles, and clinical practice expertise.
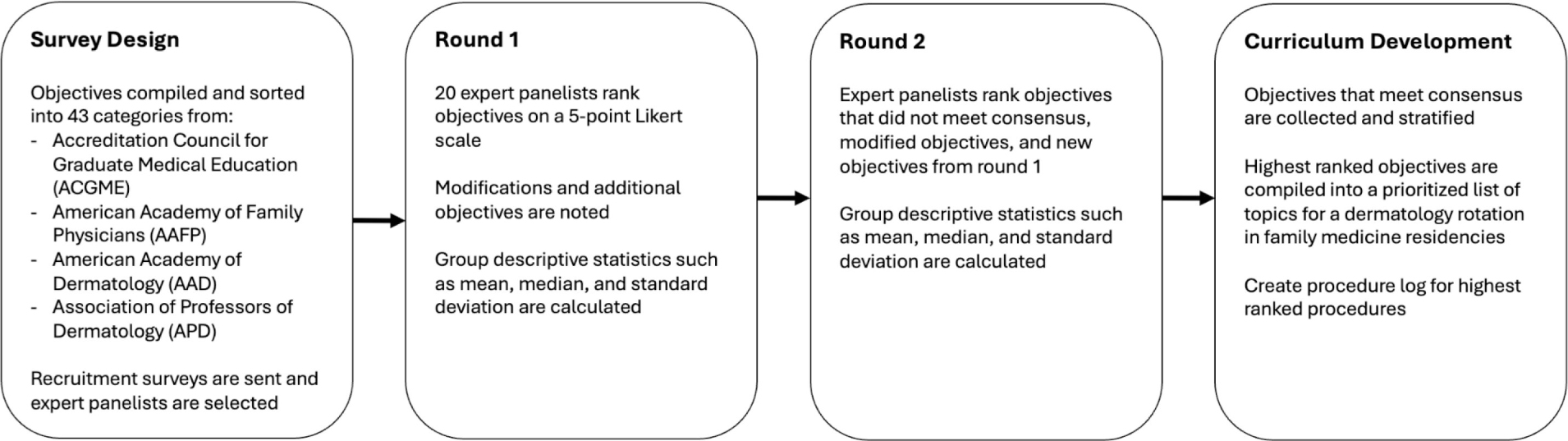
The two-round Delphi process used in this study is outlined in Figure 1. Each objective was rated using a 5-point Likert-type scale (1=strongly disagree to 5=strongly agree) to assess its importance for inclusion. Consensus was defined as ≥75% of respondents rating an item as “agree” or “strongly agree” with a standard deviation <1.0, ensuring that ratings reflected broad agreement across both specialties.19,20 We also invited panelists to suggest modifications and propose new objectives.
We undertook a secondary prioritization step in which we ranked objectives using a content validity index (CVI), validated in the RAND/UCLA appropriateness method.21,22 Prioritization with CVI was defined as≥80% of respondents rating an item as “strongly agree.” Higher score values indicate stronger expert agreement.23
After the initial round, we used descriptive statistics to summarize each objective’s distribution of ratings, mean, median, and standard deviation. The second survey round included items that did not meet consensus, defined as fewer than 75% of respondents rating “agree/strongly agree” for inclusion or “disagree/strongly disagree” for exclusion, modified objectives, additional objectives proposed, and round one group statistics such as median and mean.
After completion of the Delphi rounds, we invited panelists to participate in an optional post hoc survey. We asked each panelist to choose 10 highest-priority topics among 43, assigning ranks from 1 to 10. We analyzed rankings descriptively.
We invited 20 panelists to complete round one. Nineteen (95%) completed round one, and 18 of those 19 (95%) completed round two. Among the panelists were 11 (58%) family physicians and eight (42%) dermatologists. Sixteen (84%) practiced in urban and three (16%) in suburban settings. Seven (37%) held formal educational leadership positions, 11 (74%) were core teaching faculty members, and 15 (58%) held active clinical practice roles. Fifteen (79%) practiced in the West, three (16%) in the Midwest, one (5%) in the East, and one (5%) in the South.
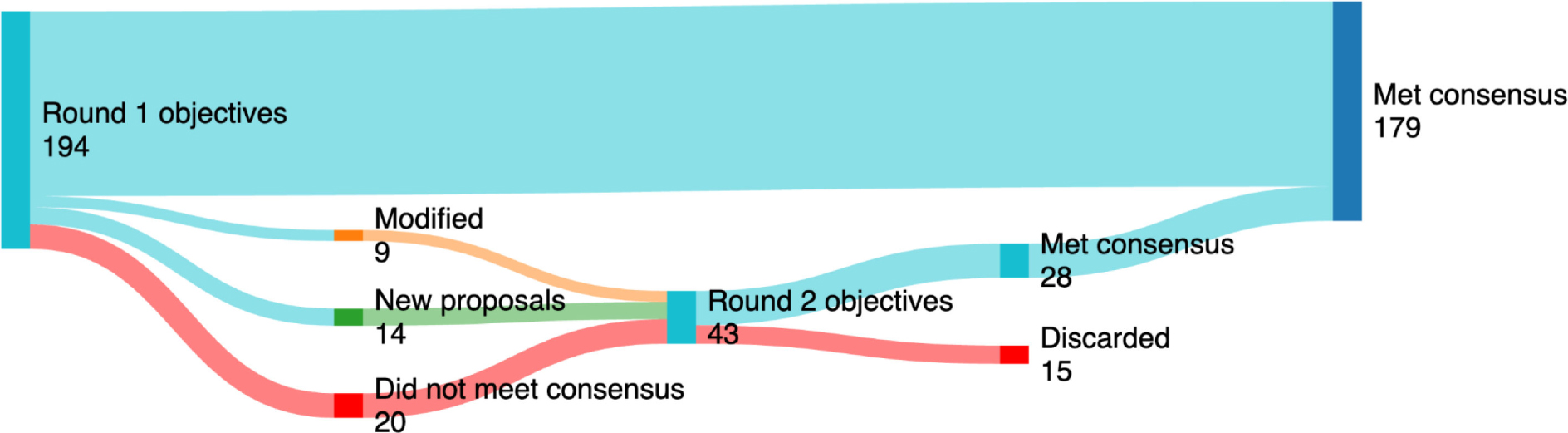
We consolidated objectives from the three original sources, removed duplicates, and grouped them into 43 topics, resulting in an initial list of 180 objectives. After the conclusion of the two rounds, a total of 179 of 194 unique objectives were retained for inclusion (Figure 2).
All objectives met the threshold for prioritization in three categories: actinic keratosis and squamous cell carcinoma, basal cell carcinoma, and atopic dermatitis. Other topics and their percentage of the objectives meeting prioritization threshold are displayed in Table 1. Thirteen panelists completed the post hoc survey. Nine or more panelists ranked the following topics in their top 10: actinic keratosis and squamous cell carcinoma, and atopic dermatitis.
Topics with all objectives meeting the threshold for prioritization |
|
Topics with>60% objectives meeting the threshold for prioritization |
Acne and rosacea Pediatric cutaneous fungal infections Melanoma Bacterial skin infections Stasis dermatitis and leg ulcers The red leg Contact dermatitis Urticaria |
Procedures meeting prioritization threshold |
|
Topics with <50% objectives meeting consensus |
|
Procedures not meeting consensus |
Excisional biopsy Electrodesiccation Curettage Nail avulsion |
Detailed objective results by topic, the number meeting consensus and prioritization, and objectives meeting or not meeting consensus by topic are shown in (Supplemental Tables 1–3), respectively.
Examination of comments made on low-prioritization categories suggested that panelists felt that these topics were out of scope or should not be prioritized. Participants wrote “With limited time in residency, I would focus more on clinical skills and hope/assume that residents remember the basic science taught in medical school” and “I would be concerned about relying on [dermoscopy] and missing the more relevant clinical findings and patient’s history.”
This study fills a gap in the dermatology curriculum for family medicine residency programs. ACGME does not specify measurable requirements or learning objectives.13 As a result, dermatology education in family medicine programs has been highly variable and often insufficient in clinical practice.1,24,25 To our knowledge, our study is the first to define consensus-driven dermatology learning objectives tailored to family medicine residents.
Using the Delphi process, we identified the three most prioritized topics and eight additional important topics. This finding is important because dermatology rotations are often brief, 2 weeks or less, and residents cannot feasibly master 43 topics during that time.9,10 The objective “injection of local anesthesia” met the prioritization threshold; however, more advanced procedures did not.
Future directions involve using the consensus-based objectives and 11 prioritized topics to develop a standardized 2 week dermatology curriculum and a basic dermatologic procedure case log for family medicine residency programs. Future research should focus on piloting this curriculum and evaluating its effect on diagnostic accuracy and referral patterns.
Despite high consensus levels and similar representation of family medicine and dermatologists, limitations should be acknowledged. First, the expert panel was composed primarily of practitioners in urban academic settings in the West. These results may not fully capture the practice realities of family physicians in rural areas or other geographic regions. Second, although our sample size was consistent with Delphi guidelines, the relatively small number of participants limits the ability to statistically analyze differences between specialties or practice environments.
In summary, this Delphi study provides a consensus-driven foundation for developing a family medicine–specific dermatology curriculum. The prioritized list of objectives highlights essential topics that can feasibly be covered within the time constraints of residency training. Implementation of this focused curriculum has the potential to enhance dermatologic care access, especially in communities where access to specialist care remains limited.
We would like to thank Mary Turocy, Sen Nguyen, Erin Mathes, Sharon Albers, Kareen Espino, Rachelene Tarsney, Jim Elam, Jenny Nguyen, Edward Kobayashi, Herbert Castillo Valladares, Julie Ramseier, Michael Waul, Iris Ahronowitz, Sarah Coates, Mukund Premkumar, Jay Sparks, David English, Kirsten Day, and Elizabeth Bailey for their participation and help in composing the draft objectives.
References
-
Verhoeven EWM, Kraaimaat FW, van Weel C, et al. Skin diseases in family medicine: prevalence and health care use.
Ann Fam Med. 2008;6(4):349–354. doi:10.1370/afm.861
-
Kerr OA, Tidman MJ, Walker JJ, Aldridge RD, Benton EC. The profile of dermatological problems in primary care.
Clin Exp Dermatol. 2010;35(4):380–383. doi:10.1111/j.1365-2230.2009.03586.x
-
-
-
Pearlman RL, Brodell RT, Byrd AC. Enhancing access to rural dermatological care: the time to start is now.
JAMA Dermatol. 2022;158(7):725–726. doi:10.1001/jamadermatol.2022.1470
-
Brumbaugh B, Lally J, Brodell R. Rural access to dermatology services: a call to action.
Dermatol Online J. 2024;30(5). doi:10.5070/D330564425
-
Feng H, Berk-Krauss J, Feng PW, Stein JA. Comparison of dermatologist density between urban and rural counties in the United States.
JAMA Dermatol. 2018;154(11):1265–1271. doi:10.1001/jamadermatol.2018.3022
-
Shadid AM, Albdaya NA, Aldosari MS, et al. Dermatology core curriculum in medical school and its association in the selection of dermatology as a future career: a nationwide cross-sectional study.
Journal of Dermatology and Dermatologic Surgery. 2023;27(2):58–62. doi:10.4103/jdds.jdds_19_23
-
Lu MD, Usatine R, Holt J, Harper DM, Verdieck A. Dermoscopy training in family medicine residencies: a CERA survey of program directors.
Fam Med. 2023;55(4):259–262. doi:10.22454/FamMed.2023.368813
-
Shellenberger RA, Fayyaz F. Dermatology education and clinical experience in a community hospital internal medicine residency program.
Advances in Clinical Medical Research and Healthcare Delivery. 2021;1(3). doi:10.53785/2769-2779.1037
-
-
-
-
-
Reed C, Kundu R. 52116 Assessment of an evidence-based dermatology curriculum for primary care medical education.
Journal of the American Academy of Dermatology. 2024;91(3):AB132. doi:10.1016/j.jaad.2024.07.532
-
Sanchez R, Sloan SR, Josephson CD, Ambruso DR, Hillyer CD, O’Sullivan P. Consensus recommendations of pediatric transfusion medicine objectives for clinical pathology residency training programs.
Transfusion. 2010;50(5):1071–1078. doi:10.1111/j.1537-2995.2009.02549.x
-
Curran ML, Martin EE, Thomas EC, et al. The pediatric rheumatology objective structured clinical examination: progressing from a homegrown effort toward a reliable and valid national formative assessment.
Pediatr Rheumatol Online J. 2019;17(1):5. doi:10.1186/s12969-019-0308-7
-
-
Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies.
J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
-
Franc JM, Hung KKC, Pirisi A, Weinstein ES. Analysis of Delphi study 7-point linear scale data by parametric methods: Use of the mean and standard deviation.
Methodological Innovations. 2023;16(2):226–233. doi:10.1177/20597991231179393
-
Fitch K, Bernstein SJ, Aguilar MD, et al. The Rand/UCLA Appropriateness Method User’s Manual. Rand; 2001.
-
-
Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity.
Res Social Adm Pharm. 2019;15(2):214–221. doi:10.1016/j.sapharm.2018.03.066
-
-
Howard J, Siegel LH, Mok K, Sibbald S. Family medicine residents’ perspectives in dermatology training.
MedEdPublish (2016). 2021;10:90. .
doi:10.15694/mep.2021.000090.1



There are no comments for this article.