Background and Objectives: Artificial intelligence (AI) offers significant potential to support various aspects of general practitioners’ (GPs’) work but raises important ethical questions. This study explored and compared AI use and the related attitudes, ethical concerns, and training needs of GP residents and supervisors.
Methods: We conducted a cross-sectional, self-administered online survey among second-and third-year GP residents and supervisors in Toulouse (France). The survey examined AI use, attitudes, ethical considerations, and training needs. We compared groups using bivariate analysis to explore potential generational differences (P<0.05).
Results: A total of 175 GP residents and 402 supervisors responded. Overall, 21% of respondents reported using AI in medical practice. Residents expressed greater familiarity with AI and less need for control and transparency than supervisors. Top ethical concerns included plagiarism, cognitive off-loading, and reasoning limitations. Training was desired by 91% of supervisors and 71% of residents.
Conclusions: Our results highlight generational differences in technology acceptance and a strong demand for AI training. Study limitations included risk of data obsolescence, nonresponse, selection bias, and a monocentric sample. These findings underscore the need to develop targeted AI training programs and implement formal safeguards to regulate AI use in academic settings.
Artificial intelligence (AI) and large language models are evolving rapidly, offering promising prospects in health care.1,2
AI appears to be highly relevant for general practitioners (GPs), with potential targeted uses including documentation, triaging results, managing patient messages,3 and diagnosis.4,5 Ambient AI documentation tools provide a concrete example of clinically relevant AI use, with studies reporting reduced time-in-note and potential improvements in burnout, task load, and work exhaustion6 alongside reductions in administrative burden and enhanced patient–clinician interaction.7 Additionally, AI could assist in mitigating cognitive biases4 and offer support in managing clinical uncertainty8 and transcribing medical reports.9 Finally, AI may support patient-centered care by enhancing patient health literacy, self-management of chronic conditions,10 and autonomy.11
Ethically, questions remain regarding algorithm transparency, because the reasoning behind large language model responses is often unclear,12 along with biases12,13 and accuracy issues.5,14
AI holds promise to enhance formative exercises, advance medical education, and support GPs’ continuing learning. In France, family medicine training follows a national pathway combining 6 years of undergraduate medical education with a 3 year residency (to be extended to 4 years for students who started residency in 2023, with the first fourth year implemented in the 2026–2027 academic year); the training is organized into 6 month clinical rotations and around 200 hours of coursework. Assessment is mainly formative and based on structured written work compiled in an electronic portfolio. In Toulouse, residents regularly produce brief records focused on a single clinical question from a consultation, alongside longer narrative reports on complex cases integrating biomedical, psychosocial, ethical, or organizational issues. These reports include the residents’ own reflections and the results of a narrative review, and are discussed with a family physician supervisor.15
AI therefore introduces new opportunities but also raises ethical concerns that present significant educational challenges. While medical students generally have a positive attitude toward AI,16,17 the lack of structured training remains a major issue.18,19 Ethically, concerns about students’ use of AI include risks to academic integrity,20 its impact on critical thinking,21 and cognitive off-loading.22
To our knowledge, no study has examined the use, attitudes, ethical concerns, and training needs regarding AI among general practice residents and their supervising physician. We hypothesized that generational differences may exist in this domain.
The study’s primary aim was to characterize the use of, attitude toward, and ethical concerns about AI and related training needs of GP residents and their supervising physicians. The secondary aim was to compare these factors between our two populations.
This was a cross-sectional observational study conducted using a self-administered questionnaire. This study followed the STROBE23 and CRISP24 recommendations.
The questionnaire was developed on LimeSurvey (LimeSurvey GmbH) by members of the University Department of General Medicine in Toulouse. The regulatory authorizations from the CNIL (France’s data protection authority) were requested and approved by the university’s data protection officer (September 2, 2024, for residents; October 2, 2024, for supervisors).
Variables included sociodemographic data (gender, years of practice for supervisors, year of internship for interns), use of AI in medical, academic, and personal practice, as well as perceptions of its usefulness, impact (time-saving, quality, relevance), and ethical issues. We assessed the reliability and relevance of AI in supporting residents’ written academic work using 5-point Likert scales (1 = not at all reliable/relevant; 5 = extremely reliable/relevant). Participants also expressed their opinions on AI training and rules to be developed to regulate AI’s use.
The questionnaire was administered to general medicine residents in Toulouse at the end of their first and second internship years; it was distributed through a QR code during welcome meetings in September 2024 and November 2024. It also was administrated to university supervisors during pedagogical meetings over three sessions in October 2024. The response rate was estimated using, for residents, the official list of enrolled students for the relevant academic year and, for supervisors, attendance lists from these pedagogical meetings.
To avoid selection bias, we surveyed all residents and supervisors meeting the inclusion criteria. Residents who had not yet started their internship were excluded because they had not yet had to produce written records. Residents nearing the end of their internship were excluded because they were no longer concerned with the development of regulatory rules.
Given the very low proportion of missing values, missing data were excluded from statistical analyses.
We compared AI use, attitudes, and ethical considerations by resident or supervisor status to explore generational differences using χ2 tests. Tests with P<0.05 were considered statistically significant.
A total of 175 GP residents and 402 supervisors responded, corresponding to response rates of 58.7% among residents (175/298) and 77.0% among supervisors attending the pedagogical meetings (402/522). Missing data accounted for less than 5% of responses for each variable and were excluded from the analyses. Demographic characteristics are presented in Table 1, with 62% being female (n = 334). A total of 33% (n = 181) reported familiarity with AI applications in clinical practice, 19% (n = 102) in academic settings, and 52% (n = 286) in personal use, with residents showing higher awareness (P<0.001). A total of 21% (n = 114) used AI in medical practice and 8% (n = 44) for complex therapeutic decisions.
Characteristic |
N |
Residents
N = 175
n (%) |
Supervisors
N = 402
n (%) |
P valuea |
Respondent profile |
Gender |
538 |
|
|
|
Female |
|
112 (68) |
222 (59) |
|
Male |
|
52 (32) |
152 (41) |
|
Not applicable |
|
11 |
28 |
|
Practice area type |
393 |
|
|
|
Rural |
|
– |
86 (22) |
|
Semirural |
|
– |
187 (48) |
|
Urban |
|
– |
120 (31) |
|
Not applicable |
|
– |
9 |
|
Years of medical experience |
393 |
|
|
|
<5 years |
|
– |
40 (10) |
|
Five to 14 years |
|
– |
187 (48) |
|
15 to 30 years |
|
– |
120 (31) |
|
More than 30 years |
|
– |
46 (12) |
|
Not applicable |
|
– |
9 |
|
Involved in thesis supervision |
384 |
|
|
|
No |
|
– |
316 (82) |
|
Yes |
|
– |
49 (13) |
|
Not yet, but interested |
|
– |
19 (4.9) |
|
Not applicable |
|
- |
18 |
|
Current internship semester |
169 |
|
|
|
2nd semester |
|
94 (56) |
– |
|
4th semester |
|
52 (31) |
– |
|
Other semester |
|
23 (14) |
– |
|
Not applicable |
|
6 |
402 |
|
AI use |
Familiar with AI in clinical practice |
551 |
|
|
<0.001 |
Uncertain |
|
29 (17) |
52 (14) |
|
No |
|
62 (37) |
227 (59) |
|
Yes |
|
75 (45) |
106 (28) |
|
Not applicable |
|
9 |
17 |
|
Familiar with AI in academic settings |
545 |
|
|
<0.001 |
Uncertain |
|
26 (16) |
41 (11) |
|
No |
|
71 (43) |
305 (81) |
|
Yes |
|
70 (42) |
32 (8.5) |
|
Not applicable |
|
8 |
24 |
|
Familiar with AI for personal use |
551 |
|
|
<0.001 |
Uncertain |
|
13 (7.8) |
35 (9.1) |
|
No |
|
41 (25) |
176 (46) |
|
Yes |
|
112 (67) |
174 (45) |
|
Not applicable |
|
9 |
17 |
|
Number of AI platforms known |
498 |
|
|
<0.001 |
0 |
|
10 (6.1) |
76 (23) |
|
1 |
|
104 (64) |
167 (50) |
|
2 |
|
30 (18) |
51 (15) |
|
Three or more |
|
19 (12) |
41 (12) |
|
Not applicable |
|
12 |
67 |
|
Already used AI in medical practice |
547 |
|
|
.3 |
No |
|
126 (76) |
307 (80) |
|
Yes |
|
39 (24) |
75 (20) |
|
Not applicable |
|
10 |
20 |
|
Domains where AI could be useful (yes) |
|
|
|
|
Filling the patient’s medical record |
577 |
97 (55) |
207 (51) |
.4 |
Patient follow-up |
577 |
49 (28) |
137 (34) |
.2 |
Diagnostic assistance |
577 |
82 (47) |
201 (50) |
.5 |
Decision support when uncertain |
577 |
67 (38) |
165 (41) |
.5 |
Managing care: ordering tests and treatments |
577 |
72 (41) |
172 (43) |
.7 |
Explaining information to patients |
577 |
52 (30) |
99 (25) |
.2 |
Already used AI for therapeutic decisions in a complex therapeutic case (yes) |
527 |
18 (11) |
26 (7.1) |
.13 |
Not applicable |
|
13 |
37 |
|
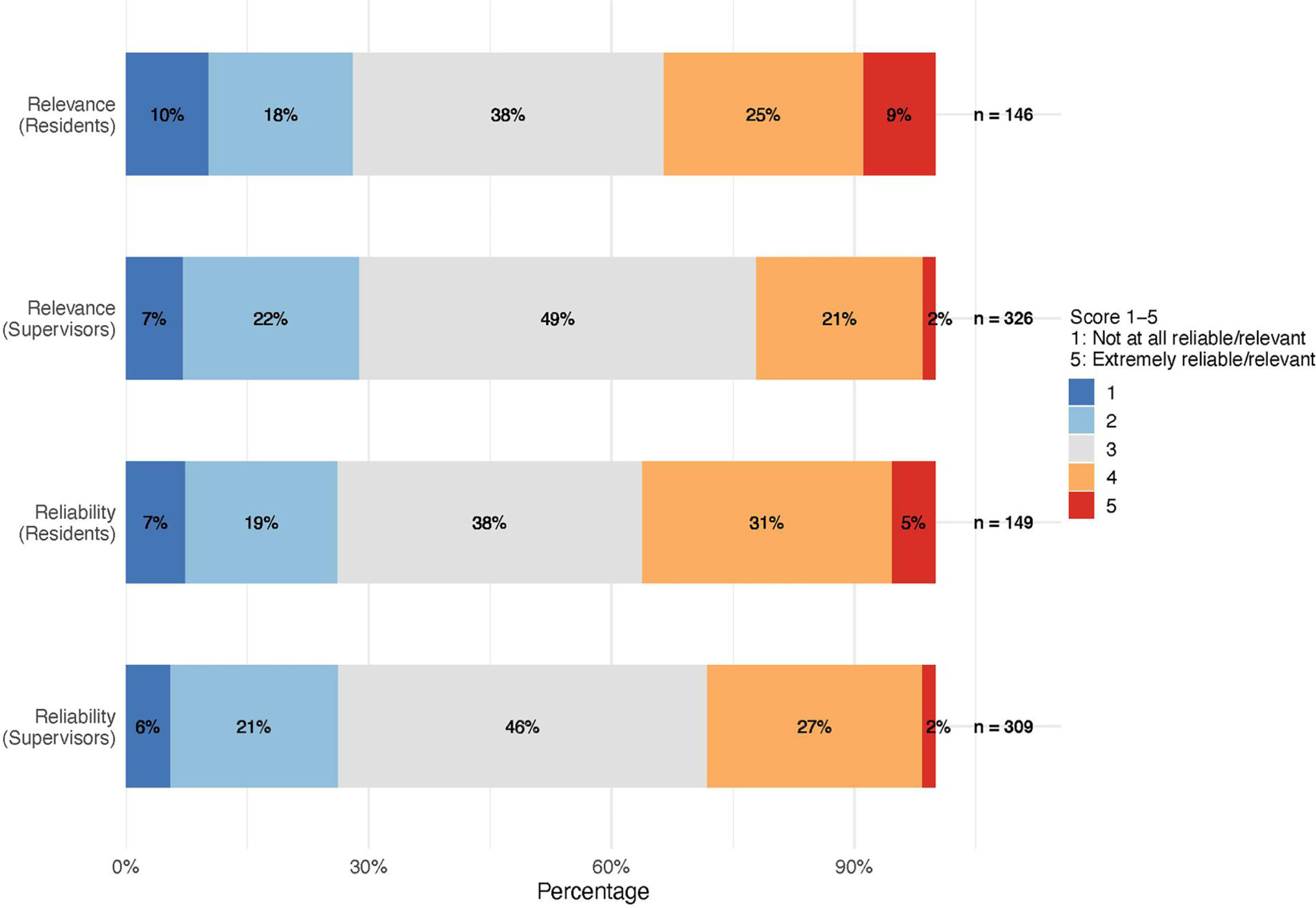
Table 2 outlines attitudes, ethical concerns, and training needs regarding AI. For written clinical tasks, 78% (n = 374) perceived quality improvement, 91% (n = 456) time-savings, and 49% (n = 227) enhanced relevance. Ethical concerns regarding the use of AI in academic writing were reported by 83% (n = 406) of respondents, more among supervisors than residents (72% residents vs 87% supervisors, p<0.001). The most frequent ethical concerns were the risk of plagiarism, cognitive off-loading, and reasoning limitations, with higher rates among supervisors (79% vs 89%, P<0.001; 75% vs 81%, P = 0.004; 83% vs 89%, P = 0.002). Regarding regulation, 70% (n = 402) of respondents favored regulated authorization; residents were statistically more inclined toward uncontrolled use (14% vs 5.2%, P<0.001), whereas supervisors preferred AI detection (15% vs 33%, P<0.001) and declaration of AI use (39% vs 69%, P<0.001). Training was desired by 91% (n = 326) of supervisors and 71% (n = 113) of residents. AI relevance in supporting residents’ clinical and research writing tasks were rated high (4 to 5 on a scale of 5) by 26% (n = 121) of participants, while 31% (n = 141) rated its reliability as high; further details on these data are illustrated in Figure 1.
Characteristic |
N |
Residents
N = 175
n (%) |
Supervisors
N = 402
n (%) |
P valuea |
Perceived impact of AI on written clinical tasks |
Improves quality of written clinical tasks |
482 |
108 (68) |
266 (83) |
<0.001 |
Not applicable |
|
15 |
80 |
|
Improves relevance on written clinical tasks |
468 |
70 (45) |
157 (50) |
.2 |
Not applicable |
|
18 |
91 |
|
Saves time on written clinical task |
503 |
145 (87) |
311 (93) |
.037 |
Not applicable |
|
8 |
66 |
|
Ethical concerns |
Perceived ethical concerns with AI for written academic work |
492 |
110 (72) |
296 (87) |
<0.001 |
Not applicable |
|
22 |
63 |
|
Type of ethical concerns with AI for written academic work |
|
|
|
|
Risk of information bias |
406 |
75 (68) |
181 (61) |
.6 |
Risk of plagiarism |
406 |
87 (79) |
264 (89) |
<0.001 |
Cognitive off-loading |
406 |
82 (75) |
240 (81) |
.004 |
Reasoning limitation |
406 |
91 (83) |
264 (89) |
.002 |
Risk of dependency |
406 |
72 (65) |
210 (71) |
.014 |
Confidentiality concerns |
406 |
65 (59) |
124 (42) |
.14 |
Impact on research value |
406 |
58 (53) |
148 (50) |
.4 |
Equity of access |
406 |
42 (38) |
131 (44) |
.039 |
Not displayed |
|
65 |
106 |
|
AI regulation preferences |
Complete ban |
577 |
7 (4.0) |
17 (4.2) |
.9 |
Regulated authorization |
577 |
121 (69) |
281 (70) |
.9 |
Free use |
577 |
25 (14) |
21 (5.2) |
<0.001 |
Detection software control |
577 |
27 (15) |
133 (33) |
<0.001 |
Declaration of use |
577 |
68 (39) |
273 (68) |
<0.001 |
Training needs |
Training during internship |
523 |
113 (71) |
330 (91) |
<0.001 |
Not applicable |
|
16 |
38 |
|
Training for supervisors |
359 |
– |
326 (91) |
|
Not applicable |
|
175 |
43 |
|
This study provided early insights into perceptions and emerging use of AI in French general practice. While most respondents recognized AI’s potential in clinical and academic contexts, AI’s widespread adoption remains limited. Notably, residents showed greater familiarity with AI and less demand for control and transparency than supervising physicians, highlighting important generational differences in technology acceptance. A strong desire for targeted AI training also emerged.
Our findings align with international trends showing cautious optimism toward AI in primary care.25,26 Generational differences in digital health technology use have been described among patients27 but, to our knowledge, no prior data allow comparison with residents’ and supervisors’ use of AI. The need to adapt medical education to the realities of the AI era is widely acknowledged, with several authors emphasizing the importance of comprehensive curricular reform to equip future physicians with the necessary skills and ethical frameworks for responsible AI use.28,29
Environmental considerations, such as AI’s energy consumption and carbon footprint, were not addressed but are increasingly relevant for sustainable health care.30
Strengths of our study included a large sample and early data capture, establishing a baseline for AI uptake in primary care. Limitations included potential data obsolescence, item nonresponse, selection bias from voluntary supervisor participation, and a limited sample size due to monocentric recruitment from a single department of general practice in France. Although the proportion of missing data was low (below 5% for each variable), this remains a potential source of bias and may have slightly influenced our estimates.
In response to identified needs, our department has implemented targeted AI training and formal safeguards regulating academic use. Evaluation is still required to determine which teaching formats and points in the curriculum are most effective. Strengthening transparency around AI is essential, and specific strategies are needed to help students appreciate its value. Supervisors also may need to define which clinical competencies should deliberately remain free of AI support in order to safeguard core professional skills. Given rapid technological evolution and emerging ethical issues, periodic reassessment of attitudes and practices seems essential to ensure safe, effective, and patient-centered integration of AI in family medicine. While AI might risk diminishing human connection, integrating AI education could enhance future doctor-patient interactions.11 Future research should explore this critical dimension.
Our results suggest that, although most respondents recognize the potential of AI in clinical and academic settings, its adoption remains limited. We identified generational differences, with residents more familiar with AI and supervisors seeking more control and transparency. Both groups expressed strong demand for AI training. These findings underscore the need to develop targeted AI training programs and implement formal safeguards to regulate AI use in academic settings.
The authors thank Kevanne Monkhouse for English language editing and assistance with translating the manuscript. The authors also thank Aurore Palmaro for valuable advice on methodological aspects of the study.
References
-
Lee P, Bubeck S, Petro J. Benefits, limits, and risks of GPT-4 as an AI chatbot for medicine.
N Engl J Med. 2023;388(13):1233–1239. doi:10.1056/NEJMsr2214184
-
Haug CJ, Drazen JM. Artificial intelligence and machine learning in clinical medicine.
N Engl J Med. 2023;388(13):1201–1208. doi:10.1056/NEJMra2302038
-
Menchaca JT. For AI in primary care, start with the problem.
Ann Fam Med. 2025;23(1):5–6. doi:10.1370/afm.240504
-
Summerton N, Cansdale M. Artificial intelligence and diagnosis in general practice.
Br J Gen Pract. 2019;69(684):324–325. doi:10.3399/bjgp19X704165
-
Ríos-Hoyo A, Shan NL, Li A, Pearson AT, Pusztai L, Howard FM. Evaluation of large language models as a diagnostic aid for complex medical cases.
Front Med (Lausanne). 2024;11:1380148. doi:10.3389/fmed.2024.1380148
-
Lukac PJ, Turner W, Vangala S, et al. Ambient AI scribes in clinical practice: a randomized trial.
NEJM AI. 2025;2(12). doi:10.1056/aioa2501000
-
Alboksmaty A, Aldakhil R, Hayhoe BWJ, Ashrafian H, Darzi A, Neves AL. The impact of using AI-powered voice-to-text technology for clinical documentation on quality of care in primary care and outpatient settings: a systematic review.
EBioMedicine. 2025;118:105861. doi:10.1016/j.ebiom.2025.105861
-
Alli SR, Hossain SQ, Das S, Upshur R. The potential of artificial intelligence tools for reducing uncertainty in medicine and directions for medical education.
JMIR Med Educ. 2024;10:e51446. doi:10.2196/51446
-
Agarwal P, Lall R, Girdhari R. Artificial intelligence scribes in primary care.
CMAJ. 2024;196(30):E1042. doi:10.1503/cmaj.240363
-
Traylor DO, Kern KV, Anderson EE, Henderson R. Beyond the screen: the impact of generative artificial intelligence (AI) on patient learning and the patient-physician relationship.
Cureus. 2025;17(1):e76825. doi:10.7759/cureus.76825
-
Sauerbrei A, Kerasidou A, Lucivero F, Hallowell N. The impact of artificial intelligence on the person-centred, doctor-patient relationship: some problems and solutions.
BMC Med Inform Decis Mak. 2023;23(1):73. doi:10.1186/s12911-023-02162-y
-
Yu KH, Healey E, Leong TY, Kohane IS, Manrai AK. Medical artificial intelligence and human values.
N Engl J Med. 2024;390(20):1895–1904. doi:10.1056/NEJMra2214183
-
Sasseville M, Ouellet S, Rhéaume C, et al. Bias mitigation in primary health care artificial intelligence models: scoping review.
J Med Internet Res. 2025;27:e60269. doi:10.2196/60269
-
Williams CYK, Miao BY, Kornblith AE, Butte AJ. Evaluating the use of large language models to provide clinical recommendations in the emergency department.
Nat Commun. 2024;15(1):8236. doi:10.1038/s41467-024-52415-1
-
Escourrou E, Bergeaut M, Gimenez L, et al. Evolution of reactions to uncertainty among residents during a clinical rotation.
Fam Med. 2020;52(5):339–345. doi:10.22454/FamMed.2020.403807
-
Amiri H, Peiravi S, Rezazadeh Shojaee SS, et al. Medical, dental, and nursing students’ attitudes and knowledge towards artificial intelligence: a systematic review and meta-analysis.
BMC Med Educ. 2024;24(1):412. doi:10.1186/s12909-024-05406-1
-
Laupichler MC, Aster A, Meyerheim M, Raupach T, Mergen M. Medical students’ AI literacy and attitudes towards AI: a cross-sectional two-center study using pre-validated assessment instruments.
BMC Med Educ. 2024;24(1):401. doi:10.1186/s12909-024-05400-7
-
Jebreen K, Radwan E, Kammoun-Rebai W, et al. Perceptions of undergraduate medical students on artificial intelligence in medicine: mixed-methods survey study from Palestine.
BMC Med Educ. 2024;24(1):507. doi:10.1186/s12909-024-05465-4
-
Jackson P, Ponath Sukumaran G, Babu C, et al. Artificial intelligence in medical education—perception among medical students.
BMC Med Educ. 2024;24(1):804. doi:10.1186/s12909-024-05760-0
-
Foltynek T, Bjelobaba S, Glendinning I, et al. ENAI recommendations on the ethical use of artificial intelligence in education.
Int J Educ Integr. 2023;19(1):1–4. doi:10.1007/s40979-023-00133-4
-
Lee HP, Sarkar A, Tankelevitch L, et al. The impact of generative AI on critical thinking: self-reported reductions in cognitive effort and confidence effects from a survey of knowledge workers.
Paper presented at: CHI Association for Computing Machinery; April 26, 2025; Yokohama, Japan. 10.1145/3706598.3713778
-
Gerlich M. AI tools in society: impacts on cognitive offloading and the future of critical thinking.
Societies. 2025;15(1):6. doi:10.3390/soc15010006
-
von Elm E, Altman DG, Egger M, et al, STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies.
Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
-
Phillips WR, Sturgiss E, Glasziou P, et al. Improving the reporting of primary care research: consensus reporting items for studies in primary care—the CRISP statement.
Ann Fam Med. 2023;21(6):549–555. doi:10.1370/afm.3029
-
Abdulazeem HM, Meckawy R, Schwarz S, Novillo-Ortiz D, Klug SJ. Knowledge, attitude, and practice of primary care physicians toward clinical AI-assisted digital health technologies: systematic review and meta-analysis.
Int J Med Inform. 2025;201:105945. doi:10.1016/j.ijmedinf.2025.105945
-
Allen MR, Webb S, Mandvi A, Frieden M, Tai-Seale M, Kallenberg G. Navigating the doctor-patient-AI relationship—a mixed-methods study of physician attitudes toward artificial intelligence in primary care.
BMC Prim Care. 2024;25(1):42. doi:10.1186/s12875-024-02282-y
-
Cecconi C, Adams R, Cardone A, et al. Generational differences in healthcare: the role of technology in the path forward.
Front Public Health. 2025;13:1546317. doi:10.3389/fpubh.2025.1546317
-
Jong M. Transforming medical education in the AI era: balancing technological expertise with humanistic care in tomorrow’s doctors.
Ann Acad Med Singap. 2024;53(12):754–757. doi:10.47102/annals-acadmedsg.2024242
-
Pregowska A, Perkins M. Artificial intelligence in medical education: technology and ethical risk.
SSRN Journal. 2023. doi:10.2139/ssrn.4643763
-
Gaetani M, Mazwi M, Balaci H, Greer R, Maratta C. Artificial intelligence in medicine and the pursuit of environmentally responsible science.
Lancet Digit Health. 2024;6(7):e438–e440. doi:10.1016/S2589-7500(24)00090-6



There are no comments for this article.