Background and Objectives: Family-oriented care is a core competency in family medicine, yet the educational processes through which residents develop this skill remain poorly understood. We examined how family physicians acquire family-oriented perspectives through clinical practice and reflective learning to inform curriculum development.
Methods: We conducted a qualitative descriptive study by purposively collecting residency evaluation portfolios from 15 physicians who were board-certified in family medicine in Japan between 2018 and 2023. Reflective narratives were analyzed by a five-member research team using Steps for Coding and Theorization (SCAT), referencing the “Action, Looking back on the action, Awareness of essential aspects, Creating alternative methods of action, and Trial” (ALACT) model and the Levels of Physician Involvement With Families framework.
Results: Residents’ reflections demonstrated progressive learning. They developed awareness of their emotions and communication, recognized circular perspectives, and viewed themselves as agents of change within family systems. They also linked family-oriented care with core principles of family medicine: continuity, comprehensiveness, and attention to social context. However, the depth of reflection varied. Practice descriptions emphasized empathic engagement, tailored advice, and information sharing or role negotiation, often through family conferences, whereas exploration of relational dynamics and emotional involvement was limited. Context-sensitive flexibility appeared crucial in shaping practice quality.
Conclusions: Family-oriented care acquisition involved knowledge, skills, and meaningful shifts in clinical attitudes and professional identity. Variation in reflective depth and relational insight suggests a need for structured reflective learning and targeted educational strategies to support family-oriented competencies.
Families play a central role in caregiving across diverse clinical contexts, including cancer, dementia, chronic illness, and end-of-life care, and the physical and mental health of family caregivers are internationally recognized as major concerns.1,2 Family-oriented care is widely recognized as a core perspective in family medicine, and competency frameworks emphasize attention to family relationships and social context as essential elements of training.3-5 However, educational programs remain insufficiently systematized, and concrete guidance for educators is limited.6
Previous studies have demonstrated several educational benefits of family-oriented care, including improved understanding of genograms and family systems theory,7 enhanced rapport-building and empathic communication,8 improved quality of care and positive effects on clinicians’ self-understanding and self-care.9 However, most prior research has focused on evaluating outcomes of educational interventions; the learning processes themselves—how residents develop a family-oriented perspective through clinical experiences and reflection—remain largely unclear.
Because family-oriented care involves complex relational dynamics and requires emotional engagement from clinicians, knowledge transmission alone is insufficient. Reflective practice is regarded as fundamental to professional growth,10,11 and several training frameworks now incorporate structured reflection through tools such as e-portfolios and supervision.3,4,12
In Japan, family medicine residents are required to document clinical cases and reflections across 20 competency domains, including family-oriented care, within their certification portfolios.13 These portfolios offer a unique opportunity to examine reflective learning processes, because they function both as a record of clinical practice and as an assessment tool for certification.14,15
This study aimed to qualitatively analyze these evaluation portfolios, completed during residency training, to clarify how family medicine residents learn and integrate family-oriented care into clinical practice. The findings may inform curriculum development and the refinement of competencies in this domain.
This qualitative descriptive study, grounded in a constructivist paradigm, examined reflective descriptions contained in evaluation portfolios completed during residency training by Japanese family physicians who were board-certified at the time of the study. The ALACT model (Action, Looking back on the action, Awareness of essential aspects, Creating alternative methods of action, and Trial) served as the guiding framework for analyzing reflective learning,16 while the Levels of Physician Involvement With Families framework was used to classify the degree of family involvement.17 In the ALACT model, Looking back on the action represents descriptive reconstruction of events, whereas Awareness reflects deeper interpretive insight into emotions, assumptions, and meanings. These distinctions informed our analytic approach.
The research team consisted of five members with expertise in family medicine, psychosomatic medicine, and qualitative research. Reflexive dialogue, bracketing, and multidisciplinary perspectives were incorporated to enhance analytic rigor. Bracketing was defined as the process of identifying and setting aside researchers’ preconceptions.
Participant and Recruitment
Through purposive sampling, we recruited physicians who underwent the Japanese Society of Primary Care’s family medicine specialist certification examination between 2018 and 2023.
All participants were board-certified family physicians at the time of the study, and the analyzed portfolios had been completed during their residency training. We distributed email invitations with study information and consent forms. After written consent was obtained, participants provided their portfolios in PDF format.
Data Collection
Portfolios from 15 physicians, completed during residency training, were anonymized and assigned identification codes. The correspondence table linking IDs to individuals was stored separately under password protection. Ethical approval was granted by the Nagoya University Clinical Research Review Committee (Approval No. 2023–0252).
Data Analysis
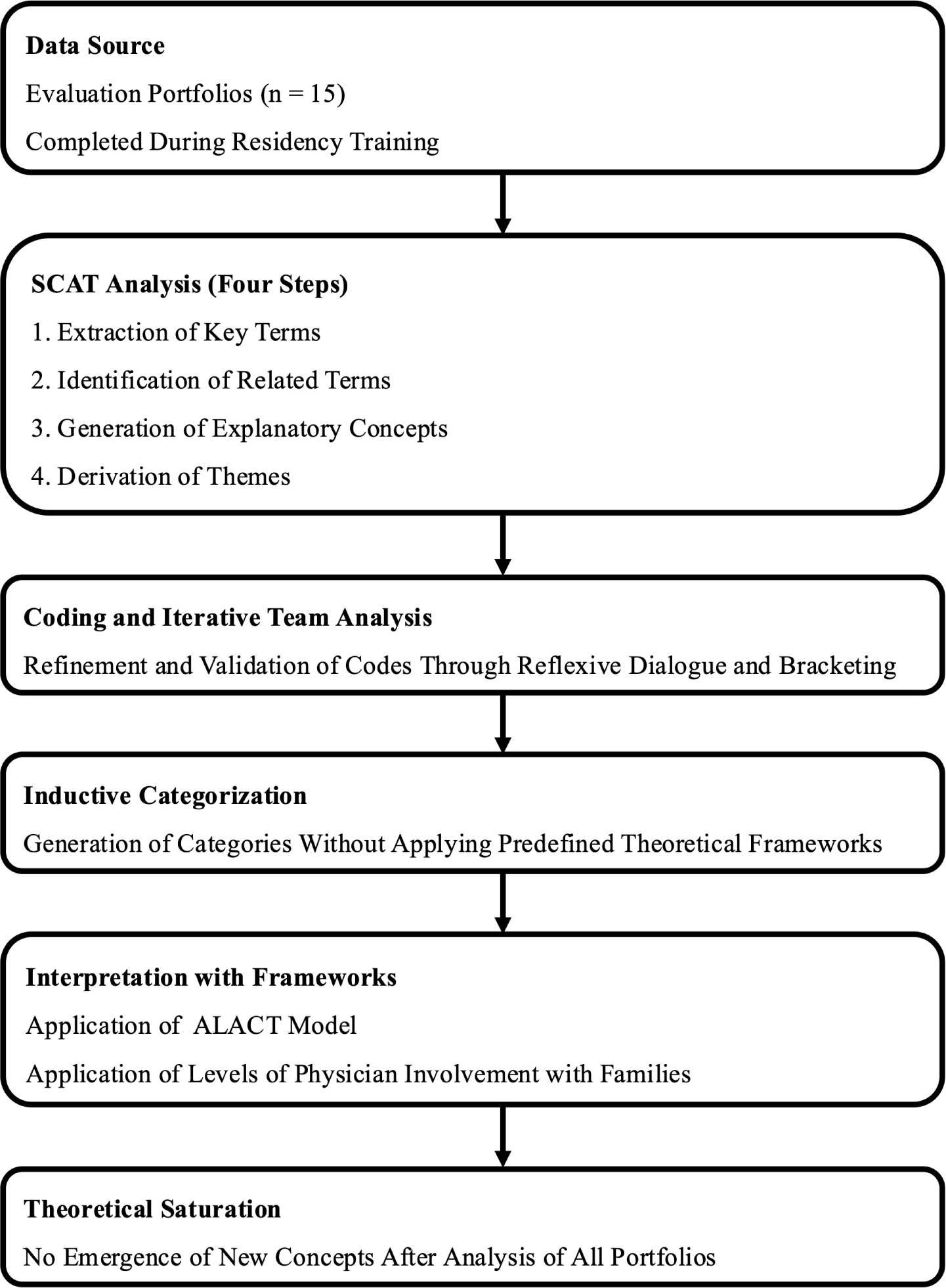
We analyzed data using Steps for Coding and Theorization (SCAT), a four-stage qualitative analysis method: (1) extraction of key terms, (2) identification of related terms, (3) generation of explanatory concepts, and (4) derivation of themes.18 The overall analysis process is shown in Figure 1. We used SCAT to identify and conceptualize thoughts, attitudes, and learning processes underlying family-oriented care.
The primary analyst generated initial codes, followed by iterative team discussions to refine coding and assess the validity and coherence of emerging interpretations. To minimize the influence of researchers’ preconceptions on the analytic process, all data were fully anonymized, and consensus was developed through reflexive team discussions and the deliberate use of bracketing.
After explanatory concepts were derived, they were inductively organized into categories without applying any theoretical framework during coding. When these categories were later reviewed, they were found to align naturally with the ALACT model and the Levels of Physician Involvement With Families framework. We used these frameworks, therefore, only to structure and deepen the interpretation of findings, rather than to constrain the inductive analytic process.
Multiple disciplinary perspectives within the research team were incorporated throughout the analytic process to enhance rigor and ensure multifaceted interpretation. Theoretical saturation was reached when no new concepts emerged after analysis of all 15 portfolios.
Table 1 summarizes the characteristics of the 15 evaluation portfolios. Tables 2 and 3 present descriptions mapped to each stage of the ALACT model and to the corresponding involvement levels from the Levels of Physician Involvement With Families framework. Because the portfolios described single clinical episodes without subsequent reintervention, the Trial stage was not analyzed. Level one involvement was excluded, because it was assumed to have been acquired during initial training. Level one was defined as minimal emphasis on family, with no explicit integration of family perspectives into care.
|
n (%) |
Characteristics of the portfolio authors (N = 15) |
Gender |
|
Female |
11 (73) |
Male |
4 (27) |
Others |
0 |
Residency years |
|
3 |
11 (73) |
4 |
4 (27) |
Characteristics of the clinical cases (N = 15) |
Age group (years) |
|
0–9 |
1 (7) |
10–19 |
1 (7) |
20–29 |
1 (7) |
50–59 |
1 (7) |
60–69 |
1 (7) |
70–79 |
3 (20) |
80–89 |
6 (40) |
90–99 |
1 (7) |
Family life cycle phase |
|
Emerging young adults |
1 (7) |
Families with young children |
1 (7) |
Families with adolescents |
1 (7) |
Launching children and moving on at midlife |
1 (7) |
Families in late middle age |
1 (7) |
Family nearing the end of life |
10 (67) |
Clinical scenario |
|
Outpatient |
6 (40) |
Inpatient |
6 (40) |
Home care |
2 (13) |
Residential facility |
1 (7) |
Family approach format |
|
Family interview in a routine office visit |
3 (20) |
Family conference |
12 (80) |
ALACT stage |
Portfolios showing the stage
n (%) |
Action |
15 (100) |
Looking back on the action |
15 (100) |
Awareness of essential aspects |
10 (67) |
Creating alternative methods of action |
10 (67) |
Behavioral domain |
n (%) |
Level 2. Ongoing medical information and advice |
Clear communication of medical information |
5 (33) |
Eliciting relevant clinical information |
0 |
Attentive listening to concerns |
1 (7) |
Advising on care and rehabilitation |
6 (40) |
Channeling communication through key members |
15 (100) |
Identifying major dysfunction and referring |
0 |
Level 3. feeling and support |
Eliciting concerns and feelings |
8 (53) |
Empathic listening and normalization |
5 (33) |
Assessing family functioning |
10 (67) |
Encouraging family coping |
0 |
Tailoring advice to family needs |
6 (40) |
Tailoring referral to family context |
0 |
Level 4. Systemic assessment and planned intervention |
Engaging families in planned conferences |
9 (60) |
Structuring inclusive family conferences |
12 (80) |
Systematic assessment of functioning |
10 (67) |
Supporting individuals without coalitions |
0 |
Reframing family problem definitions |
1 (7) |
Promoting collaborative coping efforts |
1 (7) |
Generating alternative coping strategies |
5 (33) |
Balancing family roles and autonomy |
13 (87) |
Orchestrating referral beyond primary care |
0 |
Level 5. Family therapy |
Interviewing hard-to-engage families |
0 |
Testing hypotheses about interaction patterns |
2 (13) |
Escalating conflict to break impasses |
0 |
Strategic temporary siding |
0 |
Managing strong resistance to change |
1 (7) |
Negotiating with external professionals/systems |
3 (23) |
Descriptions of learning and practice were organized according to the ALACT model. For the Action stage, practices were additionally mapped to the Levels of Physician Involvement With Families framework (Table 4).
ALACT stage |
Category |
Concepts |
Action (triggers) |
Clinician-related |
Negative emotions; ethical issues; over-involvement; difficulty at turning points |
Patient- and family-related |
Family distress; disagreements; need for dialogue; isolation; relationship changes |
Action (practice) |
Information/advice |
Medical explanations; treatment plans |
Feeling/support |
Identifying anxieties; empathic listening; tailored advice |
Systemic intervention |
Family conferences; ensuring expression; functional assessment; role adjustment; supporting coping |
Family therapy |
Interprofessional collaboration |
Looking back on the action |
Clinician self-evaluation |
Reduced distress; broader perspective |
Patient/family evaluation |
Emotional changes; shared understanding; relationship changes |
Practice evaluation |
Conference effectiveness; support effectiveness |
Awareness of essential aspects |
Awareness of one’s own support |
Emotional insight; circular perspective; awareness of mediating role |
Connection with family medicine expertise |
Continuity—comprehensiveness link; comprehensiveness over time |
Connection with society |
Family—society intersection |
Creating alternative methods of action |
Promoting family understanding |
Emotional understanding; family relationships; life-cycle perspective |
Improving family-approach techniques |
Conference skills; decision-support skills |
Creating learning opportunities |
Reflective opportunities; ongoing learning |
Action
At the Action stage, residents described the triggers and content of their family-oriented care practices. The triggers were mapped to two categories: clinician-related factors and patient- and family-related factors (Table 4).
With respect to practice, several portfolios detailed efforts to build trust and collaborate with families through empathetic listening, providing advice, conducting family conferences, and facilitating the sharing of opinions and adjustment of roles. These practices mapped to Levels 2–4 of the Levels of Physician Involvement With Families framework, while Level five involvement was observed only in a single training program in a specific region (Table 3).
For example, in the following case, a family conference was convened to address disagreements among family members. The physician facilitated the discussion while attending to the emotions involved and ensured that all participants, despite holding different perspectives, could express their views comfortably:
“The eldest son’s wife, who frequently visited the hospital as a key person, did not seem to welcome the patient’s discharge to home. . . . Therefore, we decided to hold a conference to adjust opinions. . . . The author explained to everyone that the goal of the conference was to discuss how to ensure that the patient could safely continue their convalescence and organized the issues based on patient-centered care methods.” (Portfolio No. 2).
Looking Back on the Action
At the Looking Back on the Action stage, residents evaluated the outcomes of their practice, generally in a concrete and descriptive manner. Reflections were mapped to three categories: clinician self-evaluation, patient/family evaluation, and evaluation of practice content (Table 4).
For example, in the following case, the resident concluded that the family conference had been effective after developing a support plan based on viewing the family as a whole system:
“By understanding the differences in the family life cycles of the ‘patient couple’ and ‘patient’s children,’ viewing the patient’s family as a system, discussing the thoughts and concerns of those involved, identifying care resources, and devising a plan, it was reflected that the fifth stage of the family conference was achieved.” (Portfolio No. 11)
Awareness of Essential Aspects
While Looking Back on the Action involved descriptive evaluation of past events, the Awareness of Essential Aspects stage reflected deeper interpretive insight into the emotions, assumptions, and meanings underlying residents’ actions. These insights were mapped to three categories:
Awareness of One’s Own Support
Residents recognized their emotional responses, their communication patterns, and their role as mediators of change, and how their own habitual perspectives shaped the interaction. For example:
“Joining with patients is important, but in cases where I feel that a vicious cycle is occurring, I have learned that it is effective to change myself, that is, to change my perspective, become aware of the system surrounding the case, and intervene. I understood my own tendency to empathize with the patients in front of me.” (Portfolio No. 15)
Connection With Family Medicine Expertise
Residents recognized the alignment between family-oriented care and the core principles of continuity and comprehensiveness, conceptualizing these principles from a longitudinal family perspective. For example:
“Family-oriented care provided by family physicians, who engage with patients not only in terms of disease but also continuously and comprehensively, allows individuals to navigate life events appropriately and receive support for their growth.” (Portfolio No. 3)
Connection With Society
Residents reflected on broader social issues, recognizing how family-oriented care intersects with societal challenges such as aging and caregiver burden. For example:
“Care for the burden of family caregiving is essential in Japan as it faces an aging society, and I want to be a doctor who cares for families while also considering the ‘family tree.’” (Portfolio No. 8).
Creating Alternative Methods of Action
At the Creating Alternative Methods of Action stage, residents reflected on strategies to deepen their understanding of families, strengthen their support skills, and sustain ongoing learning. Reflections were mapped to three categories: promoting family understanding, improving family-approach techniques, and creating learning opportunities (Table 4).
For example, in the following case, the resident recognized the need to develop skills for conducting structured family conferences beyond the brief discussions typically held during routine visits:
“The counseling session conducted this time to bring about changes in the family was a family counseling session within the context of a regular visit. In the future, there will be families for whom changes are difficult to achieve through counseling sessions within regular visits alone. As the next step, I would like to learn the method of family conferences conducted separately from regular medical care opportunities.” (Portfolio No. 7)
This study explored how family medicine residents in Japan learn and practice family-oriented care through analysis of their certification portfolios. By examining reflective narratives, the study provides insight into developmental processes that have received limited empirical attention, particularly within portfolio-based research.
Residents’ reflections indicated that learning family-oriented care involved more than acquiring knowledge and technical skills. Many described shifts in clinical perspectives and attitudes, particularly within the Awareness of Essential Aspects stage of the ALACT model. These reflections included recognizing their emotional reactions, adopting circular perspectives, and understanding their role as mediators of change within family systems. Such developments align with the systemic paradigm of family therapy, which emphasizes relational meaning-making.19
However, the depth of reflection varied considerably. Some narratives remained primarily descriptive or limited to basic self-evaluation, illustrating the need for structured educational support to facilitate deeper reflective practice. Prior research has highlighted the value of supervision, Balint groups, genogram-based exploration, and Person of the Therapist Training in helping trainees link emotions, interpretations, and clinical encounters.20-23 Similarly, prior reports have described residency programs that incorporate these approaches into curricula.24 In contrast, our findings suggest, in the Japanese context, that these competencies are not necessarily provided through structured curricula but are often learned through everyday clinical experience and reflection. Developing effective strategies to support such learning remains an important challenge.
In terms of practical content, residents most frequently described empathic engagement, tailored advice, and information sharing or role negotiation during family conferences. These findings are consistent with studies emphasizing emotional attunement and collaborative decision-making as central to family-oriented care.25 In contrast, explicit interventions targeting family relationships or reflections on emotional involvement were less common. These higher-order practices require not only an understanding of family systems but also interview techniques for exploring family functioning—areas in which training opportunities remain limited.26 Strengthening these skills through systematic educational design may support residents in moving beyond supportive communication toward more systemic engagement.
Context-sensitive flexibility also emerged as an important element of practice. Some portfolios described one-way or overly directive conferences, whereas others achieved high-level family engagement without a formal conference. These findings suggest that educational emphasis should be placed on clinical judgment and responsiveness rather than on viewing family conferences as an end in themselves.27,28
Variation across training environments further shaped learning opportunities. Level five involvement appeared only in portfolios from a single program in a region with limited medical resources, suggesting that local context and educational environments influence opportunities for deeper family engagement. Differences in family life-cycle stages also were observed. Many cases involved end-of-life care, likely reflecting clinical demands related to decision-making and grief support.29 In contrast, cases involving couples or families with typically developing children were sparse, echoing broader challenges in Japan, such as shortages of child mental health specialists and regional disparities in service availability.30,31 These gaps highlight potential areas for strengthening residency curricula.
In the Japanese context, limited availability of family therapists and mental health professionals in primary care has been reported, often requiring family physicians to manage complex family-related issues themselves.32 While this context increases the importance of family-oriented care in clinical practice, opportunities for structured training and supervision remain limited. As a result, these competencies often are learned through everyday clinical experience rather than formal curricula. These factors also may be related to sociocultural norms regarding family roles and relationships, which further shape how family-oriented care is practiced and learned in Japan. These norms may differ from some settings where referral to such specialists is more readily available.
This study had several limitations. First, evaluation portfolios emphasize what was learned, which may underrepresent the cognitive processes underlying learning.33 Because portfolios represent final submissions for certification, early trial-and-error or unsuccessful attempts may be omitted. Second, portfolio narratives primarily capture reflection-on-action, whereas immediate, in-the-moment learning (reflection-in-action) is difficult to document in writing.12 Third, cases were selected at the discretion of each resident and may not fully represent daily clinical practice. The quality of practice cannot be comprehensively assessed from written descriptions alone,34 and future research combining portfolios with interviews or direct observation may deepen understanding. Furthermore, we did not systematically assess the influence of specific educational components, such as Balint groups or other reflective practices, which may have influenced the findings. Finally, the Levels of Physician Involvement With Families framework may not fully align with the constraints of busy primary care settings. In particular, higher levels of family involvement may be difficult to implement consistently in such settings. Flexible, context-sensitive educational goals may therefore be needed as family medicine continues to evolve.
This study demonstrated that the acquisition of family-oriented care involves a reflective process that extends beyond knowledge and skills, encompassing shifts in clinical attitudes and professional identity. However, residents varied in their insight into family relationships, their ability to support bidirectional decision-making, and the depth of their reflection, indicating a need for targeted educational support. In the Japanese context, these competencies may be learned through everyday clinical experience rather than through structured curricula. These findings highlight the importance of developing educational strategies that support structured reflective learning while preserving context-sensitive practice in family-oriented care.
Presented at the 16th Annual Conference of the Japan Primary Care Association, June 20–22, 2025, Sapporo, Hokkaido, Japan.
The authors acknowledge the Kameda Family Medicine Residency Program, the Mie University General Practice Residency Program, and the Nagoya University General Practice Residency Program for their support with data collection.
References
-
-
Haley WE, Elayoubi J. Family caregiving as a global and lifespan public health issue.
The Lancet Public Health. 2024;9(1):e2–e3. doi:10.1016/S2468-2667(23)00227-X
-
-
-
-
-
-
Schiefer R, Levy S, Rdesinski RE, Garvin RD, Verdieck A, Skariah JM. Impact of a residency family systems curriculum on the postresidency practice of family physicians.
Fam Med. 2024;56(1):35–37. doi:10.22454/FamMed.2023.411218
-
Schiefer R, Levy S, Rdesinski R. A family systems curriculum: evaluating skills and empathy.
Fam Med. 2021;53(1):54–57. doi:10.22454/FamMed.2021.391849
-
Stewart M, Brown JB, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-Centered Medicine: Transforming the Clinical Method. 3rd ed. CRC Press; 2013.
10.1201/b20740
-
Wright LM, Leahey M. Nurses and Families: A Guide to Family Assessment and Intervention. 6th ed. F.A. Davis Company; 2013.
-
Mann K, Gordon J, MacLeod A. Reflection and reflective practice in health professions education: a systematic review.
Adv Health Sci Educ Theory Pract. 2009;14(4):595–621. doi:10.1007/s10459-007-9090-2
-
-
Van Tartwijk J, Driessen EW. Portfolios for assessment and learning: AMEE Guide no. 45.
Med Teach. 2009;31(9):790–801. doi:10.1080/01421590903139201
-
Tochel C, Haig A, Hesketh A, et al. The effectiveness of portfolios for post-graduate assessment and education: BEME Guide No 12.
Med Teach. 2009;31(4):299–318. doi:10.1080/01421590902883056
-
Korthagen FAJ, Kessels J, Koster B, Lagerwerf B, Wubbels T. Linking Practice and Theory: The Pedagogy of Realistic Teacher Education. Routledge; 2001.
doi:10.4324/9781410600523
-
Doherty WJ, Baird MA. Developmental levels in family-centered medical care. Fam Med. 1986;18(3):153–156.
-
-
Goldenberg H, Goldenberg I. Family Therapy: An Overview. 8th ed. Cengage Learning; 2012.
-
Van Roy K, Vanheule S, Inslegers R. Research on Balint groups: a literature review.
Patient Educ Couns. 2015;98(6):685–694. doi:10.1016/j.pec.2015.01.014
-
Kilminster S, Cottrell D, Grant J, Jolly B. AMEE guide no. 27: effective educational and clinical supervision.
Med Teach. 2007;29(1):2–19. doi:10.1080/01421590701210907
-
McGoldrick M, Gerson R, Petry SS. Genograms: Assessment and Intervention. : 3rd ed . Norton; 2008
-
Aponte HJ, Kissil K, eds. The Person of the Therapist Training Model: Mastering the Use of Self. Routledge; 2016.
doi:10.4324/9781315719030
-
Garcia-Huidobro D, Soto G, Victoria Rodgriguez M, vonBorries P, Rivera S. Teaching family-oriented patient care to family medicine residents in Chile.
Fam Med. 2025;57(5):381–384. doi:10.22454/FamMed.2025.245190
-
Takenaka H, Ban N, Suzuki T, Tokuyama H, Sato J. General physicians’ perceptions of family approach in Japan: a qualitative study. Qual Prim Care. 2016;24(2):88–93.
-
Smith RC, Fortin LM, eds. Smith’s Patient-Centered Interviewing: An Evidence-Based Method. 3rd ed. McGraw-Hill; 2015.
-
-
-
Doherty WJ, Mendenhall TJ. Citizen health care: A model for engaging patients, families, and communities as coproducers of health.
Families, Systems, & Health. 2006;24(3):251–263. doi:10.1037/1091-7527.24.3.251
-
-
Takei A. Supporting children with developmental disabilities in the community: collaboration between pediatrics and community support. Shonika Rinsho. 2022;75(5):813–819.
-
Takenaka H, Suzuki T, Date J, Kusaba T, Sato J, Ban N. What kinds of family involvement do family physician in Japanese clinics provide? a survey by focus group discussion [report 2].
J Jpn Prim Care Assoc. 2019;42(1):40–46. doi:10.14442/generalist.42.40
-
Tillema H, Smith K. Portfolio appraisal: In search of criteria.
Teaching and Teacher Education. 2007;23(4):442–456. doi:10.1016/j.tate.2006.12.005
-
Govaerts M, van der Vleuten CPM. Validity in work-based assessment: expanding our horizons.
Med Educ. 2013;47(12):1164–1174. doi:10.1111/medu.12289



There are no comments for this article.