Background and Objectives: Burnout is a growing concern in health care, leading to consequences such as reduced working hours and early retirement. Federally qualified health centers (FQHCs) may be particularly susceptible because they often are located in under-resourced settings; however, research specific to FQHCs is limited. This review aims to fill this gap by examining the level of burnout in FQHCs, contributing factors, and potential mitigation strategies.
Methods: We conducted a literature search using PubMed, Scopus, and PsychINFO to identify studies related to FQHCs and burnout. We included studies that addressed burnout levels, contributing factors, or mitigation strategies. We then charted data from eligible studies into tables, with two authors independently reviewing entries. Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines were followed.
Results: The majority of the 13 eligible studies surveyed providers and staff in FQHCs to examine the level of burnout, contributing factors, and potential mitigation strategies. Several linked working in FQHCs to increased burnout risk, while others explored causes such as resource scarcity and compensation differentials. Proposed mitigation strategies included boundary-setting sessions, increased reimbursement, and mental health support. Several studies evaluated burnout prevention programs, showing promising results but lacking comprehensive evaluation.
Conclusions: This scoping review highlights the need for more research on burnout in FQHCs and the importance of validating intervention strategies. Addressing burnout in FQHCs is crucial for mitigating health disparities and ensuring optimal health care delivery to vulnerable populations.
Burnout is a work-related syndrome characterized by emotional exhaustion, depersonalization, and a feeling of reduced personal accomplishment.1 More than half of health care workers have reported experiencing some degree of burnout.2,3 Leading causes include a stressful work environment, poor workplace management, loss of autonomy, and overreliance on computer systems and electronic medical records.4
Burnout in physicians has multiple consequences, including elevated levels of depression, substance use disorder, and an increased risk of suicide.5 Furthermore, burnout drives many physicians to reduce working hours or consider early retirement.6 Similar consequences are observed among nurses who leave their positions early, increase requests for sickness-related absences, and report poorer overall health.7 The impact of burnout extends to patients as well. Lower patient satisfaction, poorer health care quality, reduced patient safety, increased medical errors, and increased patient recovery time are additional impacts of burnout in health care.8-10
Despite extensive research conducted within larger academic institutions, data regarding burnout among federally qualified health centers (FQHCs) remain scant. FQHCs are public, government-funded centers that provide affordable and accessible primary care to underserved populations and/or geographical areas.11 FQHCs often are located in areas experiencing physician shortages, making the prevention of burnout and burnout-related turnover especially important.12 With this background in mind, examining the level of burnout, factors contributing to burnout, and potential mitigation strategies for burnout among FQHC providers and staff is important. This review specifically explores the existing literature on burnout in the FQHC settings to summarize current findings, identify research gaps, and consider potential solutions.
Search Strategy
We conducted a literature search to examine the level of burnout in FQHCs using PubMed, Scopus, and PsychINFO on January 15, 2024. We conducted searches across all indexed fields using the following search string: ([FQHC*] OR [“Federally Qualified Health Center*”]) AND [burnout]). In PubMed, the Medical Subject Heading (MeSH) term “Burnout, Professional” was also included. Searches were limited to studies published in English.
Eligibility and Study Selection
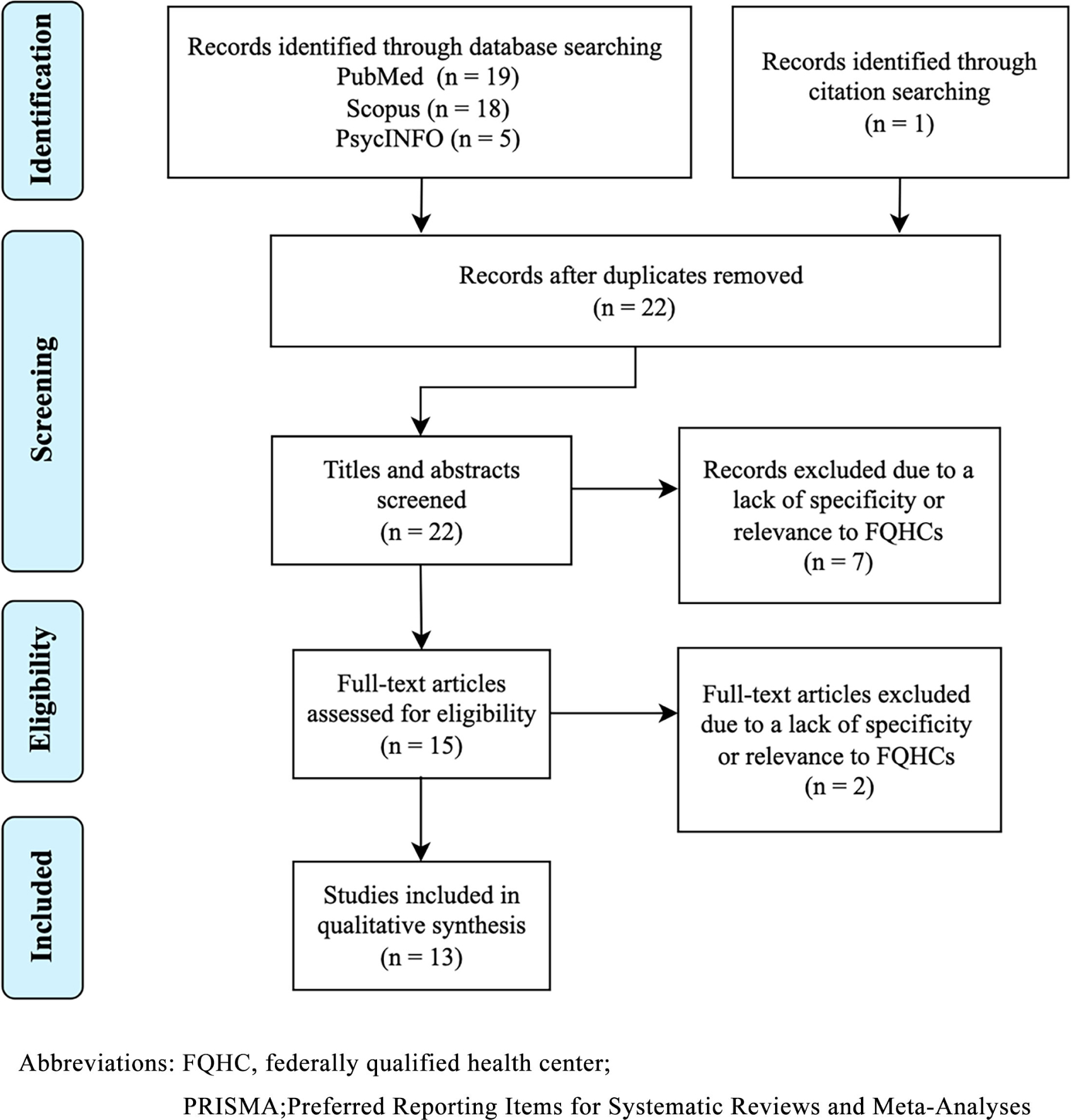
Studies were eligible for inclusion if they focused on health care providers or staff in FQHCs and addressed the level, causes, or impacts of burnout, or mitigation strategies for burnout. Eligible study designs included empirical studies, program evaluations, case reports, scoping or narrative reviews, and meta-analyses. Studies were excluded if they were not conducted in FQHCs, did not address burnout, were not available in full text, or were nonresearch in nature, such as editorials, commentaries, or letters. Articles were then screened for relevance based on titles, abstracts, and full text. Additionally, the reference sections of the identified sources were reviewed to identify other potentially relevant literature. Two authors independently conducted study selection, resolving disagreements through consensus. The study selection process is summarized in Figure 1.
Data Extraction and Synthesis
Data extraction was performed independently by two authors, with any discrepancies resolved by consensus. Extracted data included study type, study participants, sample size, practice type, and selected findings. These data were then charted into Table 1. Selected findings were those related to the level, causes, impacts, and mitigation strategies of burnout among FQHC providers and staff. “Level” of burnout was defined as any reported measure of burnout, including percentages meeting thresholds, odds ratios, or mean scores. When studies reported additional outcomes, only those directly related to these variables were extracted.
References |
Study type |
Study participants |
Sample size |
Practice type |
Selected findings |
Burnout measurement tool |
Edwards et al, 201814 |
Survey |
Physicians, APCs, and staff |
N = 10,284 |
Independent, hospital-owned, FQHC, and other |
Higher rates of burnout at FQHCs compared to independent practices |
Single-item burnout question |
Cuellar et al, 201815 |
Survey |
Physicians, APCs, and staff |
N = 2005 |
Independent, hospital system, FQHC |
Similar rates of burnout at FQHCs and independent practices |
Single-item burnout question |
Friedberg et al, 201716 |
Survey |
Physicians, APCS, and staff |
N = 564 |
FQHC |
Increasing burnout rates in FQHCs |
Burnout assessed via author-designed survey; instrument not named |
Hill et al, 202317 |
Survey |
Physicians, BHCs, and CHWs |
N = 74 |
FQHC |
Higher rates of burnout in FQHCs during the COVID-19 pandemic |
Maslach burnout Inventory—human services survey for medical personnel |
Stupplebeen et al, 201918 |
Semistructured group interview |
CHWs, clinicians, and administrators |
N = 13 |
FQHC |
Burnout attributed to sense of working 24/7 due to living in community served and fulfilling numerous grant-specific roles |
Qualitative thematic analysis |
Martinez-Hollingsworth et al, 202119 |
Semistructured interview |
Administrators |
N = 14 |
FQHC |
Differing causes of burnout based on what motivates a provider to work at an FQHC |
Qualitative thematic analysis |
Jung et al, 202320 |
Survey |
Providers and staff |
N = 1417 |
FQHC |
Mitigation strategies should focus on enhancing manager communication, providing perks, and fostering camaraderie. |
Not applicable |
Sullivan et al, 202221 |
Survey |
Clinicians |
N = 506 |
FQHC |
Respondents commented that they believe they would benefit from employer-paid time to seek assistance for burnout. |
Single-item burnout question |
Filteau et al, 202122 |
Qualitative interview |
Clinicians, staff, and patients |
N = 90 |
Hospital, IMAT clinic, FQHC |
Burnout among staff was attributed to forsaking own well-being to meet local demand for treatment. multidisciplinary team approaches were recommended for preventing burnout |
Qualitative thematic analysis |
Powell & Yuma-Guerrero, 201623 |
Intervention, survey, semistructured interview |
Staff |
N = 69 |
FQHC |
Significant decrease in acute stress after intervention, thus reducing the likelihood of burnout |
Professional quality of life scale, burnout subscale |
Cauley et al, 202224 |
Intervention, qualitative interview |
Clinicians |
N = 28 |
FQHC |
Wellness initiative was appreciated but did not address underlying causes of burnout. |
Qualitative thematic analysis |
Hurley-Kim et al, 202325 |
Prospective assessment and reporting of experiences |
Pharmacists |
N = Not defined |
FQHC |
Pharmacists addressed 9.2% of the refill requests within 48 hours 87.8% of the time. |
Not applicable |
Longo et al, 202326 |
Survey |
Performance/quality improvement professionals, executive-level leaders, accreditation specialists/ professionals, and administrators |
N = 481 |
Joint commission accredited hospital, FQHC |
Most FQHCs did not have a funded leadership position responsible for assessing and promoting clinician well-being or a wellness committee. more than half of FQHCs implemented targeted interventions for burnout. |
Not applicable |
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines.13 A review protocol was not registered. Consistent with scoping review methodology, no formal critical appraisal of included studies was conducted. Sources of funding for the included studies were not systematically collected. The scoping review itself did not receive funding. The Penn State College of Medicine Institutional Review Board (IRB) determined that this study does not meet the definition of human subject research; therefore, IRB review and approval were not required.
Description of the Study Populations
Of the 13 eligible studies, clinicians were surveyed in nine and staff were surveyed in 10 (Table 1).14-26 Performance and quality improvement professionals, executive-level leaders, accreditation specialists, and patients were each represented in only one study.22,26 Thirteen studies included FQHCs, and two included independently owned and hospital-owned practices.14,15
Studies Measuring Level of Burnout at FQHCs
Four of the 13 studies focused on exploring the relationship between working at an FQHC and the level of provider and staff burnout.14-17 Edwards et al. found that people who worked in hospital/health-system-owned practices or an FQHC had higher odds of burnout (aOR = 1.42, CI = 1.16,1.73; and aOR = 1.36, CI = 1.03,1.78, respectively) and higher rates of burnout (22.9% and 21.6%, respectively) compared to those working in physician/advanced practice clinician-owned practices (18.3%).14 Cuellar et al. found that mean burnout scores in FQHCs were higher than in hospital-owned practices and similar to independent practices.15 Friedberg et al. demonstrated that burnout rates in FQHCs were increasing, from 23%–31.5% over the 1 year study period, but did not compare these rates to hospital-owned or physician-owned practices.16 Hill et al. also demonstrated an increase in burnout, from 20.5%–22.9% over the 18 month study period, but noted that the COVID-19 pandemic emerged during the study.17
Studies Investigating Causes of and Mitigation Strategies for Burnout
Five of the 13 studies focused on understanding the causes of and proposing mitigation strategies for burnout in FQHCs (Table 2).18-22 Two analyzed burnout in general and found that leading causes included feeling as if they were working 24/7 because of living in the communities they served, needing to fulfill grant-specific responsibilities, working in resource-scarce environments, lacking time to pursue health equity work, and receiving lower compensation in FQHCs.18,19 In these studies, mitigation strategies were proposed by administration. Strategies included boundary-setting sessions, increased insurance reimbursement to reduce the need for specific grants, training providers to expect diminished patient compliance, implementing a buyout program to give providers time to volunteer, encouraging providers to practice their full scope for increased pay, and continuing with student loan forgiveness programs.18,19 One study did not analyze causes, but rather collected recommendations from clinicians and staff for mitigation strategies.20 They recommended that strategies should focus on improving communication with managers, offering workplace perks, and cultivating a sense of camaraderie.
Causes |
Mitigation strategies |
Job feels like it is 24/7 because workers live in the communities that they serve.18 |
Boundary-setting sessions18 |
CHW must fulfill a number of grant-specific roles due to the variety of funding sources.18 |
Increase funding for CHW through statewide policies on reimbursement or other funding mechanisms such as global payment.18 |
Frustrating working in a resource-scarce community19 |
Train providers to expect diminished patient compliance.19 |
The demanding role of a CHW puts stress on their support systems.19 |
Train providers in the need for bonding with peers and support peer-mentorship networks.19 |
Lower compensation in FQHCs19 |
Support providers in working to the top of their scope of practice and continue student loan forgiveness.19 |
Lack of time in their schedule to do things they are passionate about19 |
Buy out providers time to allow them to volunteer or contribute to research.19 |
Struggle to balance local demand for addiction management treatment, and provider availability22 |
Expand addiction management access in rural and underserved communities.22 |
Lack of time to receive mental health support and/or for wellness activities21 |
Dedicated time to receive support or take breaks during working hours21 |
The remaining two studies analyzed specific cases of burnout: burnout due to work with opioid use disorder patients and burnout following a stressful event.21,22 A cause of burnout when working with opioid use disorder patients was the struggle to meet the local demand. Respondents recommended multidisciplinary team approaches to medication-assisted treatment, which could help reduce the responsibility falling onto one person.22 One cause of burnout following a stressful event was difficulty accessing support. Survey respondents stated that they would benefit from employer-paid time to seek assistance, such as dedicated time for seeking assistance or being allowed to use sick hours, rather than vacation hours, to seek mental health assistance.21 While all five studies suggested mitigation strategies, none mentioned the implementation of these strategies.
Studies Evaluating Burnout Prevention Programs
Four of the 13 studies evaluated programs that were implemented to mitigate burnout at FQHCs.23-26 Three of these four studies discussed specific programs, the Resilience and Coping for the Healthcare Community (RCHC) program, a pharmacist-managed refill service, and the Physician Wellness Initiative (PWI).23-25 The RCHC program was developed in response to the distress health care workers faced after Hurricane Sandy and uses psychoeducation to help health care workers recognize and cope with disaster-related stress. Results showed increased knowledge and reduced acute stress after attendance of the workshop.23 The pharmacist-managed refill service was created to help reduce the administrative burden on primary caregivers and was set up so that pharmacists could dedicate approximately 3 hours to the pilot per week. A 1 year evaluation of the service showed that pharmacists addressed 9.2% of the refill requests within 48 hours 87.8% of the time.25 No data were available on how this service impacted administrative burden or burnout. The PWI program was a yearlong wellness initiative developed based on common interventions to reduce burnout, such as idea boards and holiday parties. A 1 year evaluation revealed that while the clinicians appreciated the efforts, they did not address the underlying causes of burnout, such as work-life imbalance and staff shortages.24
To provide an overview of burnout prevention programs more widely, the fourth study surveyed FQHCs about the programs they offer.26 More than half of FQHC respondents implemented targeted interventions for burnout, such as making workflow changes or flexible work arrangements. However, only 5.4% of FQHCs established a funded leadership position responsible for assessing and promoting clinician well-being, and only 29.3% established a wellness committee.26 The results did not include the effectiveness of the interventions or positions. Of the four studies evaluating burnout prevention programs, none of them externally validated the results, and two did not comment on the effectiveness of these programs in burnout prevention.
This scoping review of 13 studies highlights the persistent reporting of physician burnout within FQHCs. Four studies examined the association between FQHCs and burnout, with two indicating higher odds of burnout in FQHCs compared to at least one other setting and two suggesting an increasing trend in burnout rates.14-17 Additionally, five studies identified common causes of burnout and proposed mitigation strategies.18-22 Causes included resource shortages, compensation differentials, and lack of mental health support.18,19,21 Proposed mitigation strategies ranged from external and systems-level reforms to internal and organizational-level supports.18-22 Systemic reforms, often suggested by administration, included increasing insurance reimbursements and maintaining federal loan forgiveness programs.18,19 Internal supports, recommended by administration, providers, and staff, included boundary-setting sessions, dedicated mental health support, provider buyout programs, and improved workplace camaraderie.18-21 Notably, none of the studies that proposed mitigation strategies assessed their implementation. Finally, four studies evaluated burnout prevention programs.23-26 While two assessed the effectiveness of burnout mitigation, they have not been implemented elsewhere, limiting their generalizability.23,24
The review’s findings are unsurprising given the presence of stressors that are more specific to these settings. Unlike many nonsafety-net practices, FQHCs operate with resource shortages and compensation differentials that create conditions that may uniquely contribute to burnout. Although the underlying causes of burnout may differ across practice types, exploring whether burnout prevention programs validated in academic or private practice settings could be adapted for use in FQHCs may have value. For example, continuing medical education focused on burnout and 12 hour shifts has been shown to be effective and could potentially alleviate burnout in FQHCs, regardless of not addressing the underlying FQHC-specific causes.27
Despite offering crucial insights into burnout within FQHCs, this review also reveals several limitations. First, the reliance on self-reported burnout data and use of differing measurement instruments limits comparability. Second, the aggregation of physicians, advanced practice clinicians, and staff, and the exclusion of learners, such as medical students and residents, limits insights into how burnout differs across roles and levels of training. Third, the lack of studies measuring the efficacy of interventions weakens the validity of proposed strategies, because whether these interventions would be truly effective remains unclear. This limits actionability for both policymakers and FQHC administrators, who would be responsible for implementing these changes. Fourth, FQHCs vary by location, funding, and size, which may contribute to differences in burnout drivers and limit comparability across studies. Finally, consistent with PRISMA-ScR guidance, this scoping review is subject to methodological limitations related to the search strategy and study selection process, which may have resulted in the omission of relevant evidence.
To our knowledge, this is the first scoping review focusing on physician burnout within FQHCs. By providing a comprehensive overview of the existing literature on this historically understudied topic, this review contributes to the understanding of different facets of FQHC-related burnout. However, the scarcity of research, particularly into the implementation and outcomes of proposed interventions, reinforces the need for further investigation.
The existing literature underscores gaps in understanding and investigating burnout within the FQHC context. Across studies, FQHCs consistently reported higher burnout rates than other practice types, although the relative burnout in the other groups varied (hospital-owned versus physician-owned practices), and some analyses were limited by small sample sizes. Research on exploring and validating the proposed intervention strategies to address this problem was also limited, which presents a key barrier to implementing these strategies.
The implications of unaddressed burnout in FQHCs extend far beyond compromised physician well-being. Considering that FQHCs care for the medically underserved, the risk of perpetuating health disparities among these communities becomes particularly heightened when physicians are expected to provide care in suboptimal states.
Future work should expand on the causes of burnout in FQHCs and mitigation strategies, as well as implement and validate proposed strategies. Exploring wellness programs used in non-FQHC settings may help identify transferable approaches for FQHCs. Standardizing burnout measurement across studies would strengthen the evidence base, allowing for clearer cross-study comparisons. Additional research is also needed to assess the impact of burnout in FQHCs on provider and staff retention, as well as on learners’ interests in pursuing careers in FQHC settings. With stronger evidence, policymakers and FQHC administrators can be better prepared to make informed decisions and enact meaningful changes to improve workforce well-being and patient care outcomes.
Presented at the American Academy of Family Physicians’ Physician Well-Being Conference, April 25, 2023, Palm Springs, California.
The authors acknowledge Brad Long for his assistance with the methodology.
References
-
-
Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014.
Mayo Clin Proc. 2015;90(12):1600–1613. doi:10.1016/j.mayocp.2015.08.023
-
Prasad K, McLoughlin C, Stillman M, et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: a national cross-sectional survey study.
EClinicalMedicine. 2021;35:100879. doi:10.1016/j.eclinm.2021.100879
-
Fred HL, Scheid MS. Physician burnout: causes, consequences, and (?) cures.
Tex Heart Inst J. 2018;45(4):198–202. doi:10.14503/THIJ-18-6842
-
Ryan E, Hore K, Power J, Jackson T. The relationship between physician burnout and depression, anxiety, suicidality and substance abuse: a mixed methods systematic review.
Front Public Health. 2023;11:1133484. doi:10.3389/fpubh.2023.1133484
-
Landon BE, Reschovsky JD, Pham HH, Blumenthal D. Leaving medicine: the consequences of physician dissatisfaction.
Med Care. 2006;44(3):234–242. doi:10.1097/01.mlr.0000199848.17133.9b
-
Shah MK, Gandrakota N, Cimiotti JP, Ghose N, Moore M, Ali MK. Prevalence of and factors associated with nurse burnout in the US.
JAMA Netw Open. 2021;4(2):e2036469. doi:10.1001/jamanetworkopen.2020.36469
-
West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study.
JAMA. 2006;296(9):1071–1078. doi:10.1001/jama.296.9.1071
-
Halbesleben JRB, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients.
Health Care Manage Rev. 2008;33(1):29–39. doi:10.1097/01.HMR.0000304493.87898.72
-
Stehman CR, Testo Z, Gershaw RS, Kellogg AR. Burnout, drop Out, suicide: physician loss in emergency medicine, part I.
West J Emerg Med. 2019;20(3):485–494. doi:10.5811/westjem.2019.4.40970
-
-
Xue Y, Greener E, Kannan V, Smith JA, Brewer C, Spetz J. Federally qualified health centers reduce the primary care provider gap in health professional shortage counties.
Nurs Outlook. 2018;66(3):263–272. doi:10.1016/j.outlook.2018.02.003
-
Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation.
Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
-
Edwards ST, Marino M, Balasubramanian BA, et al. Burnout among physicians, advanced practice clinicians and staff in smaller primary care practices.
J Gen Intern Med. 2018;33(12):2138–2146. doi:10.1007/s11606-018-4679-0
-
Cuellar A, Krist AH, Nichols LM, Kuzel AJ. Effect of practice ownership on work environment, learning culture, psychological safety, and burnout.
Ann Fam Med. 2018;16(Suppl 1):S44–S51. doi:10.1370/afm.2198
-
Friedberg MW, Reid RO, Timbie JW, et al. Federally qualified health center clinicians and staff increasingly dissatisfied with workplace conditions.
Health Affairs. 2017;36(8):1469–1475. doi:10.1377/hlthaff.2017.0205
-
Hill C, Justo S, Park H, et al. Pediatric provider and staff burnout in federally qualified community health centers.
J Ambul Care Manage. 2023;46(4):265–271. doi:10.1097/JAC.0000000000000472
-
-
Martinez-Hollingsworth A, Kim L, Richardson TG, et al. Supporting “bleeders” and “billers”: how safety-net administrators mitigate provider burnout during the COVID-19 pandemic and beyond.
J Ambul Care Manage. 2021;44(3):172–183. doi:10.1097/JAC.0000000000000383
-
Jung OS, Begum F, Dorbu A, Singer SJ, Satterstrom P. Ideas from the frontline: improvement opportunities in federally qualified health centers.
J Gen Intern Med. 2023;38(13):2888–2897. doi:10.1007/s11606-023-08294-1
-
-
Filteau MR, Kim FL, Green B. “It’s more than just a job to them”: a qualitative examination of patient and provider perspectives on medication-assisted treatment for opioid use disorder.
Community Ment Health J. 2022;58(2):321–327. doi:10.1007/s10597-021-00824-7
-
Powell T, Yuma-Guerrero P. Supporting community health workers after a disaster: findings from a mixed-methods pilot evaluation study of a psychoeducational intervention.
Disaster Med Public Health Prep. 2016;10(5):754–761. doi:10.1017/dmp.2016.40
-
Cauley AW, Green AR, Gardiner PM. Lessons learned from clinicians in a federally qualified health center: steps toward eliminating burnout.
J Integr Complement Med. 2023;29(3):196–203. doi:10.1089/jicm.2021.0401
-
Hurley-Kim K, Keyvani A, Ahmed R, Wong HW, McBane S. Pharmacist-managed refill service impacts on clinician workload and medication interventions in a federally qualified health center.
J Prim Care Community Health. 2023;14.
doi:10.1177/21501319231168716
-
Longo BA, Schmaltz SP, Williams SC, Shanafelt TD, Sinsky CA, Baker DW. Clinician well-being assessment and interventions in joint commission-accredited hospitals and federally qualified health centers.
Jt Comm J Qual Patient Saf. 2023;49(10):511–520. doi:10.1016/j.jcjq.2023.04.007
-
Matsuzaki PG, Mariya FA, Ueno LI, Gimenes MJF. Physician burnout: prevention strategies.
Rev Bras Med Trab. 2021;19(4):511–517. doi:10.47626/1679-4435-2021-713



There are no comments for this article.