
Individualized learning plans (ILPs) foster resident and fellow development of personalized learning goals.1 The Accreditation Council for Graduate Medical Education (ACGME) began requiring ILPs for all residents and fellows regardless of the presence of individual deficiencies in 2020;2 and, in family medicine, program directors (PDs) must guide faculty in mentoring ILPs.1 ILPs effectively identify and monitor personalized goals.2,3 Additionally, ILPs help develop master adaptive learners, preparing trainees for lifelong learning.1,4 We could find no published studies describing ILP content. We hoped that exploring ILPs within our health system would inform program, faculty, and resident development initiatives.
LEARNER RESEARCH
Faculty Perceptions of Individualized Learning Plans in Medical Education
Bryce A. Ringwald, MD | Jennifer L. Middleton, MD, MPH | Valerie Niedermier, MD
PRiMER. 2026;10:8.
Published: 3/5/2026 | DOI: 10.22454/PRiMER.2026.108285
Background and Objectives: Individualized learning plans (ILPs) enable learners to establish and track their personal educational goals, aiding their progression as master adaptive learners. Despite their significance, little research focuses on the content of ILPs. Our study aimed to detail the perceived content and implementation of ILPs within various residency and fellowship specialties across a large multihospital system.
Methods: We conducted an observational cross-sectional survey among faculty between July 27 and August 27, 2024. The survey was developed de novo following a thorough literature review and was piloted by experts to ensure its effectiveness. We aimed to evaluate the perceived content and execution of ILPs, with associations explored using descriptive statistics and χ2 tests.
Results: The survey had a response rate of 49.6% (112/226), with 60.7% (68/112) of respondents having an active role in ILP development and monitoring. Of those involved with ILPs, 60.3% (41/68) of responding faculty belonged to diagnostic specialties and 39.7% (27/68) to procedural specialties. Our analysis found no significant differences in the frequency of ILP reviews among different specialties. Procedural specialties placed a greater emphasis on career planning (P=.02, 5% vs 2%) and scholarly activity (P=.0019, 5% vs 1%), while diagnostic specialties prioritized medical knowledge (P=.0376, 16% vs 21%) and practice-based learning (P=.0021, 0% vs 3%).
Conclusions: We identified notable differences in the faculty perceptions of ILP content between procedural and diagnostic specialties. These insights may help guide resource allocation tailored to the specific needs of procedural and diagnostic program faculty.
We surveyed faculty in our large graduate medical education (GME) system to identify ILP advisors. Our original intention was to include thematic analysis of ILPs; our institutional review board (IRB), however, deemed ILPs as protected employee documentation. Given our inability to collect specialty data due to potential reidentification of anonymized data, we used a local distinction between diagnostic and procedural specialties to categorize responding programs. We chose these designations because programs such as anesthesiology, sports medicine, and osteopathic neuromuscular medicine are considered procedural specialties by our hospital system but are not surgical specialties. Our study team felt that the learning needs of procedure-focused specialties were similar due to their kinesiologic focus. We also were unable to ensure that respondents chose the correct category because the data were self-identified.
OhioHealth GME includes programs across five hospitals with 18 residency programs and eight clinical fellowship programs.5 Our system distinguishes specialties as diagnostic or procedural, which is how the data were collected and presented. Our system has nine residency programs in four diagnostic specialties (emergency medicine, family medicine, internal medicine, and psychiatry) and nine residency programs in six procedural specialties (anesthesiology, dermatology, OB/GYN, orthopedic surgery, otolaryngology, and general surgery). Fellowship programs include four diagnostic (addiction medicine, cardiology, geriatrics, and critical care) and five procedural (colorectal surgery, osteopathic neuromuscular medicine, sports medicine, surgical critical care, and trauma surgery) specialties. Our system has 26 PDs, 158 diagnostic faculty, and 42 procedural faculty.
The survey (see Appendix 1) was developed after an extensive literature review failed to reveal an appropriate validated questionnaire. Terminology was reviewed for understanding, and content was reviewed and revised by past PDs and former advisors who were not included in the study.6 The survey was administered electronically and was open from July 27 to August 27, 2024.
The survey collected information from faculty advisors and program directors on clinical specialty (diagnostic or procedural), perceived ILP content area (ACGME core competencies7 and non-ACGME core competencies), and ILP implementation (who reviews and how often).
We used descriptive statistics to describe ILP content, and implementation data were analyzed using R version 4.2.2 statistics software (R Foundation). To examine the differences between diagnostic and procedural specialties, content, and implementation, we used Pearson’s χ2 test, setting statistical significance at α=.05.
This study was deemed exempt by the OhioHealth IRB, Columbus, Ohio, on June 24, 2024.
The overall survey response rate was 49.6% (112/226), of which 60.7% (68/112) of responders identified as involved in ILPs and were allowed to complete the survey. From this group, 60.3% (41/68) of faculty were from a diagnostic specialty, and 39.7% (27/68) were from a procedural specialty. We found no significant differences between specialty of respondents and nonrespondents.
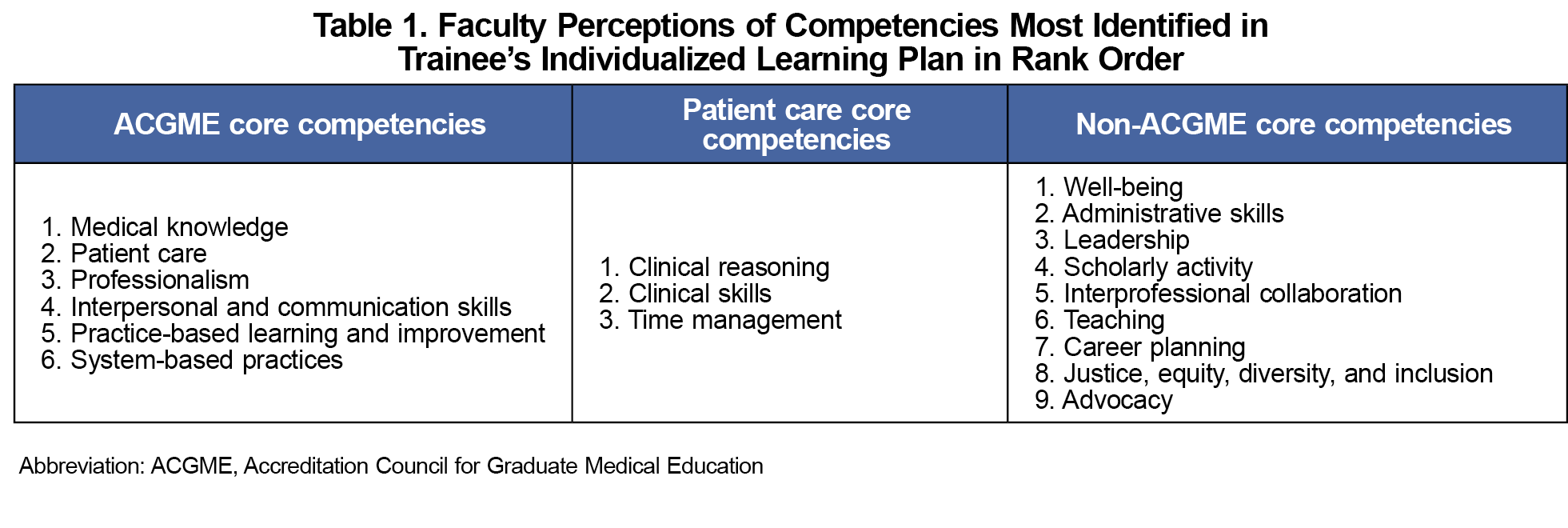
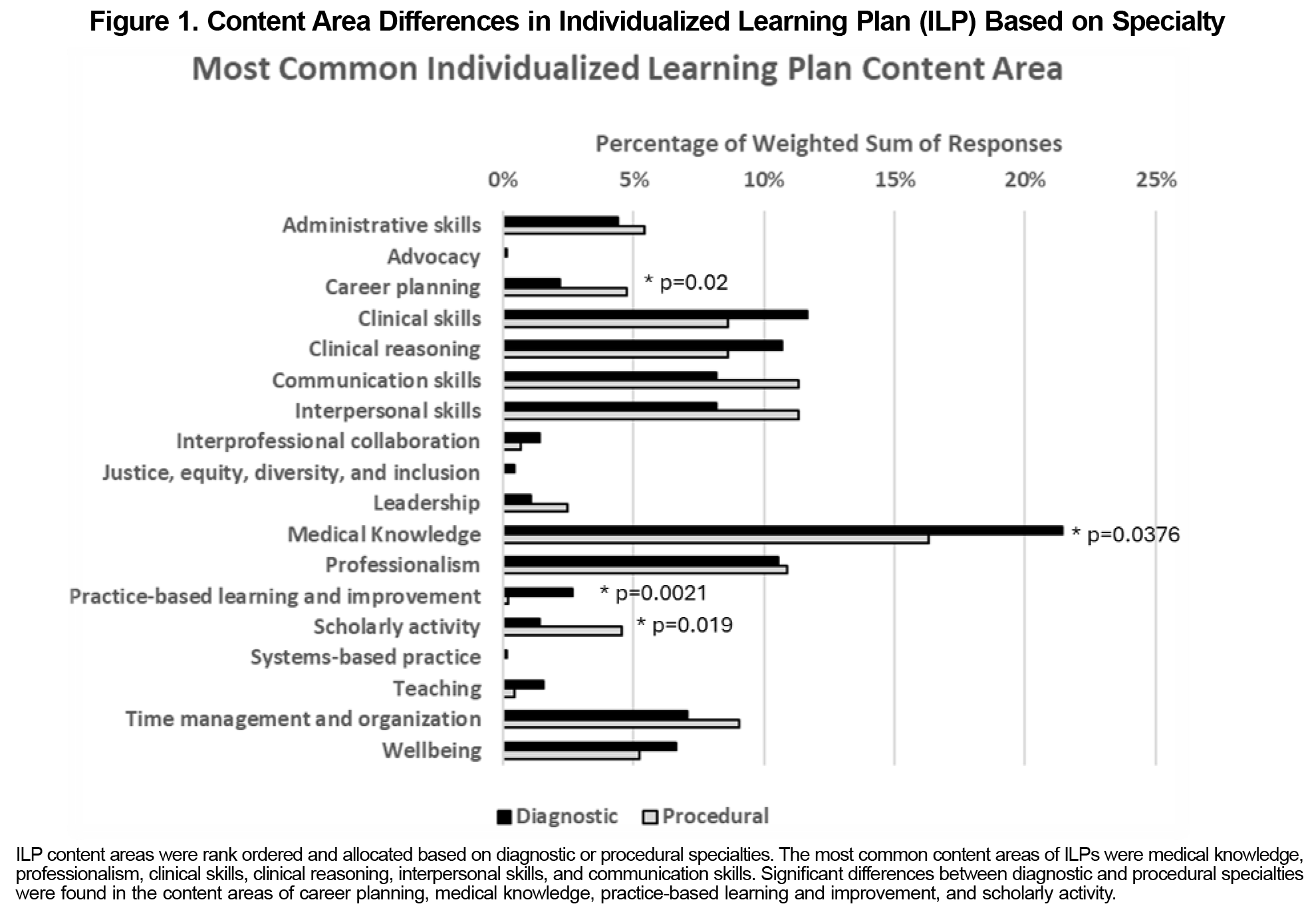
The ACGME core competencies of medical knowledge, patient care, and professionalism were the most common areas of an ILP’s focus (Table 1). Within the competency of patient care, clinical reasoning was the most common, followed by clinical skills and time management. The most common non-ACGME competencies were well-being, administrative skills, and leadership. We found differences in content areas between diagnostic and procedural specialties (Figure 1). Procedural specialties more commonly were directed toward career planning (P=.02, 5% vs 2%) and scholarly activity (P=.0019, 5% vs 1%), compared to diagnostic specialties, which more commonly focused on medical knowledge (P=.0376, 16% vs 21%) and practice-based and lifelong learning (P=.0021, 0% vs 3%).
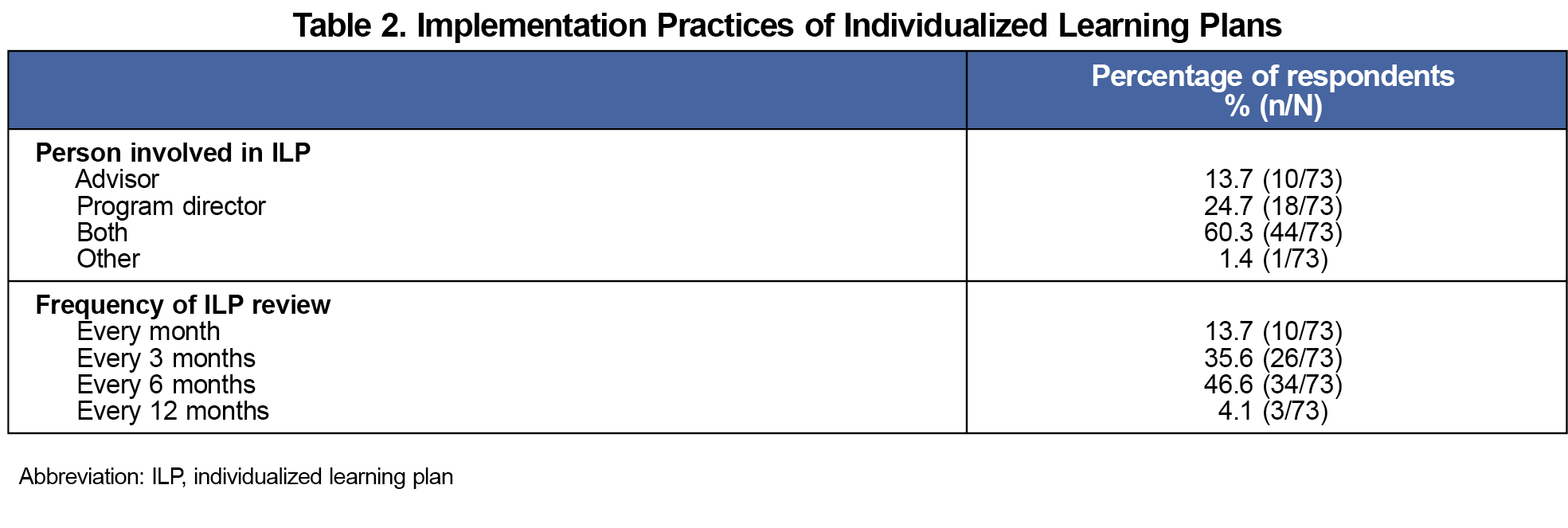
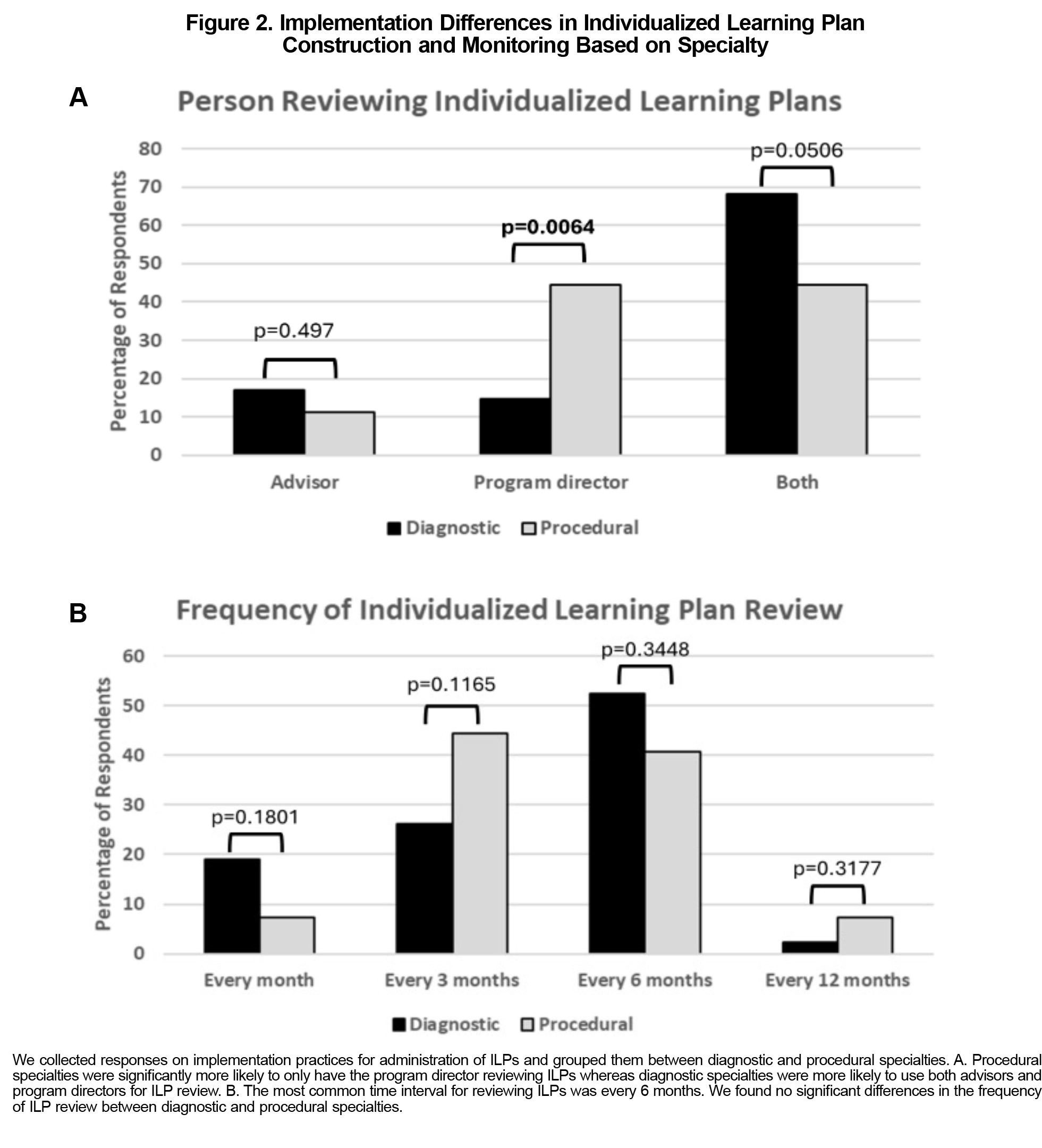
Both advisors and PDs were most involved in reviewing completed ILPs with learners (61.1%; Table 2). Reviewing ILPs occurred most frequently every 6 months (46.6%), though 35.6% reviewed every 3 months, and 13.7% did so monthly. Procedural specialties were more likely to have only the PD review ILPs than diagnostic specialties (Figure 2A, P=.0064, 44.4% vs 14.6%). We found no difference in the frequency of ILP review between specialties (Figure 2B).
The most identified content areas for ILPs were medical knowledge, clinical skills, professionalism, clinical reasoning, and interpersonal/communication skills. We found statistically significant differences between diagnostic and procedural specialties in the percentage of ILPs that focused on career planning, scholarly activity, and practice-based learning and improvement (PBLI). These findings may reflect differences in learners’ needs within diagnostic and procedural training programs, and they may reflect differences in the comfort of mentoring faculty. These differences also may reflect differences in what advisors and curricula focus on in various specialties and could provide information for programs to assess whether other content areas need increased attention. A larger percentage of ILPs focused on PBLI within diagnostic specialties, which may reflect how these content areas are (or are not) incorporated within the curriculum.
ACGME does not provide detailed guidance on how to implement ILPs.8 Specialty-specific requirements provide minimal additional details, with family medicine requiring use of the semiannual review to develop ILPs.9 Our literature search found a gap in describing ILP content areas.10-11 Understanding the why behind the content areas for learner ILPs could help health systems support their programs’ optimal use of ILPs and better meet ACGME’s intention behind the ILP requirement.
Our health system’s GME team will incorporate these results into our annual needs assessment regarding programming. Ensuring that our faculty physicians have adequate resources for teaching and mentoring PBLI will be a priority for our diagnostic programs. We also have an opportunity to gather additional information about the background training and comfort level that faculty members have related to ILP development to ensure consistent baseline competency, regardless of the program, within our health system.
Our study used a convenience sample, and limitations include the possibility that respondents were not fully representative of OhioHealth graduate medical education. Our study also was conducted within one regional health system and may not be generalizable to other health systems. Our IRB did not permit us to collect information about residents’ specific specialties, which limited our ability to draw more specific conclusions.
Next steps include identifying faculty comfort and skill in mentoring ILP development and providing any necessary support in those domains. Examining the reason for choosing identified content areas would provide information that could guide learner- and faculty-level training. Further study could include identifying trends in the content areas of learners across different postgraduate years. Finally, studying ILP content from other health systems would add to the literature.
This study described the content of ILPs across a range of residency and fellowship specialties within a large multihospital graduate medical education system. We found differences in ILPs’ focus between procedural and diagnostic specialties, with procedural specialties prioritizing career planning and scholarly activity, and diagnostic specialties emphasizing medical knowledge and PBLI. These insights underscore the need for faculty development and resource allocation tailored to the distinct needs of procedural and diagnostic specialties. Further research is needed to explore the long-term impact of ILPs on resident and fellow performance and patient care.
Acknowledgments
The authors acknowledge John Elliott for his help in IRB approval and creation and deployment of our survey in RedCap.
Presentation
This study was previously presented as:
Ringwald B, Middleton J, Niedermeyer V. Implementation of Individualized Learning Plans Across a Large Midwestern Healthcare System Department of Graduate Medical Education. Accreditation Council for Graduate Medical Education Annual Meeting, 2025.
References
- Wheat S, Cole S. Individualized learning plans: who, what, when, where, why, and how? Ann Fam Med. 2023;21(6):560-562. doi:10.1370/afm.3062
- Getto LP, Drake J, Kern A, Fredette J. Implementation of a monthly individualized learning plan with emergency medicine residents. AEM Educ Train. 2021;5(4):e10710. doi:10.1002/aet2.10710
- Svrakic M, Bent JP III. Individualized learning plan (ILP) is an effective tool in assessing achievement of otology-related subcompetency milestones. Otol Neurotol. 2018;39(7):816-822. doi:10.1097/MAO.0000000000001855
- Lockspeiser TM, Kaul P. Using individualized learning plans to facilitate learner-centered teaching. J Pediatr Adolesc Gynecol. 2016;29(3):214-217. doi:10.1016/j.jpag.2015.10.020
- OhioHealth. Medical education. Accessed November 19, 2024. https://www.ohiohealth.com/medical-education
- Artino AR Jr, La Rochelle JS, Dezee KJ, Gehlbach H. Developing questionnaires for educational research: AMEE guide no. 87. Med Teach. 2014;36(6):463-474. doi:10.3109/0142159X.2014.889814
- Edgar L, Roberts S, Holmboe E. Milestones 2.0: A step forward. J Grad Med Educ. 2018;10(3):367-369. doi:10.4300/JGME-D-18-00372.1
- Accreditation Council for Medical Education. ACGME Common Program Requirements (Residency). 2023. Accessed December 5, 2024.
- Accreditation Council for Medical Education. ACGME Program Requirements for Graduate Medical Education in Family Medicine. 2024. Accessed December 5, 2024.
- Li ST, Paterniti DA, Tancredi DJ, Co JP, West DC. Is residents’ progress on individualized learning plans related to the type of learning goal set? Acad Med. 2011;86(10):1,293-1,299. doi:10.1097/ACM.0b013e31822be22b
- Gifford KA, Thoreson L, Burke AE, et al. Describing overarching curricular goals for individualized education. Teach Learn Med. 2021;33(3):282-291. doi:10.1080/10401334.2020.1835665
Lead Author
Bryce A. Ringwald, MD
Affiliations: Family Medicine Residency Program, OhioHealth Riverside Methodist Hospital, Columbus, OH
Co-Authors
Jennifer L. Middleton, MD, MPH - Family Medicine Residency Program, OhioHealth Riverside Methodist Hospital, Columbus, OH
Valerie Niedermier, MD - OhioHealth Graduate Medical Education System, Columbus, OH | Family Medicine Residency Program, OhioHealth Grant Medical Center, Columbus, OH
Corresponding Author
Bryce A. Ringwald, MD
Correspondence: Family Medicine Residency Program, OhioHealth Riverside Methodist Hospital, Columbus, OH
Email: bryceringwald@gmail.com
Fetching other articles... 
Loading the comment form...
Submitting your comment...

There are no comments for this article.